




 |
 |
| J Korean Med Assoc > Volume 50(8); 2007 > Article |
Abstract
Until recently, the fracture was regarded as the dominant element of high energy injuries, probably because trauma and orthopedic training was, by tradition, centered on the care of bone and joint injuries. Nowadays, however, orthopedic and trauma surgeons consider soft tissue injuries to be the most important component of high-energy trauma. High energy injuries such as polytrauma that may lead to dysfunction or failure of remote organs and vital systems, open fractures indicating a communication between the fracture and the external environment, pelvic fractures comprised of pelvic ring injuries and acetabular fractures are mostly associated with soft tissue injuries and are different from low energy injuries in their mechanism. Treatments of high energy injuries are more difficult than those of low energy injuries. Meticulous care should be taken to evaluate complications such as compartment syndrome, deep vein thrombosis, pulmonary embolism, and fat embolism, which tend to be easily neglected. Fractures with soft tissue injuries that are mostly high energy injuries need focusing on the patient as a whole and comprehensive approach. Close observations to establish early diagnosis of complications and to take timely, appropriate measures are also necessary.
References
1. Behrman SW, Fabian TC, Kudsk KA, Taylor JC. Improved outcome with femur fractures: early vs. delayed fixation. J Trauma 1990;30:792-797.
2. Bone LB, Johnson KD, Weigelt J, Scheinberg R. Early versus delayed stabilization of femoral fractures. A prospective randomized study. J Bone Joint Surg Am 1989;71:336-340.
3. Bone LB, Johnson KD, Weigelt J, Scheinberg R. Early versus delayed stabilization of femoral fractures: a prospective randomized study. 1989. Clin Orthop Relat Res 2004;11-16.
4. Goris RJ, Gimbrere JS, van Niekerk JL, Schoots FJ, Booy LH. Early osteosynthesis and prophylactic mechanical ventilation in the multitrauma patient. J Trauma 1982;22:895-903.
5. Johnson KD, Cadambi A, Seibert GB. Incidence of adult respiratory distress syndrome in patients with multiple musculoskeletal injuries: effect of early operative stabilization of fractures. J Trauma 1985;25:375-384.
6. Riska EB, von Bonsdorff H, Hakkinen S, Jaroma H, Kiviluoto O, Paavilainen T. Prevention of fat embolism by early internal fixation of fractures in patients with multiple injuries. Injury 1976;8:110-116.
7. Ruedi T, Wolff G. Prevention of post-traumatic complications through immediate therapy in patients with multiple injuries and fractures. Helv Chir Acta 1975;42:507-512.
8. Lange RH, Bach AW, Hansen ST, Johansen KH. Open tibial fractures with associated vascular injuries: prognosis for limb salvage. J Trauma 1985;25:203-208.
9. Gustilo RB, Anderson JT. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: retrospective and prospective analyses. J Bone Joint Surg Am 1976;58:453-458.
10. Gustilo RB, Mendoza RM, Williams DN. Problems in the management of type III (severe) open fractures: a new classification of type III open fractures. J Trauma 1984;24:742-746.
11. Court-Brown CM, McQueen MM, Quaba AA, Christie J. Locked intramedullary nailing of open tibial fractures. J Bone Joint Surg Br 1991;73:959-964.
12. Court-Brown CM, Wheelwright EF, Christie J, McQueen MM. External fixation for type III open tibial fractures. J Bone Joint Surg Br 1990;72:801-804.
13. Okike K, Bhattacharyya T. Trends in the management of open fractures. A critical analysis. J Bone Joint Surg Am 2006;88:2739-2748.
14. Stewart DG, Kay RM, Skaggs DL. Open fractures in children. Principles of evaluation and management. J Bone Joint Surg Am 2005;87:2784-2798.
15. Worlock P, Slack R, Harvey L, Mawhinney R. The prevention of infection in open fractures: an experimental study of the effect of fracture stability. Injury 1994;25:31-38.
