




 |
 |
| J Korean Med Assoc > Volume 53(10); 2010 > Article |
Sang-Hyup Yoon, MD, Shin-Yoon Kim, MD
Abstract
A large number of patients who are diagnosed with rheumatoid arthritis undergo a chronic and progressive course. Surgical treatment is often needed for these patients, who have not responded to medical treatment. The aim of surgical intervention in rheumatoid arthritis is to restore function and quality of life by preventing joint destruction, correcting deformity, relieving pain, and making cosmetic improvements. There are many surgical options, including synovectomy, osteotomy, arthrodesis, resection arthroplasty, joint replacement, surgeries for the treatment of the tendon involved (repair, transfer, graft), and cervical spine surgery (fusion or decompression). The selection of the optimal surgical option requires consideration of not only the articular status and the degree of regional deformity involved, but also the physical status and age of the patient. In addition, timely surgical intervention is important because a delay of surgery often results in poorer functional outcomes and an increase in postoperative complications. Early referral to orthopedic treatment can provide better functional outcomes for patients with rheumatoid arthritis. Precise prediction of the disease progress and selection of the optimal treatment option are needed for excellent results to be expected. Therefore, a cooperative and multidisciplinary treatment strategy should be made among the relevant teams, such as physical medicine, rheumatology, orthopedics, physical therapy, occupational therapy, social work, and psychology.
References
1. Breedveld FC. Current and future management approaches for rheumatoid arthritis. Arthritis Res 2002;4:S16-S21.
2. Verstappen SM, Hoes JN, Ter Borg EJ, Bijlsma JW, Blaauw AA, van Albada-Kuipers GA, van Booma-Frankfort C, Jacobs JW. Joint surgery in the Utrecht Rheumatoid Arthritis Cohort: the effect of treatment strategy. Ann Rheum Dis 2006;65:1506-1511.
3. van Lankveld WG, van't Pad Bosch P, van de Putte L. Predictors of changes in observed dexterity during one year in patients with rheumatoid arthritis. Br J Rheumatol 1998;37:733-739.
4. Bogoch ER, Judd MG. The hand: a second face? J Rheumatol 2002;29:2477-2483.
5. Rheumatic diseases-surgical treatment. A systematic literature review by SBU-the Swedish Council on Technology Assessment in Health Care. Acta Orthop Scand Suppl 2000;294:1-88.
6. Gariepy R, Demers R, Laurin CA. The prophylactic effect of synovectomy of the knee in rheumatoid arthritis. Can Med Assoc J 1966;94:1349-1352.
7. Kerschbaumer F, Kandziora F, Herresthal J, Hertel A, Hor G. [Combined arthroscopic and radiation synovectomy in rheumatoid arthritis]. Orthopade 1998;27:188-196.
8. Kvien TK, Pahle JA, Hoyeraal HM, Sandstad B. Comparison of synovectomy and no synovectomy in patients with juvenile rheumatoid arthritis. A 24-month controlled study. Scand J Rheumatol 1987;16:81-91.
9. Nakamura H, Nagashima M, Ishigami S, Wauke K, Yoshino S. The anti-rheumatic effect of multiple synovectomy in patients with refractory rheumatoid arthritis. Int Orthop 2000;24:242-245.
10. Herold N, Schroder HA. Synovectomy and radial head excision in rheumatoid arthritis. 11 patients followed for 14 years. Acta Orthop Scand 1995;66:252-254.
11. Vahvanen V, Eskola A, Peltonen J. Results of elbow synovectomy in rheumatoid arthritis. Arch Orthop Trauma Surg 1991;110:151-154.
12. Ertel AN. Flexor tendon ruptures in rheumatoid arthritis. Hand Clin 1989;5:177-190.
13. Trieb K. Management of the foot in rheumatoid arthritis. J Bone Joint Surg Br 2005;87:1171-1177.
