



 |
 |
| J Korean Med Assoc > Volume 55(5); 2012 > Article |
Abstract
Proton beam therapy (PBT) was initiated in the particle accelerator located in the physics laboratory. As this modality moves from the research laboratory to hospital-based facilities, there has been a rapid growth in the number of proton medical facilities worldwide. The clinical advantage of proton radiotherapy over photon radiotherapy is the marked reduction in the radiation dose to the normal tissues due to the absence of an exit dose with a proton Bragg peak. Pediatric patients are considered to have the maximum clinical gain with the use of protons because their normal tissues will keep developing and growing with an anticipated long remaining life. In pediatric brain tumors, PBT is used aiming to preserve neurocognitive function as much as possible. In this article, the basic principles and benefits of PBT are introduced with the latest available clinical data on PBT for pediatric brain tumors.
Acknowledgement
This study was supported by a grant from the National R&D Program for Cancer Control, Ministry of Health and Welfare, Republic of Korea (no. 0520300), and also by National Cancer Center Korea Grant 1010480.
References
1. Halperin EC, Constine LS, Tarbell NJ, Kun LE. Pediatric radiation oncology 2011;5th ed. Philadelphia: Lippincott Williams & Wilkins.
2. Miralbell R, Lomax A, Cella L, Schneider U. Potential reduction of the incidence of radiation-induced second cancers by using proton beams in the treatment of pediatric tumors. Int J Radiat Oncol Biol Phys 2002;54:824-829.
3. Yoon M, Shin DH, Kim J, Kim JW, Kim DW, Park SY, Lee SB, Kim JY, Park HJ, Park BK, Shin SH. Craniospinal irradiation techniques: a dosimetric comparison of proton beams with standard and advanced photon radiotherapy. Int J Radiat Oncol Biol Phys 2011;81:637-646.
4. Chung CS, Keating N, Yock T, Tarbell N. Comparative analysis of second malignancy risk in patients treated with proton therapy versus conventional photon therapy. Int J Radiat Oncol Biol Phys 2008;71:1 Suppl. S8.
5. De Ruysscher D, Mark Lodge M, Jones B, Brada M, Munro A, Jefferson T, Pijls-Johannesma M. Charged particles in radiotherapy: a 5-year update of a systematic review. Radiother Oncol 2012;02. 10. [Epub].
6. Fitzek MM, Linggood RM, Adams J, Munzenrider JE. Combined proton and photon irradiation for craniopharyngioma: long-term results of the early cohort of patients treated at Harvard Cyclotron Laboratory and Massachusetts General Hospital. Int J Radiat Oncol Biol Phys 2006;64:1348-1354.
7. Luu QT, Loredo LN, Archambeau JO, Yonemoto LT, Slater JM, Slater JD. Fractionated proton radiation treatment for pediatric craniopharyngioma: preliminary report. Cancer J 2006;12:155-159.
8. Merchant TE, Hua CH, Shukla H, Ying X, Nill S, Oelfke U. Proton versus photon radiotherapy for common pediatric brain tumors: comparison of models of dose characteristics and their relationship to cognitive function. Pediatr Blood Cancer 2008;51:110-117.
9. Merchant TE, Kiehna EN, Kun LE, Mulhern RK, Li C, Xiong X, Boop FA, Sanford RA. Phase II trial of conformal radiation therapy for pediatric patients with craniopharyngioma and correlation of surgical factors and radiation dosimetry with change in cognitive function. J Neurosurg 2006;104:2 Suppl. 94-102.
10. Merchant TE, Kiehna EN, Sanford RA, Mulhern RK, Thompson SJ, Wilson MW, Lustig RH, Kun LE. Craniopharyngioma: the St. Jude Children's Research Hospital experience 1984-2001. Int J Radiat Oncol Biol Phys 2002;53:533-542.
11. Hug EB, Muenter MW, Archambeau JO, DeVries A, Liwnicz B, Loredo LN, Grove RI, Slater JD. Conformal proton radiation therapy for pediatric low-grade astrocytomas. Strahlenther Onkol 2002;178:10-17.
12. MacDonald SM, Safai S, Trofimov A, Wolfgang J, Fullerton B, Yeap BY, Bortfeld T, Tarbell NJ, Yock T. Proton radiotherapy for childhood ependymoma: initial clinical outcomes and dose comparisons. Int J Radiat Oncol Biol Phys 2008;71:979-986.
13. Chang JW, Yu YS, Kim JY, Shin DH, Choi J, Kim JH, Kim SJ. The clinical outcomes of proton beam radiation therapy for retinoblastomas that were resistant to chemotherapy and focal treatment. Korean J Ophthalmol 2011;25:387-393.
14. Vavvas D, Kim I, Lane AM, Chaglassian A, Mukai S, Gragoudas E. Posterior uveal melanoma in young patients treated with proton beam therapy. Retina 2010;30:1267-1271.
15. Hug EB, Adams J, Fitzek M, De Vries A, Munzenrider JE. Fractionated, three-dimensional, planning-assisted protonradiation therapy for orbital rhabdomyosarcoma: a novel technique. Int J Radiat Oncol Biol Phys 2000;47:979-984.
16. Peeters A, Grutters JP, Pijls-Johannesma M, Reimoser S, De Ruysscher D, Severens JL, Joore MA, Lambin P. How costly is particle therapy? Cost analysis of external beam radiotherapy with carbon-ions, protons and photons Radiother Oncol 2010;95:45-53.
17. Lundkvist J, Ekman M, Ericsson SR, Jonsson B, Glimelius B. Cost-effectiveness of proton radiation in the treatment of childhood medulloblastoma. Cancer 2005;103:793-801.
Figure 1
Proton therapy facility in National Cancer Center, Korea. (A) As one of the proton facility's main components, the cyclotron accelerates protons to 60% of the light speed in order to enable it to reach deeply-seated tumors in the body. (B) Beam transportation line. Magnet is used to deflect the proton beam, transporting it to the treatment room. (C) Gantry treatment room. The proton beam can be delivered to a patient at any angle since the huge steel structured gantry revolves 360 degrees around the patients who lies on the couch. (Courtesy of National Cancer Center, Korea)
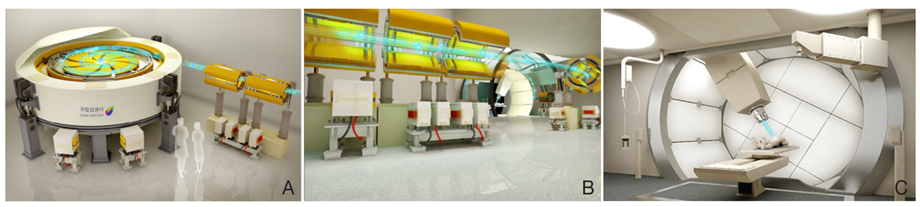
Figure 2
Depth dose distribution of proton beam in comparison with conventional proton beam. (A) As opposed to the X-ray which builds up the highest energy a few millimeters below the skin and loses its energy as it penetrates matter (blue), the proton beam releases a relatively low dose of energy before it reaches the target. After depositing the biggest energy on the target it suddenly stops its activity afterwards. The point where the highest energy is released is called "Bragg peak" (red). Since the Bragg peak of monoenergetic proton beam is too narrow to cover the extent of most target volumes, the Bragg peak can be spread out by superposition of several beams of different energies, which is called "Spread of Bragg Peak" (pink). (B) Side-by-side comparison of a photon (left) and a proton beam in the treatment on retinoblastomo (right).

