



 |
 |
| J Korean Med Assoc > Volume 52(4); 2009 > Article |
Abstract
As, until now, many studies have failed to establish the clinical effect of numerous neuroprotectives, antithrombotic therapy must be emphasized as one of critical options among limited treatment strategies in acute ischemic stroke. Based on the accumulating evidences that platelets and coagulating proteins play an important role in the thrombus formation, antiplatelets and anticoagulants are served as antithrombotics. Recently, major advances have been made in understanding the effects of antiplatelets and anticoagulants. Large randomized clinical trials have highlighted the effectiveness and safety of early and continuous antiplatelet therapy in reducing atherothrombotic stroke recurrence. Urgent anticoagulation has been used often to prevent early recurrent stroke and to improve neurological outcomes, however, its formal use in acute stroke has been the subject of debate even in cardioembolic stroke. That's because anticoagulants also increase the risk of fatal or disabling intracranial hemorrhage and it is difficult to monitor proper anticoagulation. Although early administration of anticoagulants should be considered to prevent the secondary injury and the propagation of thrombosis in patients with atherothrombotic stroke, more evidences are needed especially in patients with infractions secondary to large artery thrombosis or cardioembolism. This review discusses recent advances related to antithrombotic strategies and putative neuroprotectives.
References
1. Coull BM, Williams LS, Goldstein LB, Meschia JF, Heitzman D, Chaturvedi S, Johnston KC, Starkman S, Morgenstern LB, Wilterdink JL, Levine SR, Saver JL. Anticoagulants and antiplatelet agents in acute ischemic stroke: report of the Joint Stroke Guideline Development Committee of the American Academy of Neurology and the American Stroke Association (a division of the American Heart Association). Neurology 2002;59:13-22.
2. Adams HP Jr, del Zoppo G, Alberts MJ, Bhatt DL, Brass L, Furlan A, Grubb RL, Higashida RT, Jauch EC, Kidwell C, Lyden PD, Morgenstern LB, Qureshi AI, Rosenwasser RH, Scott PA, Wijdicks EF. Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: the American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Stroke 2007;38:1655-1711.
3. Guidelines for management of ischaemic stroke and transient ischaemic attack 2008. Cerebrovasc Dis 2008;25:457-507.
4. Albers GW, Amarenco P, Easton JD, Sacco RL, Teal P. Antithrombotic and thrombolytic therapy for ischemic stroke: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008;133:6S. 630S-669S.
5. Sandercock PA, Counsell C, Gubitz GJ, Tseng MC. Antiplatelet therapy for acute ischaemic stroke. Cochrane Database Syst Rev 2008;CD000029.
6. CAST: randomised placebo-controlled trial of early aspirin use in 20,000 patients with acute ischaemic stroke. CAST (Chinese Acute Stroke Trial) Collaborative Group. Lancet 1997;349:1641-1649.
7. International Stroke Trial Collaborative Group. The International Stroke Trial (IST): a randomised trial of aspirin, subcutaneous heparin, both, or neither among 19435 patients with acute ischaemic stroke. Lancet 1997;349:1569-1581.
8. Chen ZM, Sandercock P, Pan HC, Counsell C, Collins R, Liu LS, Xie JX, Warlow C, Peto R. On behalf of the CAST and IST collaborative groups. Indications for early aspirin use in acute ischemic stroke : A combined analysis of 40,000 randomized patients from the chinese acute stroke trial and the international stroke trial. Stroke 2000;31:1240-1249.
9. Hankey GJ, Warlow CP. Treatment and secondary prevention of stroke: evidence, costs, and effects on individuals and populations. Lancet 1999;354:1457-1463.
10. Wardlaw JM. Overview of Cochrane thrombolysis meta-analysis. Neurology 2001;57(S2):S69-S76.
11. Emergency administration of abciximab for treatment of patients with acute ischemic stroke: results of a randomized phase 2 trial. Stroke 2005;36:880-890.
