



 |
 |
| J Korean Med Assoc > Volume 51(11); 2008 > Article |
Abstract
Benign paroxysmal positional vertigo (BPPV) is characterized by brief recurrent episodes of vertigo triggered by head position changes. BPPV is one of the most common causes of recurrent vertigo. BPPV results from abnormal stimulation of the cupula within any of the three semicircular canals by free-floating otoliths (canalithiasis) or otoliths adhered to the cupula (cupulolithiasis). Typical symptoms and signs of BPPV are evoked when the head is positioned so that the plane of the affected semicircular canal is spatially vertical and thus aligned with gravity. Paroxysm of vertigo and nystagmus develops after a brief latency during Dix-Hallpike maneuver in posterior canal BPPV and supine roll test in horizontal canal BPPV. Usually positioning the head in the opposite direction reverses the direction of the nystagmus. The duration, frequency, and intensity of symptoms of BPPV vary depending on the involved canals and the nature of otolithic debris. Spontaneous recovery occurs frequently even with conservative treatment, however, canalith repositioning maneuvers are believed to be the best way to treat BPPV by moving the canaliths from the semicircular canal to the vestibule.
References
1. von Brevern M, Radtke A, Lezius F, Feldmann M, Ziese T, Lempert T, Neuhauser H. Epidemiology of benign paroxysmal positional vertigo: a population based study. J Neurol Neurosurg Psychiatry 2007;78:710-715.
2. Steenerson RL, Cronin GW, Marbach PM. Effectiveness of treatment techniques in 923 cases of benign paroxysmal positional vertigo. Laryngoscope 2005;115:226-231.
3. Moon SY, Kim JS, Kim BK, Kim JI, Lee H, Son SI, Kim KS, Rhee JK, Han KC, Lee WS. Clinical characteristics of benign paroxysmal positional vertigo in Korea: a multicenter study. J Korean Med Sci 2006;21:539-543.
4. Fife TD, Iverson DJ, Lempert T, Furman JM, Baloh RW, Tusa RJ, Hain TC, Herdman S, Morrow MJ, Gronseth GS. Practice Parameter: Therapies for benign paroxysmal positional vertigo (an evidence-based review): Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2008;70:2067-2074.
5. Baloh RW, Honrubia V, Jacobson K. Benign positional vertigo: clinical and oculographic features in 240 cases. Neurology 1987;37:371-378.
6. Lempert T, Leopold M, von Brevern M, Neuhauser H. Migraine and benign positional vertigo. Ann Otol Rhinol Laryngol 2000;109:1176.
7. Cohen HS, Kimball KT, Stewart MG. Benign paroxysmal positional vertigo and comorbid conditions. ORL J Otorhinolaryngol Relat Spec 2004;66:11-15.
8. Vibert D, Kompis M, Haüsler R. Benign paroxysmal positional vertigo in older women may be related to osteoporosis and osteopenia. Ann Otol Rhinol Lanyngol 2003;112:885-889.
9. Ziavra NV, Bronstein AM. Is uric acid implicated in benign paroxysmal positional vertigo? J Neurol 2004;251:115.
10. Barany R. Diagnose von Krankheitserscheinunen im berieche des oolithenapparates. Acta Otolaryngol 1921;2:434-437.
11. Dix R, Hallpike CS. The pathology, symptomatology, and diagnosis of certain common disorders of vestibular system. Proc R Soc Med 1952;54:341-354.
12. Schuknecht HF. Cupulolithiasis. Arch Otolaryngol 1969;90:765-778.
13. Hall SF, Ruby RRF, McClure JA. The mechanics of benign paroxysmal vertigo. J Otolaryngol 1979;8:151-158.
14. Parnes LS, McClure JA. Free-floating endolymph particles: a new operative finding during posterior semicircular canal occlusion. Laryngoscope 1992;102:988-992.
