서론
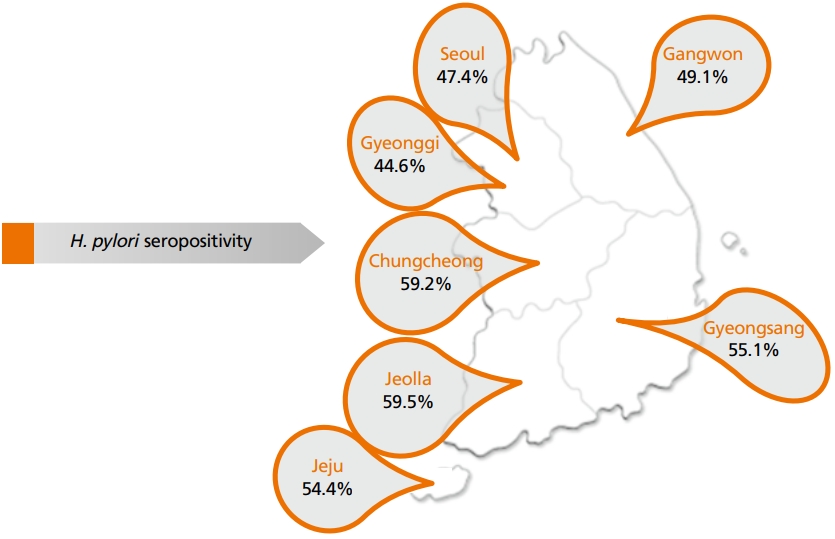
헬리코박터 파일로리(Helicobacter pylori)는 나선 모양의 그람 음성 박테리아이며, 인간에서 가장 흔한 만성 박테리아 감염을 유발한다. 이 박테리아는 지역, 연령, 인종/민족, 사회경제적 지위에 따라 상당한 차이가 있지만, 세계 인구의 약 절반에 존재하는 것으로 보고되고 있다[1,2]. 위암 발생에서 H. pylori의 역할을 입증하는 다양한 증거가 보고됨에 따라 1994년 세계보건기구와 국제암연구소(International Agency for Research on Cancer)에서 group I carcinogen로 지정하고 있다[3]. H. pylori와 비분문부 위암의 발병 사이의 연관성은 잘 확립되어 있으며 H. pylori에 감염된 대부분의 사람들은 무증상으로 남아있지만, 1-3%에서 위선 암이 발생하고 전체 위암의 약 90%가 H. pylori에 기인한다고 알려져 있다[1]. 위암의 발병률은 H. pylori 감염이 높은 동아시아, 특히 한국, 일본 및 중국 등에서 높은 것으로 잘 알려져 있다. 최근 국내의 H. pylori 감염 보고에 따르면 각 지역별로 차이는 있지만 전체적으로 51%로 높은 유병률을 보이고 있다(Figure 1) [4]. 위 종양의 약 90%는 선암으로 2가지 주요 조직학적 유형인 장형 또는 미만형으로 분류되며, H. pylori는 위암의 두 하위 유형과 모두 관련이 있지만, 특히 장형 선암의 발생과 더 밀접하게 관련되어 있는 것으로 보고되고 있다[5,6]. 장형 위암의 발생은 위 위축과 장상피화생(intestinal metaplasia)을 동반한 체부에 주된 위염(corpus-dominant gastritis)을 특징으로 하는 반면, 미만형은 위축 없이 위 전체의 위염을 특징으로 한다[7]. 이에 이 논문에는 위암 발생의 위험인자로의 헬리코박터 위염에 대하여 기술하고자 한다.