14. Caron M, Kron E, Saltrick KR. Tibiotalar joint arthrodesis for the treatment of severe ankle joint degeneration secondary to rheumatoid arthritis. Clin Podiatr Med Surg 1999;16:337-361.
15. Connor J, Nalebuff EA. Current recommendations for surgery of the rheumatoid hand and wrist. Curr Opin Rheumatol 1995;7:120-124.
16. Herren DB, Ishikawa H. Partial arthrodesis for the rheumatoid wrist. Hand Clin 2005;21:545-552.
17. Jaakkola JI, Mann RA. A review of rheumatoid arthritis affecting the foot and ankle. Foot Ankle Int 2004;25:866-874.
18. O'Brien ET. Surgical principles and planning for the rheumatoid hand and wrist. Clin Plast Surg 1996;23:407-420.
19. Trieb K. Treatment of the wrist in rheumatoid arthritis. J Hand Surg Am 2008;33:113-123.
20. Kobus RJ, Turner RH. Wrist arthrodesis for treatment of rheumatoid arthritis. J Hand Surg Am 1990;15:541-546.
21. Della Santa D, Chamay A. Radiological evolution of the rheumatoid wrist after radio-lunate arthrodesis. J Hand Surg Br 1995;20:146-154.
22. Gallo RA, Payatakes A, Sotereanos DG. Surgical options for the arthritic elbow. J Hand Surg Am 2008;33:746-759.
23. Chiari C, Trieb K. Metacarpophalangeal joint arthroplasty in rheumatoid arthritis. J Bone Joint Surg Am 2004;86-A:1832-1833.
24. Nelissen RG. The impact of total joint replacement in rheumatoid arthritis. Best Pract Res Clin Rheumatol 2003;17:831-846.
25. Gough AK, Lilley J, Eyre S, Holder RL, Emery P. Generalised bone loss in patients with early rheumatoid arthritis. Lancet 1994;344:23-27.
26. Kumar MN, Swann M. Uncemented total hip arthroplasty in young patients with juvenile chronic arthritis. Ann R Coll Surg Engl 1998;80:203-209.
27. Chmell MJ, Scott RD. Total knee arthroplasty in patients with rheumatoid arthritis. An overview. Clin Orthop Relat Res 1999;366:54-60.
28. van de Sande MA, Brand R, Rozing PM. Indications, complications, and results of shoulder arthroplasty. Scand J Rheumatol 2006;35:426-434.
29. Goldfarb CA, Dovan TT. Rheumatoid arthritis: silicone metacarpophalangeal joint arthroplasty indications, technique, and outcomes. Hand Clin 2006;22:177-182.
30. Chung KC, Kowalski CP, Myra Kim H, Kazmers IS. Patient outcomes following Swanson silastic metacarpophalangeal joint arthroplasty in the rheumatoid hand: a systematic overview. J Rheumatol 2000;27:1395-1402.
31. Boden SD, Dodge LD, Bohlman HH, Rechtine GR. Rheumatoid arthritis of the cervical spine. A long-term analysis with predictors of paralysis and recovery. J Bone Joint Surg Am 1993;75:1282-1297.
32. Levy O, Funk L, Sforza G, Copeland SA. Copeland surface replacement arthroplasty of the shoulder in rheumatoid arthritis. J Bone Joint Surg Am 2004;86-A:512-518.
33. Bishop JY, Flatow EL. Humeral head replacement versus total shoulder arthroplasty: clinical outcomes-a review. J Shoulder Elbow Surg 2005;14:141S-146S.
Figure 1
(A) and (B) show radiographs of an elbow with rheumatoid arthritis. There is diffuse joint space narrowing and subchondral osteopenia; (C), (D) and (E) Arthroscopic synovectomy and debridement was perfomed. Arthroscopic findings show synovial hyperplasi and erosive change of cartilage. RH, radial head
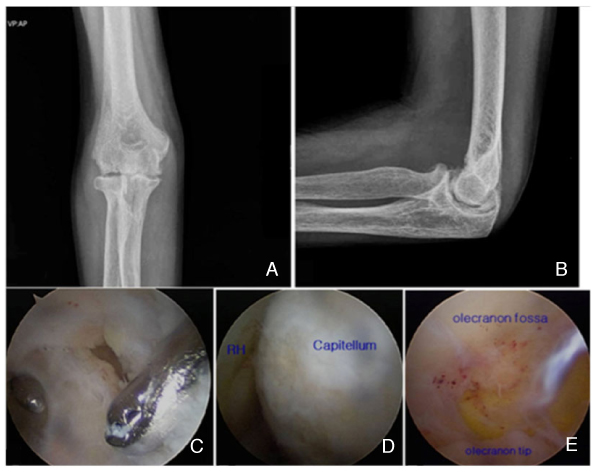
Figure 2
(A), (B) Wrist radiograph of a 56-year-old woman showing a destructive change in the wrist joint. (C) She complained of limitation of the third, fourth, and fifth fingers without trauma history. (D) Intraoperative finding showed rupture of EDC to the third, fourth, and fifth fingers. (E) The ulnar head was resected and EIP was transferred to the ruptured EDC. EDC, extensor digiti mini; EIP, extensor indicis proprius