Figure 3
Treatment plan for craniospinal Irradiation in the patient with medulloblastoma. Sagittal view of three-dimensional conformal radiotherapy (3D-CRT) (A,B) , tomotherapy (C,D), proton beam therapy (E,F).
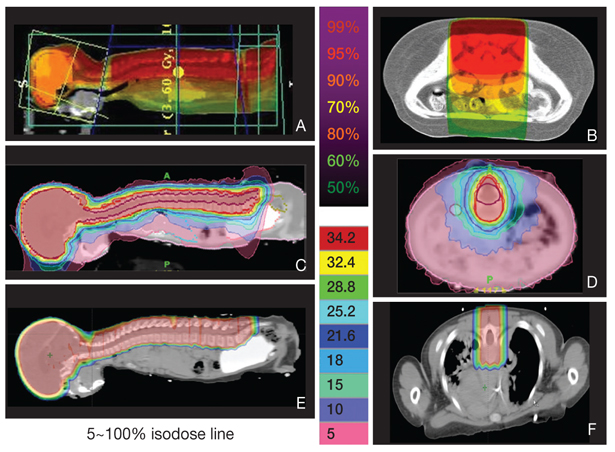
Figure 4
An example of proton beam treatment plan, irradiating only thecal sac. As most of the vertebral bones are excluded from the radiation field, bone marrow function can be preserved.
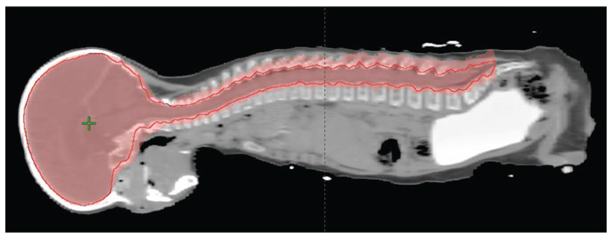
Figure 5A
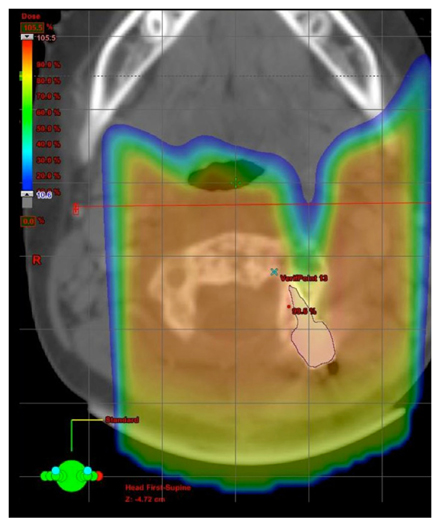
Treatment plan comparison of tumor bed boost of medulloblastoma, 3-dimensional conformal radiation therapy (left), intensity-modulated radiation therapy (middle), and proton beam therapy (right). Different colors of isodoses indicates 10% (magenda), 20% (skyblue), 40% (orange), 60% (light green), 80% (yellow), 95% (green) isodose line of the prescribed dose. Planning target volume (pink), clinical target volume (yellow), gross target volume (red) are indicated in translucent colors.
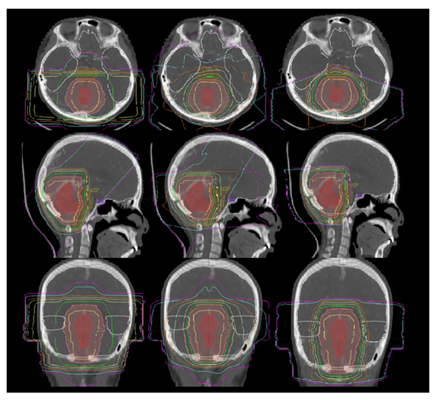
Figure 5B
Comparison of dose volume histogram obtained from intensity-modulated radiation therapy (IMRT, triangle symbol) and proton beam therapy (square symbol). The X axis of the graph indicates 0% to 100% of the prescribed dose by 10% incre-ment. Y axis of the graph indicates 0% to 100% of the volumes of each organs-at-risk (OAR). Demonstrated OAR: hypothalamus (HT, light purple), right cochlea (light green), brain stem (BS, light blue), pituitary gland (Pit, purple), temporal lobe (TL, white). Area under each curve represents the mean dose of each organs by IMRT or proton.