15. McClure JA. Horizontal canal benign positional vertigo. J Otolaryngol 1985;14:30-35.
16. Baloh RW, Yue Q, Jacobson KM, Honrubia V. Persistent direction-changing positional nystagmus: Another variant of benign positional nystagmus? Neurology 1995;45:1297-1301.
17. Bisdorff AR, Debatisse D. Localizing signs in positional vertigo due to lateral canal cupulolithiasis. Neurology 2001;57:1985-1988.
18. Han BI, Oh HJ, Kim JS. Nystagmus while recumbent in horizontal canal benign paroxysmal positional vertigo. Neurology 2006;66:706-710.
19. Koo JW, Moon IJ, Shim WS, Moon SY, Kim JS. Value of lying-down nystagmus in the lateralization of horizontal semicircular canal benign paroxysmal positional vertigo. Otol Neurotol 2006;27:367-371.
20. Lee SH, Choi KD, Jeong SH, Oh YM, Koo JW, Kim JS. Nystagmus during neck flexion in the pitch plane in benign paroxysmal positional vertigo involving the horizontal canal. J Neurol Sci 2007;256:75-80.
21. Kim JS. Positional downbeating nystagmus: Tips from the transitions. J Korean Balance Soc 2002;2:235-239.
22. Imai T, Ito M, Takeda N, Uno A, Matsunaga T, Sekine K, Kubo T. Natural course of the remission of vertigo in patients with benign paroxysmal positional vertigo. Neurology 2005;64:920-921.
23. Brandt T, Daroff RB. Physical therapy for benign paroxysmal positional vertigo. Arch Otolaryngol 1980;106:484-485.
24. Semont A, Freyss G, Vitte E. Curing the BPPV with a liberatory maneuver. Adv Otorhinolaryngol 1988;42:290-293.
25. Epley JM. The canalith repositioning procedure: for treatment of benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg 1992;107:399-404.
26. Macias JD, Ellensohn A, Massingale S, Gerkin R. Vibration with the canalith repositioning maneuver: A prospective randomized study to determine efficacy. Laryngoscope 2004;114:1011-1014.
27. Gordon CG, Gadoth N. Repeated versus single physical maneuver in benign paroxysmal positional vertigo. Acta Neurol Scand 2004;110:166-169.
28. Hilton M, Pinder D. The Epley (canalith repositioning) manoeuvre for benign paroxysmal positional vertigo. Cochrane Database Syst Rev 2004;2:CD003162.
29. Lempert J. Horizontal benign positional vertigo. Neurology 1994;44:2213-2214.
30. Vannucchi P, Giannoni B, Pagnini P. Treatment of horizontal semicircular canal benign paroxysmal positional vertigo. J Vestib Res 1997;7:1-6.
31. Appiani GC, Catania G, Gagliardi M, Cuiuli G. Repositoning maneuver for the treantment of the apogeotropic variant of horizontal canal benign paroxysmal positional vertigo. Otol Neurotol 2005;26:257-260.
32. Gufoni M, Mastrosimone L, Di Nasso F. Repositioning maneuver in benign paroxysmal vertigo of horizontal semicircular canal. Acta Otorhinolaryngol Ital 1998;18:363-367.
33. Honrubia V, Baloh RW, Harris MR, Jacobson KM. Paroxysmal positional vertigo syndrome. Am J Otol 1999;20:465-470.
34. Leveque M, Labrousse M, Seidermann L, Chays A. Surgical therapy in intractable benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg 2007;136:693-698.
Figure 1
Dix-Hallpike maneuver for diagnosis of benign paroxysmal positional vertigo (BPPV) involving the left posterior canal (PC-BPPV).
(A) With the patient sitting on the examination table, facing forward, eyes open (A-1), the physician turns the patient's head 45 degrees to the left (A-2). The physician supports the patient's head as the patient lies back quickly from a sitting to supine position, ending with the head hanging 20 degrees off the end of the examination table (A-3).