H. pylori가 위암을 일으키는 기전
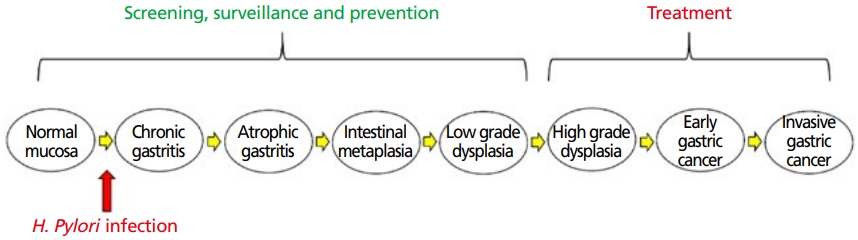
Correa cascade 가설은 장형 선암의 단계적 발달은 잘 설명하고 있다(Figure 2) [8,9]. H. pylori의 감염은 오랜 기간 동안 정상 점막에서 만성 위염으로의 변화를 일으키고, 이는 더 나아가 위축성 위염, 장상피화생, 이형성, 그리고 마지막으로 선암으로 진행됨을 설명하고 있다 H. pylori 감염은 이 경로에서 만성 활동성 위염을 유발하는 가장 잘 알려진 유발요인이다. H. pylori 감염에 의한 만성적인 위 염증은 nuclear factor kappa B 발현을 증가시켜 활성화 유도 사이티딘디아미나제(activation-induced cytidine deaminase)의 발현을 유도하게 된다, 이 활성화 유도 사이티딘디아미나제가 TP53, CDKN2BCDKN2A 등 여러 암 억제유전자의 돌연변이를 유발시키는 것이 위암을 일으키는 중요한 기전 중에 하나라고 알려져 있다[10]. 동시에 interleukin-1, tumor necrosis factor-α 등 염증성 사이토카인의 발현을 증가시키고 산화스트레스를 조장하여, DNA 메틸화 이상 및 microRNA 발현 변화를 초래함으로써 위암 발생에 기여한다고 알려져 있다. H. pylori에 의한 만성 염증은 위의 전정부에서 시작하여 체부 소만을 거쳐 체부 대만측으로 범위가 확장되며, 위의 벽세포(parietal cell)와 으뜸세포(chief cells)를 파괴하여 무산증과 위축성 위염을 유발한다. 위 전구 세포의 성장 및 분화를 조절하는 신호를 정상적으로 분비하는 벽세포와 으뜸세포의 손실은 미분화 위 전구 세포의 증식, 축적 및 장상피화생을 초래하며, 장상피화생은 이형성증과 암종을 유발할 수 있는 미분화 전구 세포가 있는 전암성 병변으로 인식되고 있다[11-13].
H. pylori의 특성
H. pylori가 위암을 유발하는 분자 메커니즘은 완전히 이해되지 않았지만, 독성인자, 숙주의 유전적 소인 및 환경인자의 조합으로 알려져 있다. H. pylori는 위의 가혹하고 산성인 환경에서 생존하도록 적응한 독특한 박테리아로 위에서 생존할 수 있는 여러 특성을 가지고 있다[14]. 나선형 모양과 편모는 운동성을 최적화하여 점막을 통해 위 상피에 도달할 수 있으며, 세균 표면 부착소는 위 상피세포의 숙주 수용체를 인식하고 결합한다. H. pylori는 위 요소를 가수분해하여 암모니아를 형성하는 요소분해효소(urease)를 생성하고 생성된 암모니아는 위산을 중화시켜 세균이 위점막으로 침투하도록 하여 상피세포를 손상시킨다. 요소분해효소는 또한 염증 세포를 자극하여 추가 세포 손상을 유발한다[15,16]. H. pylori는 두 가지 독성인자인 cytotoxinassociated antigen A (CagA) 및 vacuolating cytotoxin (VacA)이 가장 잘 알려져 있으며, 위암 발생과 밀접한 관련이 있는 것으로 알려져 있다[17,18]. CagA는 세포 증식 증가, 세포 사멸 감소 및 세포 극성 변경을 포함하여 위 상피세포에 다양한 영향을 미치며, 이는 모두 종양 발달을 촉진하는 것으로 알려져 있으며, 비분무부 위암 발생 위험에 있어서 CagA 음성 균주에 비해 CagA 양성 균주를 가진 개인에서 더 빈번한 것으로 알려져 있다[19]. 16건의 연구에 대한 한 메타분석 연구[20]에서는 CagA 양성군에서 위암의 발생이 2배 이상 높은 것으로 보고하였다(교차비, 2.01; 95% 신뢰구간, 1.21-3.32). VacA는 위 상피세포의 세포질에서 산성의 액포(vacuole) 형성을 촉진하는 또 다른 중요한 독성인자로, VacA는 요소에 대한 위 상피의 투과성을 증가시켜 요소분해효소 활성을 최적화할 수 있는 요소 수송체 역할을 한다. VacA는 또한 세포 사멸을 유도하고 상피세포 폐쇄막(tight junction)을 파괴하여 세포 붕괴를 유발하며, T-세포 증식을 억제하고 숙주 면역 반응을 변화시켜 H. pylori의 지속적인 군집화를 가능하게 하는 면역억제제 역할을 하는 것으로 알려져 있다.
