



 |
 |
| J Korean Med Assoc > Volume 55(12); 2012 > Article |
Abstract
Daily low-dose inhaled corticosteroid in preschool children with asthma is recommended to prevent the development of asthma symptom and sign based on many asthma management guidelines. But the retarded growth after long-term steroid inhalation has been concerned. Recently the method of intermittent high-dose (suspension, 1,000 µg, 2 times a day for 7 days) budesonide inhalation when the initial phase to develop the asthma exacerbation was studied to compare the efficacy and safety with daily low-dose budesonide (500 µg) inhalation regimen in preschool children positive with modified asthma predictive index in recurrent wheezer during the study period with 52 weeks. There were no significant difference between two regimen with respect to the frequency of exacerbations, the time to the first exacerbation and to the second exacerbation, and the frequency of treatment failure. The total exposure to budesonide over the period was less in the intermittent high-dose regimen than in the daily low-dose regimen. There were no significant difference in change in height. But the change in height from baseline in intermittent high-dose regimen group was 8.01 cm and in daily low-dose was 7.76 cm. We need the more clinical studies in preschool children with persistent moderate and severe asthma and in various country and nations. It is suggested the intermittent high-dose budesonide inhalation regimen in preschool children with freqeunt wheezing may be a very good alternative to control the allergic inflammation and symptoms of asthma without concerning the adverse effect of steroid.
References
1. Korean Academy of Pediatric Allergy and Respiratory Disease. Asthma management guideline in children 2008;Seoul: Kwangmoon.
2. In: Kim BJ, Kim CW, Rha YH, Park YM, Song DJ, Yem HY, Lee JS, Chang YS, Cho YJ, Cho YS, Han MY, editor. Korean Academy of Asthma, Allergy, and Clinical Immunology. Asthma in children. Asthma and allergic diseases 2012;2nd ed. Seoul: Ryo Moon Gak. 267-278.
3. Ahn HS. In: Ahn HS, editor. Bronchial asthma. Pediatrics 2012;Seoul: MiraeN. 1132-1144.
4. National Heart Lung and Blood Institute. Expert panel report 3 (EPR-3): guidelines for the diagnosis and management of asthma: full report 2007 [Internet] 2007;cited 2012 Nov 22. Bethesda: National Heart, Ling, and Blood Institute. Availabe from: http://www.nhlbi.nih.gov/guidelines/asthma
5. Global Initiative for Asthma. Global strategy for asthma management and prevention 2007;Bethesda: National Institutes of Health, National Heart, Lung, and Blood Institute.
6. Global Initiative for Asthma. GINA report, global strategy for asthma management and prevention 2009 [Internet] 2009;cited 2012 Nov 22. [place unknown]: Global Initiative for Asthma. Available from: http://www.ginasthma.org/Guidelines/guidelines-gina-report-global-strategy-for-asthma-management.html
7. Global Initiative for Asthma. GINA report, global strategy for the diagnosis and management of asthma in children 5 years and younger [Internet] 2009;cited 2012 Nov 22. [place unknown]: Global Initiative for Asthma. Available from: http://www.ginasthma.org/uploads/users/files/GINA_Under5_2009_CorxAug11.pdf