Figure 6
Verification if treatment side by the use of Digital Image Processing System (DIPS) at National Cancer Center, Korea. After positioning the patient on treatment coach, the patient's position is verified by digital image positioning system (DIPS), to precisely deliver the prescribed dose of proton to the tumor (A). The daily X-rays obtained by DIPS is compared to the digitally reconstructed radiographs obtained at the time of simulation with computed tomography (B).
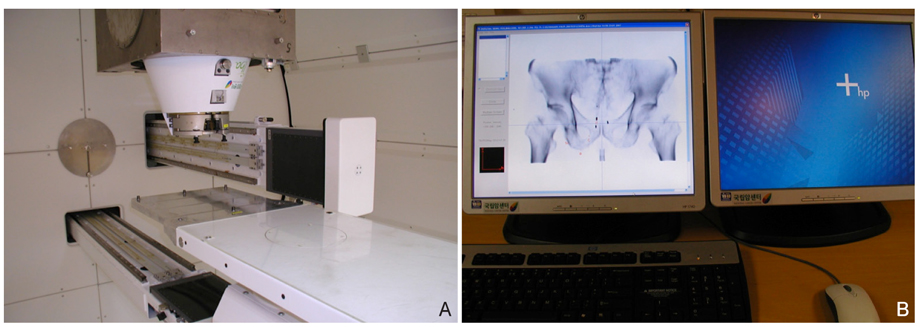
Figure 7
Preparation of pediatric anesthesia for proton beam thearpy. The children are brought to the treatment room (A) and then, anesthesiology team starts anesthesic procedure (B). The children are recovered in the recovery room before they go back to the ward (C). Informed consent was received from parents of the patient.

- TOOLS
-
- Share :
-





-
METRICS

-
Related articles in
J Korean Med Assoc -
Medical nutrition therapy for diabetes mellitus2023 July;66(7)
Reperfusion therapy in acute ischemic stroke2022 July;65(7)
Rehabilitation therapy for patients with osteoporosis2021 May;64(5)
Benign arrhythmias in pediatric patients2020 July;63(7)
Hormone Replacement Therapy and the Brain Function2000 May;43(5)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