헬리코박터 위염의 내시경 소견
최근 내시경 기기의 발전으로 위점막의 해상도가 좋아지면서 이전에는 조직검사로만 진단할 수 있었던 병변들을 내시경 소견만으로도 예측할 수 있게 되었고, 특히 H. pylori 감염에 의해 발생하는 다양한 염증 소견을 바탕으로 H. pylori 감염 여부를 확인 및 위암 발생과의 연관성을 예측하고자 하는 노력이 있었고, 최근에는 위점막의 내시경 소견으로 H. pylori 감염 상태와 위암에 대한 위험성을 예측할 수 있는 Kyoto 분류가 소개되었다[21]. Kyoto 분류의 주요 내용은 국소 병변이 아닌 배경 위점막의 내시경 소견으로 H. pylori 감염 상태를 판단하여, H. pylori의 현재 감염, 과거 감염(제균 후), 미감염을 위내시경 소견으로 감별하고 위암에 대한 위험성을 0-8점 사이로 점수화하여 예측하는 데 있다(Table 1) [21]. 또한 최근에는 영상강화내시경(image-enhanced endoscopy)과 확대 내시경 및 세포내시경(endocytoscopy)을 이용한 H. pylori 위염의 진단의 유용성에 대해서도 보고되고 있다[22,23]. 하지만 모든 소견과 감염 상태가 전부 일치하는 것은 아니고, 내시경 의사마다 주관적인 소견이 다양하기에 이러한 소견들은 현재도 관련성 및 객관화에 대한 연구들이 다양하게 진행 중에 있다.
1. H. pylori 미감염 관련 내시경 소견
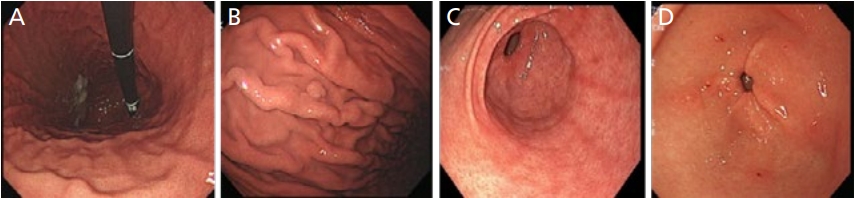
내시경검사에서 위각이나 체부의 소만측에서 보이는 균일한 집합 소정맥이 규칙적으로 배열하고 있는 영상을 확인할 수 있는데, 이를 세정맥 집합(regular arrangement of collecting venules, RAC)이라 규정하고 있으며, 이러한 RAC는 먼 거리에서는 붉은 점 형태로 보이나, 근접 관찰에서는 불가사리 내지는 새의 발자국 모양으로 위각부와 위체부의 소만에서 주로 관찰되며, 이는 손상되지 않는 위점막을 의미한다고 알려져 있다[24]. RAC 소실은 H. pylori 감염 이외에 다른 원인에 의해서도 발생할 수 있으나 상대적으로 드물기 때문에 RAC는 H. pylori 감염이 없었던 위점막임을 시사하는 대표적 소견으로 알려져 있고, 민감도와 특이도가 매우 높은 것으로 알려져 있다[25,26]. 이외에도 H. pylori 미감염을 시사하는 소견으로서 5 mm 미만의 다발성 위저선용종(fundic gland polyp)이 있으며, 그 밖에 전정부의 대만측이나 체부 소만측의 규칙적인 붉은 선상 발적(red streaks), 전정부의 융기성 미란(raised erosions), 헤마틴(hematin)의 관찰 등도 H. pylori 미감염 소견으로 흔히 나타날 수 있는 소견이다(Figure 3) [27].
