



 |
 |
| J Korean Med Assoc > Volume 51(1); 2008 > Article |
Abstract
Stereotactic Body Radiation Therapy (SBRT) is extracranial stereotactic radiosurgery or stereotactic radiation therapy, a newly emerging radiotherapy treatment method to deliver a high dose of radiation to the target, utilizing either a single dose or a small number of fractions with a high degree of precision within the body. The ability to deliver a single or a few fractions of high-dose ionizing radiation with a high targeting accuracy and rapid dose falloff gradients encompassing tumors with a patient provides the basis for the development of SBRT. A few fractions, the use of fiducial as a marker, image guidance and multiple radiation beam, and gating through a skin marker are unique technologies as compared to the conventional fractionated radiotherapy. The most common sites for these treatments are lung and liver, which are considered to parallel organs at risk. Recently, it was confirmed that prostate, spinal/paraspinal, head and neck, and pancreas tumors could be new candidates for these novel treatments. The preliminary reports show promising results with a relatively low complication rate. This article provides an overview of SBRT, the indication, descriptions of method including radiation dose and fraction size, the clinical data of lung and liver tumor, and discussions on potential areas of future investigations.
References
1. Nagata Y, Matsuo Y, Takayama K, Norkhisa Y, Mizowaki T, Mitumori M, Shibuya K, Yano S, Narita Y, Hiraoka M. Current status of stereotactic body radiotherapy for lung cancer. Int J Clin Oncol 2007;12:3-7.
2. D'Souza WD, Nazareth DP, Zhang B, Ewyoung C, Suntharalingam M, Kwok Y, Yu CX, Regine WF. The use of gated and 4D CT imaging in planning for stereotactic body radiation therapy. Med Dosi 2007;32:92-101.
3. Kavanagh BD, Scheftera TE, Wersall PJ. Liver, renal and retroperitoneal tumors:stereotactic radiotherapy. Front Radiat Ther Oncol 2007;40:415-426.
4. Fowler JF, Tome WA, Welsh JS. In: Kavanagh BD, Tirnmerman RD, editor. The radiobiology of stereotactic body radiation therapy (SBRT). Stereotactic Body Radiation Therapy 2004;1st ed. Philadelphia: Lippincott Williams & Wilkins. 7-14.
5. Uematsu M, Shioda A, Suda A, Fukui T, Ozeki Y, Wong JR, Kusano S. Computed tomography-guided frameless stereotactic radiotherapy for stage I non-small-cell lung cancer: a 5-year experience. Int J Radiat Oncol Biol Phys 2001;51:666-670.
6. Nagata Y, Negoro Y, Aoki T, Mizowaki T, Takayama K, Kokubo M, Araki N, Mitsumori M, Sasai K, Shibamoto Y, Koga S, Yano S, Hiraoka M. Clinical outcomes of 3D conformal hypofractionated single high-dose radiotherapy for one or two lung tumors using a stereotactic body frame. Int J Radiat Oncol Biol Phys 2002;52:1041-1046.
7. Hara R, Itami J, Kondo T, Aruga T, Abe Y, Ito M, Fuse M, Shinohara D, Nagaoka T, Kobiki T. Stereotactic single high dose irradiation of lung tumors under respiratory gating. Radiother Oncol 2002;63:159-163.
8. Onishi H, Araki T, Shirato H, Nagata Y, Hiraoka M, Gomi K, Yamashita T, Niibe Y, Karasawa K, Hayakawa K, Takai Y, Kimura T, Hirokawa Y, Takeda A, Ouchi A, Hareyama M, Kokubo M, Hara R, Itami J, Yamada K. Stereotactic hypofractionated high-dose irradiation for stage I non-small cell lung carcinoma: clinical outcomes in 245 subjects in a Japanese multiinstitutional study. Cancer 2004;101:1623-1631.
9. Lee SW, Choi EK, Park HJ, Ahn SD, Kim JH, Kim KJ, Yoon SM, Kim YS, Yi BY. Stereotactic body frame based fractionated radiosurgery on consecutive days for primary or metastatic tumors in the lung. Lung Cancer 2003;40:309-315.
10. Nesbitt JC, Putnam JB Jr, Walsh GL, Roth JA, Mountain CF. Survival in early stage non-small cell lung cancer. Ann Thorac Surg 1995;60:466-472.