(B) These diagrams show the semicircular canals and translocation of the canalithiasis during each stage of Dix-Hallpike maneuver.
(C) If PC-BPPV is present, upbeat and counterclockwise (from the patient's perspective) torsional nystagmus ensues usually within seconds.
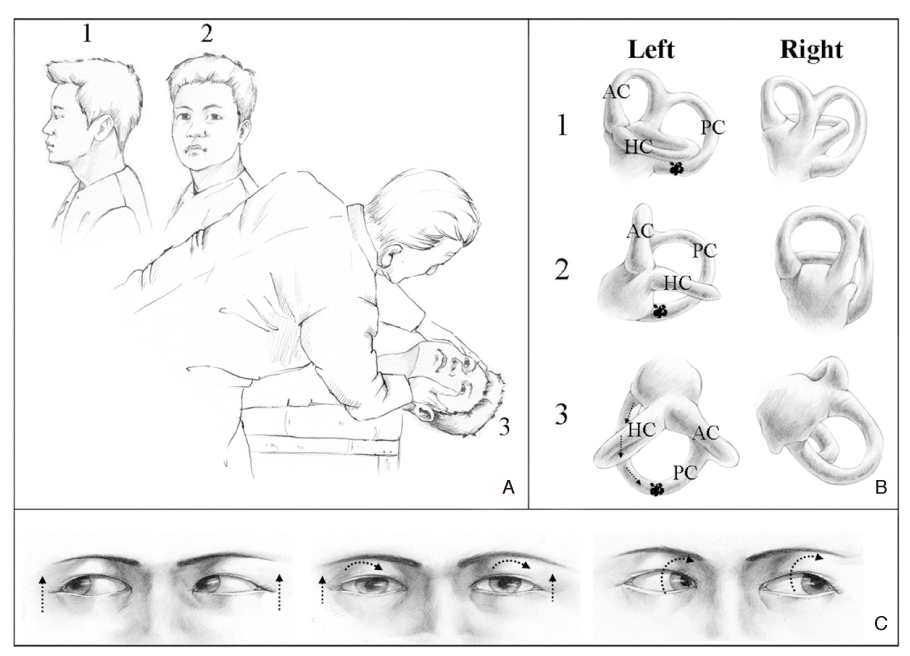
Figure 2
Two types of positional nystagmus are induced by head turning while lying down in horizontal canal type of benign paroxysmal positional vertigo. (A) In geotropic type, the nystagmus beats to the ground. (B) In apogeotropic type, the nystagmus beats toward the ceiling.
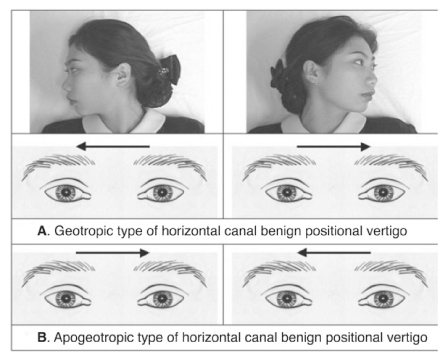
Figure 3
Canalith repositioning maneuver (modified Epley maneuver) for left posterior canal benign paroxysmal positional vertigo. (A~C) Initial three steps are same as the Dix-Hallpike maneuver in figure 1. (C) The head hanging 20~30 degrees off the end of the table should be sustained for more than 30 seconds. (D) The physician turns the patient's head 90 degrees to the right side. The patient also should be remained in this position for more than 30 seconds. (E) The physician turns the patient's head an additional 90 degrees to the right while the patient rotates his or her body 90 degrees in the same direction. The patient remains in this position for more than 30 seconds. (F) The patient sits up on the right side of the examination table. (G) Finally, the physician turns the patient's head to the neural position.

- TOOLS
-
- Share :
-





-
METRICS

-
Related articles in
J Korean Med Assoc
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