2. H. pylori 현재 감염 상태에 따른 위내시경 소견
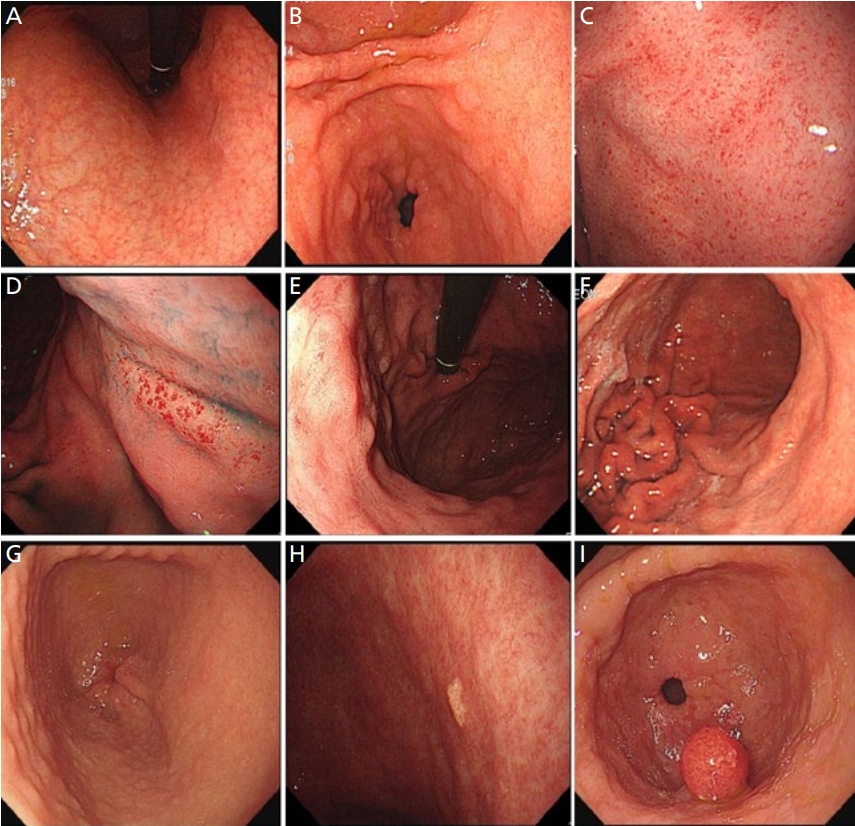
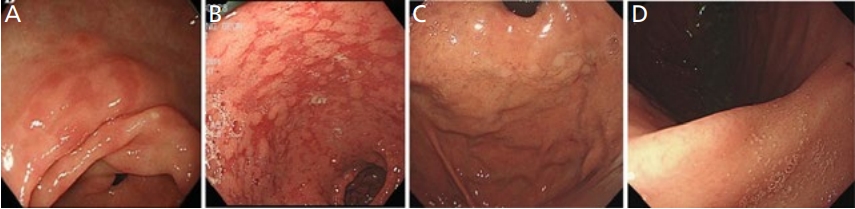
현재까지 H. pylori 감염과 연관되어 제안되고 있는 내시경 소견들로는 위선의 위축과 장상피화생, 결정상(nodularity), 주름의 비후(rugal hypertrophy), 미만성의 발적(diffuse redness), 점상 홍반(spotty redness), 점막 부종(mucosal swelling)과 끈적한 점액(sticky mucus) 소견과 과형성용종(hyperplastic polyp)의 존재나 황색종, 그리고 전정부의 함몰성 점막(depressed erosion) 병변 등이 있다[27-29]. H. pylori 감염이 장기간 지속되면 고유 위선의 감소로 인한 위축성 변화가 발생하며, 위축은 점막이 얇아져서 점막하층이 희끗 희끗한 모양으로 투영되거나, 점막하층의 혈관상이 보라색의 긴 나뭇가지 형태로 관찰되면 진단할 수 있다. 정상 점막과 위축성 변화가 동반된 경계 부위를 위축 경계선(atrophic border)으로 정의하며, 전정부에 국한된 위축성 위염은 H. pylori 감염이 없는 고령에서 흔히 관찰되며, 위암 발생의 위험은 낮은 것으로 알려져 있다[26]. H. pylori 감염이 장기간 지속되는 경우, 위축 경계선이 체부로 상승하면서 위 주름의 소실이 동반된다. 위축성 변화는 전정부에서 시작하여 위각을 지나 체부 소만측으로 진행하며 대만과 기저부는 가장 늦게 침범하며 위축의 정도와 범위는 Kimura-Takemoto 분류를 주로 사용하여 기술한다. 위축성 위염은 C1, C2, C3, O1, O2 및 O3로 등급으로 매겨지며, 위축 정도에 따라. C1, C2, C3는 폐쇄형, O1, O2, O3는 개방형으로 분류하고 있다[30]. 장상피화생의 경우는 백색광 내시경에서 불규칙하고 울퉁불퉁한 회백색 융기 병변, 얼룩성 발적(patchy redness), 융모상 변화(villous change) 및 지도상 발적(map-like redness) 등으로 관찰될 수 있으며, 지도상 발적은 과거 H. pylori 감염인 경우에 흔하고 그 외 소견은 H. pylori 만성 감염자에서 주로 관찰된다[31]. 