12. Adams HP Jr, Effron MB, Torner J, Davalos A, Frayne J, Teal P, Leclerc J, Oemar B, Padgett L, Barnathan ES, Hacke W. Emergency administration of abciximab for treatment of patients with acute ischemic stroke: results of an international phase III trial: Abciximab in Emergency Treatment of Stroke Trial (AbESTT-II). Stroke 2008;39:87-99.
13. Kennedy J, Hill MD, Ryckborst KJ, Eliasziw M, Demchuk AM, Buchan AM. Fast assessment of stroke and transient ischaemic attack to prevent early recurrence (FASTER): a randomised controlled pilot trial. Lancet Neurol 2007;6:961-969.
14. Adams HP Jr. Emergent use of anticoagulation for treatment of patients with ischemic stroke. Stroke 2002;33:856-861.
15. Al-Sadat A, Sunbulli M, Chaturvedi S. Use of intravenous heparin by North American neurologists: do the data matter? Stroke 2002;33:1574-1577.
16. Donnan GA, Davis SM. Heparin in stroke: not for most, but the controversy lingers. Stroke 2003;34:232-233.
17. Caplan LR. Resolved: Heparin may be useful in selected patients with brain ischemia. Stroke 2003;34:230-231.
18. Sandercock PA, Counsell C, Kamal AK. Anticoagulants for acute ischaemic stroke. Cochrane Database Syst Rev 2008;CD000024.
19. Saxena R, Lewis S, Berge E, Sandercock PA, Koudstaal PJ. Risk of early death and recurrent stroke and effect of heparin in 3169 patients with acute ischemic stroke and atrial fibrillation in the International Stroke Trial. Stroke 2001;32:2333-2337.
20. Camerlingo M, Salvi P, Belloni G, Gamba T, Cesana BM, Mamoli A. Intravenous heparin started within the first 3 hours after onset of symptoms as a treatment for acute nonlacunar hemispheric cerebral infarctions. Stroke 2005;36:2415-2420.
21. Chamorro A, Busse O, Obach V, Toni D, Sandercock P, Reverter JC, Cervera A, Torres F, Davalos A. The rapid anticoagulation prevents ischemic damage study in acute stroke-final results from the writing committee. Cerebrovasc Dis 2005;19:402-404.
22. Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. N Engl J Med 1995;333:1581-1587.
23. Kay R, Wong KS, Yu YL, Chan YW, Tsoi TH, Ahuja AT, Chan FL, Fong KY, Law CB, Wong A. Low-molecular-weight heparin for the treatment of acute ischemic stroke. N Engl J Med 1995;333:1588-1593.
24. Chamorro A. Heparin in acute ischemic stroke: the case for a new clinical trial. Cerebrovasc Dis 1999;9(S3):16-23.
25. Wong KS, Chen C, Ng PW, Tsoi TH, Li HL, Fong WC, Yeung J, Wong CK, Yip KK, Gao H, Wong HB. Low-molecular-weight heparin compared with aspirin for the treatment of acute ischaemic stroke in Asian patients with large artery occlusive disease: a randomised study. Lancet Neurol 2007;6:407-413.
26. The Publications Committee for the Trial of ORG 10172 in Acute Stroke Treatment (TOAST) Investigators. Low molecular weight heparinoid, ORG 10172 (danaparoid), and outcome after acute ischemic stroke: a randomized controlled trial. JAMA 1998;279:1265-1272.
27. Adams HP Jr, Bendixen BH, Leira E, Chang KC, Davis PH, Woolson RF, Clarke WR, Hansen MD. Antithrombotic treatment of ischemic stroke among patients with occlusion or severe stenosis of the internal carotid artery: A report of the Trial of Org 10172 in Acute Stroke Treatment (TOAST). Neurology 1999;53:122-125.
28. Paciaroni M, Agnelli G, Micheli S, Caso V. Efficacy and safety of anticoagulant treatment in acute cardioembolic stroke: a meta-analysis of randomized controlled trials. Stroke 2007;38:423-430.
29. Berge E, Abdelnoor M, Nakstad PH, Sandset PM. Low molecular-weight heparin versus aspirin in patients with acute ischaemic stroke and atrial fibrillation: a double-blind randomised study. HAEST Study Group. Heparin in Acute Embolic Stroke Trial. Lancet 2000;355:1205-1210.