11. Fry WA, Menck HR, Winchester DP. The National cancer data base report on lung cancer. Cancer 1996;77:1947-1955.
12. Wingo PA, Tong T, Bolden S. Cancer statistics, 1995. CA Cancer J Clin 1995;45:8-30.
13. Blomgren H, Lax I, Naslund I, Svanstrom R. Stereotactic high dose fraction radiation therapy of extracranial tumors using an accelerator. Acta Oncolgica 1995;34:861-870.
14. Nakagawa K, Aoki Y, Tago M, Terahara A, Ohtomo K. Megavoltage CT-assisted stereotactic radiosurgery for thoracic tumors: original research in the treatment of thoracic neoplasms. Int J Radiat Oncol Biol Phys 2000;48:449-457.
15. Wulf J, Hädinger U, Oppitz U, Thiele W, Ness-Dourdoumas R, Flentje M. Stereotactic radiotherapy of targets in the lung and liver. Strahlenther Onkol 2001;177:645-655.
16. Timmerman R, Papiez L, McGarry R, Likes L, DesRosiers C, Frost S, Williams M. Extracranial stereotactic radioablation: results of a phase I study in medically inoperable stage I non-small cell lung cancer. Chest 2003;124:1946-1955.
17. Hof H, Herfarth KK, Münter M, Hoess A, Motsch J, Wannenmacher M, Debus JJ. Stereotactic single dose radiotherapy of stage I non-small-cell lung cancer. Int J Radiat Oncol Biol Phys 2003;56:335-341.
18. Hawkins MA, Dawson LA. Radiation therapy for hepatocellular carcinoma from palliation to cure. Cancer 2006;15:1653-1663.
19. Blomgren H, Lax I, Näslund I, Svanstörm R. Stereotactic high dose fraction radiation therapy of extracranial tumors using an accelerator. Clinical experience of the first thirty one patients. Acta Oncol 1995;34:861-870.
20. Lunsford LD, Flickinger JC, Larson D. Radiosurgery for tumors in the body: clinical experience using a new method. J Radiosurg 1998;1:63-74.
21. Herfarth KK, Debus J, Lohr F, Bahner ML, Rhein B, Fritz P, Höss A, Schlegel W, Wannenmacher MF. Stereotactic single-dose radiation therapy of liver tumors: results of a phase I/II trial. J Clin Oncol 2001;19:164-170.
Figure 1
Real time tumor-tracking system in SBRT using the detector (A) on the ceiling and sensors (B) of the chest wall enables detecting and correcting for tumors that move with respiration. The lung or liver tumor can be treated with smaller irradiated normal volume under the adoption of this system.
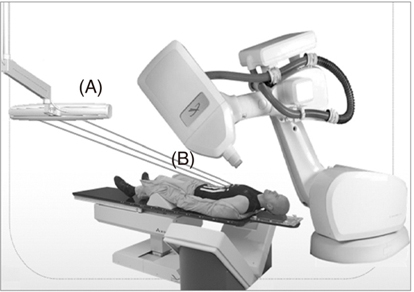
Figure 2
In SBRT, internal fiducial markers can be used for more accuracy during SBRT. Gold strict fiducial (A) and flexible helical coil markers (C). The fiducials could be placed in or around tumor under fluoroscopy (B), CT or sono.
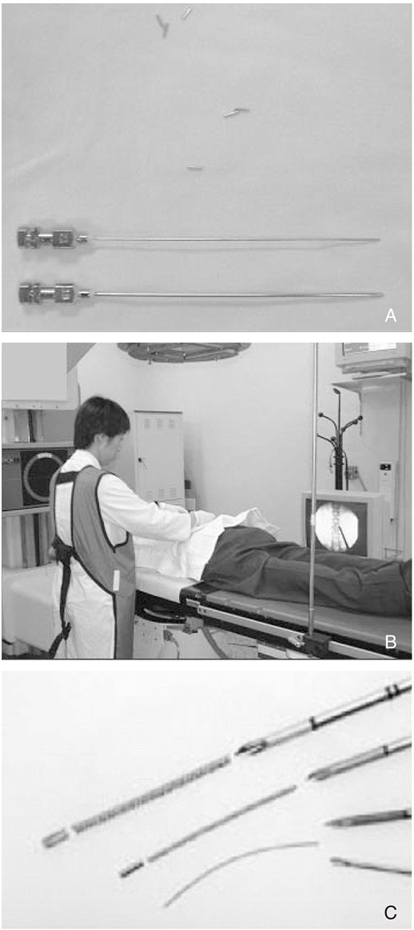
Figure 3
This is example of a highly conformal plan in SBRT. Red line (A, B, C) represents the target volume. Green lines (D) mean the multi-direction of radiation beams. The patient was malignant histiocytoma and treated with 26Gy in 2 fraction (equivalent to 83 Gy > in 2Gy per fraction). At 1 year after completion of SBRT, showing complete response and continued local control at 3 year.