더불어 영상강화내시경 검사에서는 light blue crest, bluish-whitish area 및 white opaque substance lavender color 등의 소견으로 보이며, 이는 장상피화생 부위의 브러시 테두리의 빛 반사율의 차이에 기인하는 것으로 알려져 있다[32-35]. 심한 위축성 변화와 장상피화생은 장형 위암의 발생 위험성을 증가시킨다[36]. 광범위한 발적의 경우 염증을 가진 위점막에서 점막 표증에 분포하는 모세혈관의 울혈과 확장에 의해서 나타나고, 점상 출혈, 융합된 발적, 혈관상의 투영 등이 기저부와 체부 대만 등에서 더 뚜렷하게 관찰된다[37]. 형태는 1 mm 미만의 다발성 출혈성 반점에서부터 광범위한 발적까지 다양하게 관찰될 수 있다. 또한 결정상은 마치 위점막이 닭살 모양으로 관찰되며, H. pylori에 의해 형성된 림프 여포(lymphoid follicle)와 림프 혈장계 세포의 응집(lymphoplasma cell aggregate)으로 이루어져 있다. 주로 전정부에서 이를 확인하면 현감염과의 연관성이 높다고 알려져 있으며, 젊은 여성에서 흔하고, 미만형 위암의 위험인자로 알려져 있다[38]. 주름의 비후는 위 주름이 5 mm 이상으로 두꺼워져 있는 경우를 지칭하며 이와 함께 체부 대만을 포함한 위점막에 끈적한 점액이 관찰되면 H. pylori 감염 여부을 시사한다고 할 수 있다[39,40]. 앞서 언급한 비후성 변화와 광범위한 발적 및 일부 결절성 위염의 경우는 급성 활동성 H. pylori 감염에 의한 것으로 알려져 있고, 미만형 위암의 발생과 연관이 있는 것으로 알려져 있다[40]. 과형성용종은 다른 원인으로 유발되기도 하지만, 대부분 H. pylori 감염으로 인해 발생하는 것으로 보고되고 있다. 선종(adenoma)과는 달리 붉은색으로 튀어나온 형태를 띠는 것으로 감별이 가능하다. 황색종은 비가역적인 병변으로 H. pylori 감염이 장기간 지속되어 응집된 조직구가 노란색 반점으로 관찰되는 병변으로, 과거 H. pylori 감염자에서 흔한 것으로 알려져 있다(Figure 4).