8. Douglas G, Higgins B, Barnes N, Boyter A, Burge S, Cates C, Connett G, Couriel J, Cullinan P, Edwards S, Evans E, Fletcher M, Griffiths C, Heaney L, Boon MH, Holmes S, McArthur R, Nelson-Piercy C, Partridge M, Paton J, Pavord I, Carnegie E, Pinnock H, Qureshi S, Robertson C, Shields M, Warner J, White J. British guideline on the management of asthma: a national clinical guideline. Thorax 2008;63:Suppl 4. iv1-iv121.
9. Nishimuta T, Kondo N, Hamasaki Y, Morikawa A, Nishima S. Japanese guideline for childhood asthma. Allergol Int 2011;60:147-169.
10. Bousquet J, Jeffery PK, Busse WW, Johnson M, Vignola AM. Asthma. From bronchoconstriction to airways inflammation and remodeling. Am J Respir Crit Care Med 2000;161:1720-1745.
11. The Childhood Asthma Management Program Research Group. Long-term effects of budesonide or nedocromil in children with asthma. N Engl J Med 2000;343:1054-1063.
12. Guilbert TW, Morgan WJ, Zeiger RS, Mauger DT, Boehmer SJ, Szefler SJ, Bacharier LB, Lemanske RF Jr, Strunk RC, Allen DB, Bloomberg GR, Heldt G, Krawiec M, Larsen G, Liu AH, Chinchilli VM, Sorkness CA, Taussig LM, Martinez FD. Long-term inhaled corticosteroids in preschool children at high risk for asthma. N Engl J Med 2006;354:1985-1997.
13. Zeiger RS, Mauger D, Bacharier LB, Guilbert TW, Martinez FD, Lemanske RF Jr, Strunk RC, Covar R, Szefler SJ, Boehmer S, Jackson DJ, Sorkness CA, Gern JE, Kelly HW, Friedman NJ, Mellon MH, Schatz M, Morgan WJ, Chinchilli VM, Raissy HH, Bade E, Malka-Rais J, Beigelman A, Taussig LM. CARE Network of the National Heart, Lung, and Blood Institute. Daily or intermittent budesonide in preschool children with recurrent wheezing. N Engl J Med 2011;365:1990-2001.
14. Bisgaard H, Hermansen MN, Loland L, Halkjaer LB, Buchvald F. Intermittent inhaled corticosteroids in infants with episodic wheezing. N Engl J Med 2006;354:1998-2005.
Figure 1
Correlation between pathologic mechanisms and clinical consequences in asthma (From Bousquet J, et al. Am J Respir Crit Care Med 2000;161:1720-1745, according to the Creative Commons License) [10].
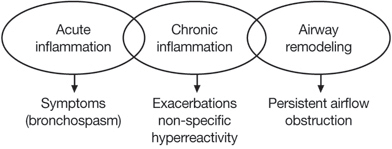
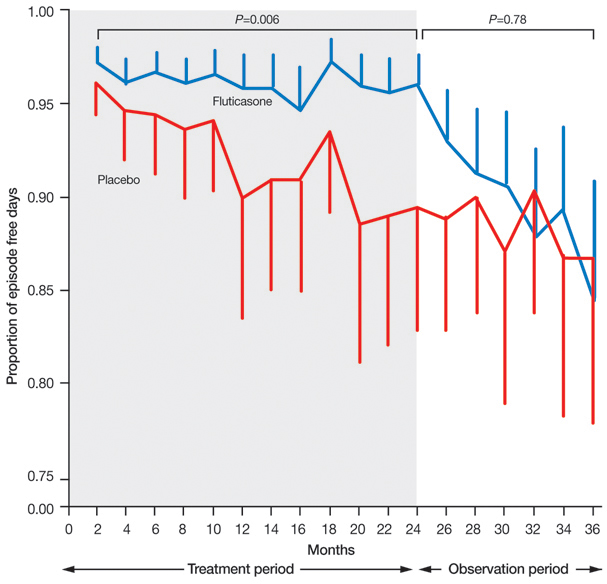
Figure 2
Bimonthly proportion of episode-free days during the two-year treatment period and the observation period. Fluticasone treatment, as compared with placebo, did not increase the proportion of episode-free days during the observation year (86.8% [95% confidence interval {CI}, 81.2 to 90.9] vs. 85.9% [95% CI, 79.9 to 90.3], P=0.78), but during the two-year treatment period (shaded area) it significantly increased the proportion of episode-free days (93.2% [95% CI, 91.1 to 94.9] vs. 88.4% [95% CI, 84.9 to 91.2], P=0.006). The proportions of episode-free days in the fluticasone group and the placebo group were 97% and 96%, respectively, during the first two months of the treatment period; 96% and 89% during the last two months of the treatment period; and 84% and 87% during the last two months of the observation year-results that demonstrate an increase in the frequency of asthma-like symptoms over time. The two study groups were compared by analysis of covariance at each two-month interval. P-values are for the comparison between the groups at each interval. Vertical bars represent 95% CI (From Guilbert TW, et al. N Engl J Med 2006;354:1985-1997, according to the Creative Commons License) [12].
- TOOLS
-
- Share :
-





-
METRICS

-
- 0 Crossref
- Scopus
- 1,322 View
- 6 Download
-

-
Related articles in
J Korean Med Assoc
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
