










 |
 |
| J Korean Med Assoc > Volume 51(10); 2008 > Article |
Abstract
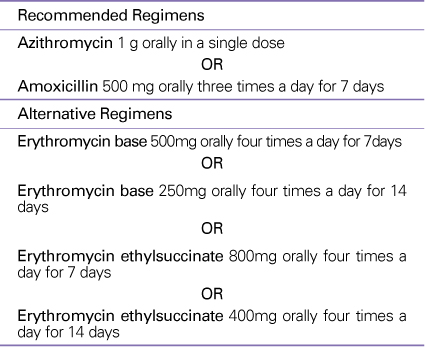
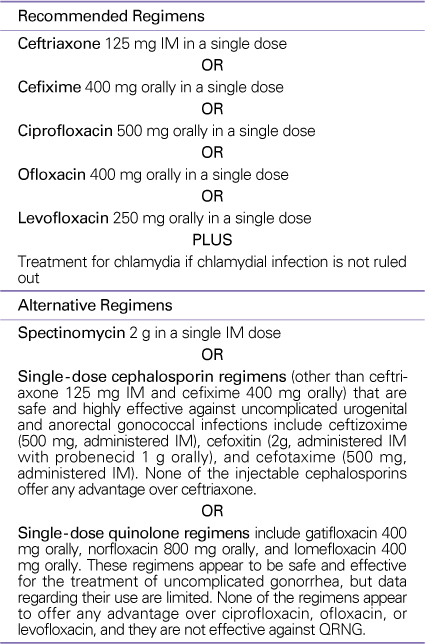
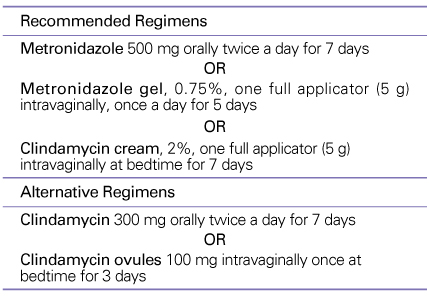
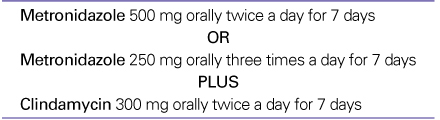
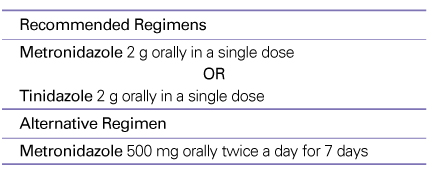
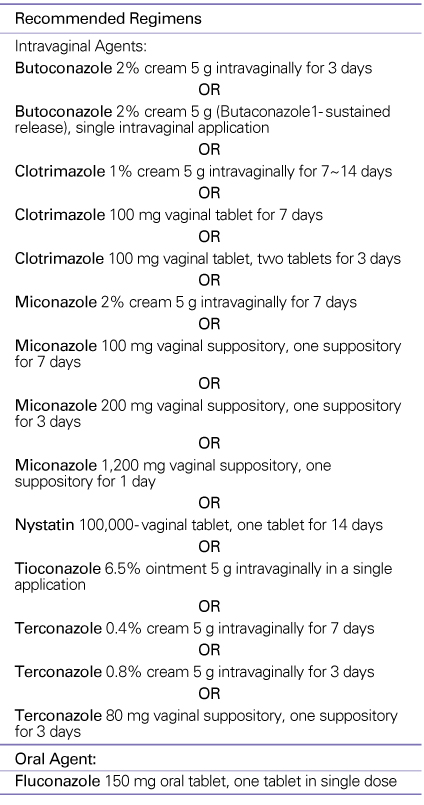
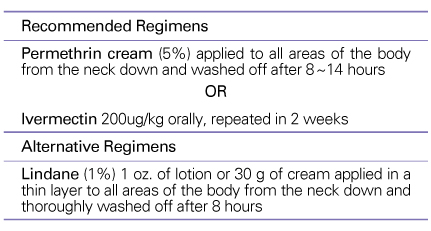
Sexually transmitted diseases (STDs) are the most common group of identifiable infectious diseases in many countries. Adolescents and young adults (15-24 years old) comprise only 25% of the sexually active population but represent almost 50% of all newly acquired STDs. In a law for prevention of infectious diseases in Korea, STDs include syphilis, gonorrhea, chancroid, nongonococcal urethritis, clamydial infection, genital herpes, and genital wart. Bacterial vaginosis, trichomoniasis, candidiasis, amebiasis, scabies, phthiriasis, granuloma inguinale, AIDS, and high risk human papilloma virus are also included in the STDs. Individuals infected with STDs are 5-10 times more likely than uninfected individuals to acquire or transmit HIV through sexual contacts. Their control is important considering the high incidences of acute infections, complications, and sequelae, their socioeconomic impact, and their role in increasing transmission of the HIV. The purpose of this paper is to summarize the treatment and management of STDs on the basis of Centers for Disease Control and Prevention treatment guidelines for sexually transmitted diseases published in 2006.
References
1. UNAIDS. Force for change: World AIDS Campaign with young people. UNAIDS 1998 theme. AIDS Anal Afr 1998;8:8-9.
2. Hillis SD, Wasserheit JN. Screening for Chlamydia-A Key to the prevention of pelvic inflammatory disease. N Engl J Med 1996;334:1399-1401.
3. Centers for Disease Control. Sexually transmitted disease treatment guidelines, 2006. MMWR 2006;55:11.
Table 11
Oral desensitization protocol for patients with a positive skin test*
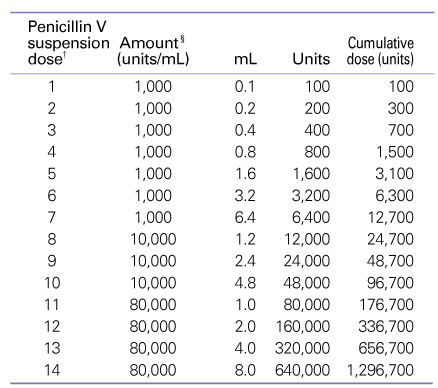
Observation period: 30 minutes before parenteral administration of penicillin
*Reprinted with permission from the New England Journal of Medicine.
SOURCE: Wendel GO Jr. Stark BJ, Jamison RB, Melina RD, Sullivan TJ. Penicillin allergy and desensitization in serious infections during pregnancy. N Engl J Med 1985; 312; 1229-1232.
†Interval between doses: 15 minutes; elapsed time: 3 hours and 45 minutes; and cumulative dose: 1.3 million units.
§The specific amount of drug was diluted in approximately 30mL of water amd then administered orally.
- TOOLS
-
- Share :
-





-
METRICS

-
Related articles in
J Korean Med Assoc -
Prevalence and management of hypertension in Korean adults2022 October;65(10)
Prevention and management of urinary stone2020 November;63(11)
Diagnosis and management of Kawasaki disease2020 July;63(7)
Understanding and Management of Occupational Diseases1997 May;40(5)
Diagnosis and Management of Facial Nerve Paralysis1999 May;42(5)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