16. Francel TJ, Vander Kolk CA, Hoopes JE, Manson PN, Yaremchuk MJ. Microvascular soft-tissue transplantation for reconstruction of acute open tibial fractures: timing of coverage and long-term functional results. Plast Reconstr Surg 1992;89:478-487.
17. Gorman PW, Barnes CL, Fischer TJ, McAndrew MP, Moore MM. Soft-tissue reconstruction in severe lower extremity trauma. A review. Clin Orthop Relat Res 1989;57-64.
18. Sanders R, Swiontkowski M, Nunley J, Spiegel P. The management of fractures with soft-tissue disruptions. J Bone Joint Surg Am 1993;75:778-789.
19. Small JO, Mollan RA. Management of the soft tissues in open tibial fractures. Br J Plast Surg 1992;45:571-577.
20. Seligson D, Ostermann PA, Henry SL, Wolley T. The management of open fractures associated with arterial injury requiring vascular repair. J Trauma 1994;37:938-940.
21. Gregory RT, Gould RJ, Peclet M, Wagner JS, Gilbert DA, Wheeler JR, Snyder SO, Gayle RG, Schwab CW. The mangled extremity syndrome (M.E.S.): a severity grading system for multisystem injury of the extremity. J Trauma 1985;25:1147-1150.
22. Howe HR, Poole GV, Hansen KJ, Clark T, Plonk GW, Koman LA, Pennell TC. Salvage of lower extremities following combined orthopedic and vascular trauma. A predictive salvage index. Am Surg 1987;53:205-208.
23. Johansen K, Daines M, Howey T, Helfet D, Hansen ST. Objective criteria accurately predict amputation following lower extremity trauma. J Trauma 1990;30:568-572.
24. Russell WL, Sailors DM, Whittle TB, Fisher DF, Burns RP. Limb salvage versus traumatic amputation. A decision based on a seven-part predictive index. Ann Surg 1991;213:473-480. discussion 80-81.
25. Trunkey DD, Chapman MW, Lim RC, Dunphy JE. Management of pelvic fractures in blunt trauma injury. J Trauma 1974;14:912-923.
26. Schopfer A, DiAngelo D, Hearn T, Powell J, Tile M. Biome chanical comparison of methods of fixation of isolated osteotomies of the posterior acetabular column. Int Orthop 1994;18:96-101.
27. Hak DJ, Olson SA, Matta JM. Diagnosis and management of closed internal degloving injuries associated with pelvic and acetabular fractures: the Morel-Lavallee lesion. J Trauma 1997;42:1046-1051.
28. Pennal GF, Tile M, Waddell JP, Garside H. Pelvic disruption: assessment and classification. Clin Orthop Relat Res 1980;12-21.
29. Tile M. Acute Pelvic Fractures: I. Causation and Classification. J Am Acad Orthop Surg 1996;4:143-151.
30. Hanson PB, Milne JC, Chapman MW. Open fractures of the pelvis. Review of 43 cases. J Bone Joint Surg Br 1991;73:325-329.
31. Rothenberger D, Velasco R, Strate R, Fischer RP, Perry JF Jr. Open pelvic fracture: a lethal injury. J Trauma 1978;18:184-187.
32. Maull KI, Sachatello CR, Ernst CB. The deep perineal laceration-an injury frequently associated with open pelvic fractures: a need for aggressive surgical management. A report of 12 cases and review of the literature. J Trauma 1977;17:685-696.
33. Oosterlee J, McGeehan DF, Robbs JV. Prevention of septic complications in massive pelvic-perineal injuries. Case reports. S Afr Med J 1984;66:147-150.
34. Richardson JD, Harty J, Amin M, Flint LM. Open pelvic fractures. J Trauma 1982;22:533-538.
35. Shrier I, Magder S. Pressure-flow relationships in in vitro model of compartment syndrome. J Appl Physiol 1995;79:214-221.