30. Bath PM, Lindenstrom E, Boysen G, De Deyn P, Friis P, Leys D, Marttila R, Olsson J, O'Neill D, Orgogozo J, Ringelstein B, van der Sande J, Turpie AG. Tinzaparin in acute ischaemic stroke (TAIST): a randomised aspirin-controlled trial. Lancet 2001;358:702-710.
31. Diener HC, Ringelstein EB, von Kummer R, Langohr HD, Bewermeyer H, Landgraf H, Hennerici M, Welzel D, Grave M, Brom J, Weidinger G. Treatment of acute ischemic stroke with the low-molecular-weight heparin certoparin: results of the TOPAS trial. Therapy of Patients With Acute Stroke (TOPAS) Investigators. Stroke 2001;32:22-29.
32. Woessner R, Grauer M, Bianchi O, Mueller M, Moersdorf S, Berlit P, Goertler M, Grotemeyer KH, Sliwka U, Stoll M, Treib J. Treatment with anticoagulants in cerebral events (TRACE). Thromb Haemost 2004;91:690-693.
33. Hallevi H, Albright KC, Martin-Schild S, Barreto AD, Savitz SI, Escobar MA, Gonzales NR, Noser EA, Illoh K, Grotta JC. Anticoagulation after cardioembolic stroke: to bridge or not to bridge? Arch Neurol 2008;65:1169-1173.
34. LaMonte MP, Nash ML, Wang DZ, Woolfenden AR, Schultz J, Hursting MJ, Brown PM. Argatroban anticoagulation in patients with acute ischemic stroke (ARGIS-1): a randomized, placebo-controlled safety study. Stroke 2004;35:1677-1682.
35. Sugg RM, Pary JK, Uchino K, Baraniuk S, Shaltoni HM, Gonzales NR, Mikulik R, Garami Z, Shaw SG, Matherne DE, Moye LA, Alexandrov AV, Grotta JC. Argatroban tPA stroke study: study design and results in the first treated cohort. Arch Neurol 2006;63:1057-1062.
36. Wahlgren NG, Ahmed N. Neuroprotection in cerebral ischaemia: facts and fancies-the need for new approaches. Cerebrovasc Dis 2004;17(S1):153-166.
37. Ginsberg MD. Neuroprotection for ischemic stroke: past, present and future. Neuropharmacology 2008;55:363-389.
38. Lees KR, Zivin JA, Ashwood T, Davalos A, Davis SM, Diener HC, Grotta J, Lyden P, Shuaib A, Hardemark HG, Wasiewski WW. NXY-059 for acute ischemic stroke. N Engl J Med 2006;354:588-600.
39. Shuaib A, Lees KR, Lyden P, Grotta J, Davalos A, Davis SM, Diener HC, Ashwood T, Wasiewski WW, Emeribe U. NXY-059 for the treatment of acute ischemic stroke. N Engl J Med 2007;357:562-571.
40. Effect of a novel free radical scavenger, edaravone (MCI-186), on acute brain infarction. Randomized, placebo-controlled, double-blind study at multicenters. Cerebrovasc Dis 2003;15:222-229.
41. Clark WM, Warach SJ, Pettigrew LC, Gammans RE, Sabounjian LA. Citicoline Stroke Study Group. A randomized dose-response trial of citicoline in acute ischemic stroke patients. Neurology 1997;49:671-678.
42. Clark WM, Wechsler LR, Sabounjian LA, Schwiderski UE. A phase III randomized efficacy trial of 2000 mg citicoline in acute ischemic stroke patients. Neurology 2001;57:1595-1602.
43. Clark WM, Williams BJ, Selzer KA, Zweifler RM, Sabounjian LA, Gammans RE. A randomized efficacy trial of citicoline in patients with acute ischemic stroke. Stroke 1999;30:2592-2597.
44. Davalos A, Castillo J, Alvarez-Sabin J, Secades JJ, Mercadal J, Lopez S, Cobo E, Warach S, Sherman D, Clark WM, Lozano R. Oral citicoline in acute ischemic stroke: an individual patient data pooling analysis of clinical trials. Stroke 2002;33:2850-2857.