3. H. pylori 제균 이후의 내시경 소견
H. pylori 감염 후 급 만성 염증에 의하여 다핵구 세포(polymorphonuclear cell)의 침윤이 만성 염증 단계에서는 단핵구 세포의 침윤이 특징적이며, H. pylori의 제균 후에는 위점막의 만성적인 염증이 개선되면서 조직학적으로는 다핵구 침윤은 저명하게 개선되어 거의 사라지며, 단핵구 침윤도 제균 직후 크게 감소하고, 남아있는 단핵구 침윤은 제균 후 4-5년에 걸쳐 점진적으로 개선된다[24,41]. 따라서 제균 후의 관찰시기에 따라서 제균 후 소견은 제균 전 H. pylori 감염 소견 시의 점막 소견 및 미감염 소견이 혼재되어 관찰될 수 있다. 제균 후 단기간 내에 점상 발적, 미만성 발적, 점막 종창, 위 주름의 종대와 사행, 끈적한 점액은 개선되는 경우가 많으며, 점상 출혈의 개선이 가장 빈번한 것으로 보고되고 있다. 성공적인 제균 치료 후에 위산 분비능의 회복으로 편평 미란이 전정부에서 관찰되기도 한다[42,43]. 그 외에도 선상 발적이나 지도 모양의 발적 등이 관찰되기도 한다. 특히 지도 모양의 발적은 제균 후 위축 영역의 장상피화생을 가진 점막은 발적으로, 반대로 위축이 없는 영역의 위저선 점막은 미만성 발적이 소실하기 때문에 백색조로 관찰되는 것으로 알려져 있다(Figure 5).
결론
여러 연구에서 H. pylori 제균은 이시성뿐만 아니라 원발성 위암도 감소시킨다고 보고하고 있다[44-46]. 이러한 결과를 바탕으로 위암 예방의 치료 전략으로 H. pylori 조기 발견이 중요하다고 할 수 있다[47]. 헬리코박터균 감염을 진단하기 위해 신속요소효소검사, 조직학적 검사, 배양 등의 내시경 생검 기반 검사가 널리 이용되고 있다. 최근에 많은 연구자들이 H. pylori에 감염된 위의 특징적인 내시경 소견을 분류하려고 시도하고 있으며, 내시경 관찰로 H. pylori 여부를 추정하고 이와 관련된 위험성을 예측하고자 하는 Kyoto 분류도 소개가 되고 있다. 내시경을 통한 H. pylori 감염 여부에 대하서는 내시경 개별 단독적인 소견보다는 여러 내시경 소견들을 종합하여 검사 시에 H. pylori 감염 상태를 미리 예측하는 것을 가능하게 하며 추가적인 침습적 진단법 선택을 함에 있어 큰 의미가 있다고 할 수 있다. 또한 H. pylori 높은 유병률을 보이고 건강검진 위내시경이 보편화된 국내 상황에 적절할 수 있다고 생각된다. 내시경검사를 통한 헬리코박터 위염을 진단하기 위해서는 많은 경험과 이해가 필요하다. 따라서 이를 위한 체계적인 연구와 노력이 필요하겠다.