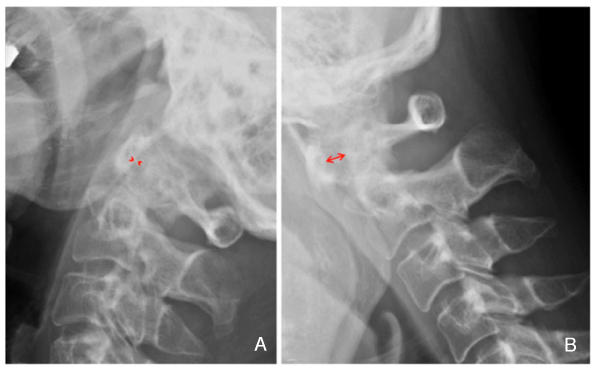
Figure 3
A 29-year-old woman with rheumatoid arthritis. (A) Anteroposterior radiograph of the right ankle shows arthritic change with a medial malleolar fracture caused by trauma. (B) The medial malleolar fracture was reduced and internally fixed with screws, and an ankle arthrodesis was performed simultaneously.

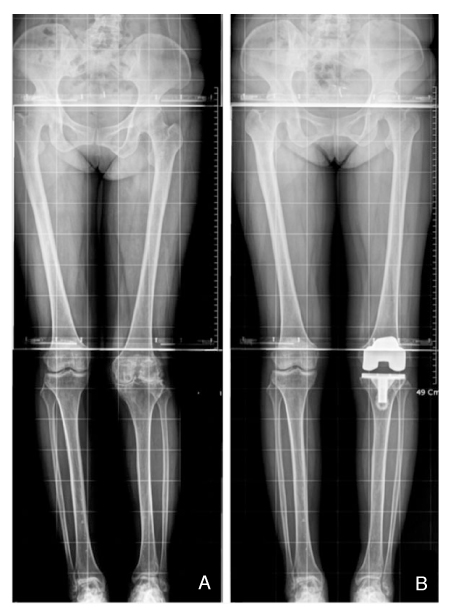
Figure 4
(A) A 39-year-old woman with rheumatoid arthritis had severe arthritic changes and valgus deformity in the left knee joint. (B) Total knee arthroplasty was done and normal alignment of the lower limb was restored.
- TOOLS
-
- Share :
-





-
METRICS

-
- 0 Crossref
- Scopus
- 1,129 View
- 9 Download
-

-
Related articles in
J Korean Med Assoc -
Surgical treatment of esophageal cancer2024 February;67(2)
Diagnosis and treatment of patellofemoral joint arthritis2023 August;66(8)
Diagnosis and treatment of trigeminal neuralgia2023 January;66(1)
Pharmacologic treatment of tinnitus2022 December;65(12)
Surgical treatment for gastroesophageal reflux disease2022 December;65(12)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