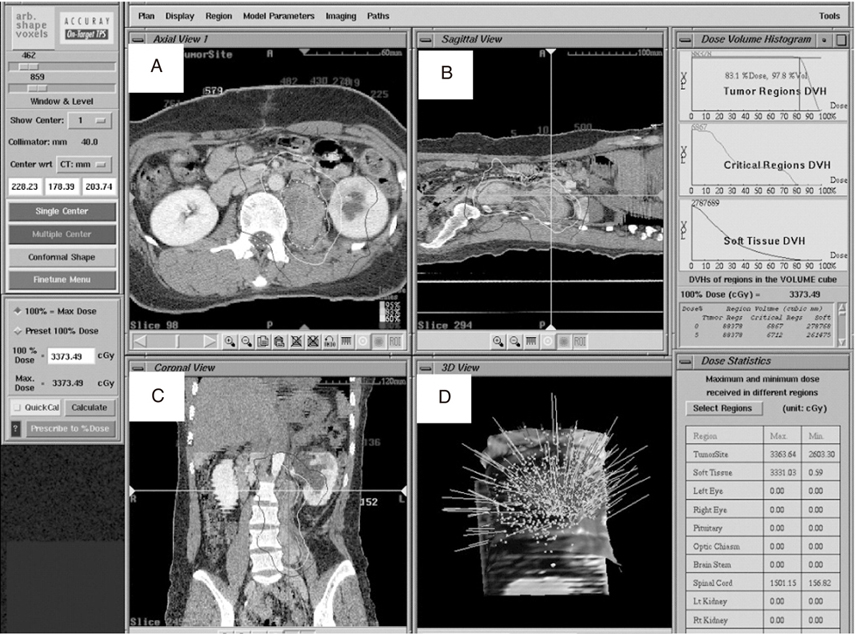
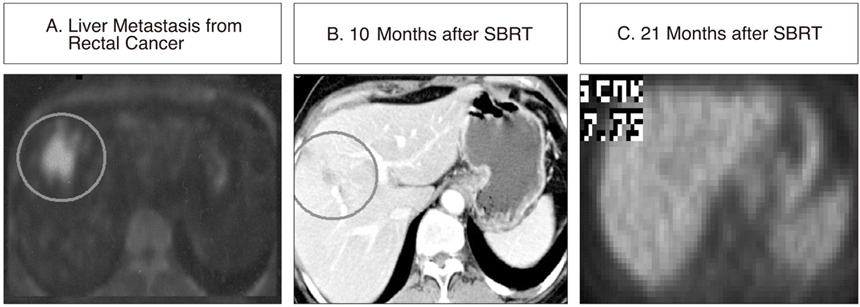
Figure 4
(A) is PET/CT images for a patient with liver metastasis from rectal cancer. (B) is showing small lesion on CT 10 months after SBRT, which is difficult to distinguish between residual tumor or radiation reaction. PET or PET/CT would be helpful for differential diagnosis. (C) is showing continued complete response on PET at 21 months.
- TOOLS
-
- Share :
-





-
METRICS

-
- 1 Crossref
- Scopus
- 1,171 View
- 7 Download
-

-
Related articles in
J Korean Med Assoc -
Fractionated Stereotactic Radiation Therapy1997 January;40(1)
Current Concepts in Androgen Deprivation Therapy2004 May;47(5)
Climacteric Symptoms and Hormone Therapy2006 January;49(1)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