36. Matsen FA 3rd, Winquist RA, Krugmire RB Jr. Diagnosis and management of compartmental syndromes. J Bone Joint Surg Am 1980;62:286-291.
37. Mubarak SJ, Owen CA. Double-incision fasciotomy of the leg for decompression in compartment syndromes. J Bone Joint Surg Am 1977;59:184-187.
38. Montgomery KD, Geerts WH, Potter HG, Helfet DL. Thromboembolic complications in patients with pelvic trauma. Clin Orthop Relat Res 1996;68-87.
39. Rabinov K, Paulin S. Roentgen diagnosis of venous thrombosis in the leg. Arch Surg 1972;104:134-144.
40. Erdmann MW, Richardson J, Templeton J. Os calcis fractures: a randomized trial comparing conservative treatment with impulse compression of the foot. Injury 1992;23:305-307.
41. Palmer AJ, Koppenhagen K, Kirchhof B, Weber U, Bergemann R. Efficacy and safety of low molecular weight heparin, unfractionated heparin and warfarin for thrombo-embolism prophylaxis in orthopaedic surgery: a meta-analysis of randomised clinical trials. Haemostasis 1997;27:75-84.
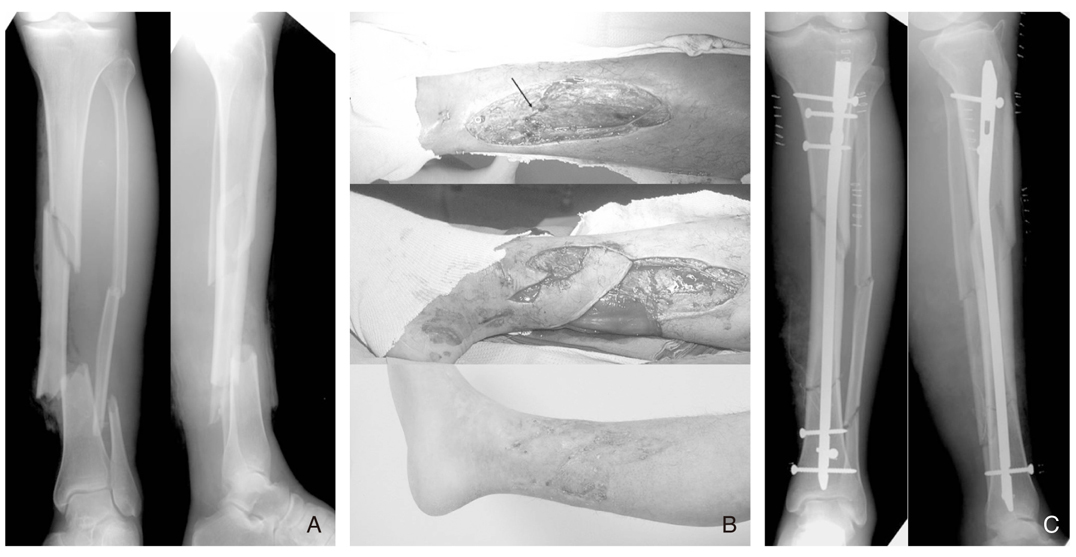
Figure 1
Type III B open tibial and fibular fracture.
A) Preoperative radiographs showed segmental fractures of the tibia and fibula.
B) Uncovered fracture site(arrow) of open wound was covered with rotational fasciocutaneous flap and the remnant wound left open was closed later with skin grafts.
C) Immediate postoperative radiographs demonstrated a good alignment of the tibia after internal fixation with intramedullary nail.
- TOOLS
-
- Share :
-





-
METRICS

-
- 1 Crossref
- Scopus
- 1,271 View
- 6 Download
-

-
Related articles in
J Korean Med Assoc -
Causes and symptoms of varicose veins2022 April;65(4)
Stricture and Mass under Colonoscopy2000 June;43(6)
Ethical Issues Related to Tissue Banking2001 November;44(11)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