Figure 1
Absolute effects in CAST and IST of early use of aspirin in 40,000 randomized patients with suspected acute ischemic stroke. Numbers and percentages of patients with various outcomes during the scheduled treatment period, by allocated treatment: A indicates aspirin; C, control. The percentages are plotted as bars (with the SD of each bar plotted at the top). The difference between aspirin and control is given as the benefit per 1,000, along with its SD and statistical significance (2P). A negative benefit indicates an apparent hazard. *Number of patients who experienced the relevant event and survived (Stroke 2000; 31: 1240-1249).

Table 1
Characteristics of the two large trials of the early use of aspirin in acute ischemic stroke: CAST and IST (Stroke 2000; 31: 1240-1249)
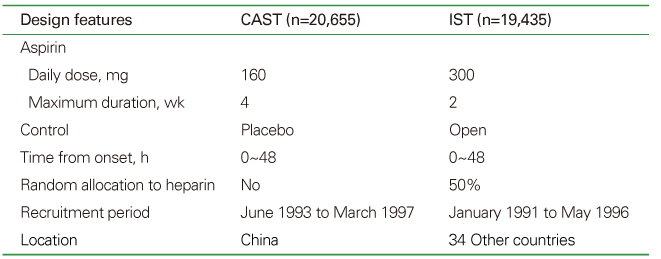
Table 2
Recent trials of emergent lower-molecular-weight heparin and danaparoid for acute ischemic stroke
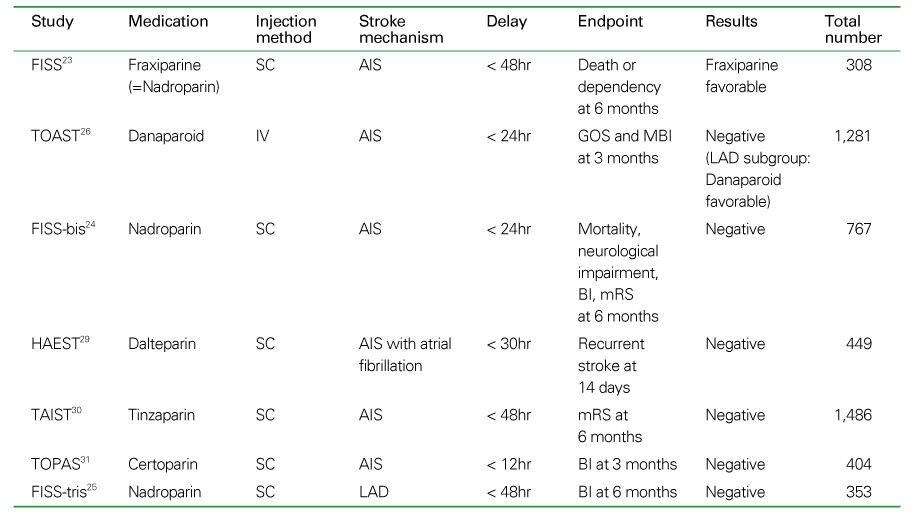
FISS: the Fraxiparine in Ischemic Stroke, Study, TOAST: the Trials of ORG 10172 in Acute Stroke Treatment, TAIST: Tinzaparin in Acute Ischemic Stroke Trial, TOPAS: Therapy Of Patients with Acute Stroke, HAEST: Heparin in Acute Embolic Stroke Trial, GOS: Glasgow Outcome Scale, MBI: Modified Barthel Index, AIS: acute ischemic stroke, LAD: large artery atherosclerotic disease.
- TOOLS
-
- Share :
-





-
METRICS

-
- 0 Crossref
- Scopus
- 1,214 View
- 5 Download
-

-
Related articles in
J Korean Med Assoc -
Reperfusion therapy in acute ischemic stroke2022 July;65(7)
Thrombolytic Treatment of Acute Stroke2009 April;52(4)
Recent advances in thrombolysis of acute ischemic stroke2013 May;56(5)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
