




 |
 |
| J Korean Med Assoc > Volume 49(4); 2006 > Article |
Abstract
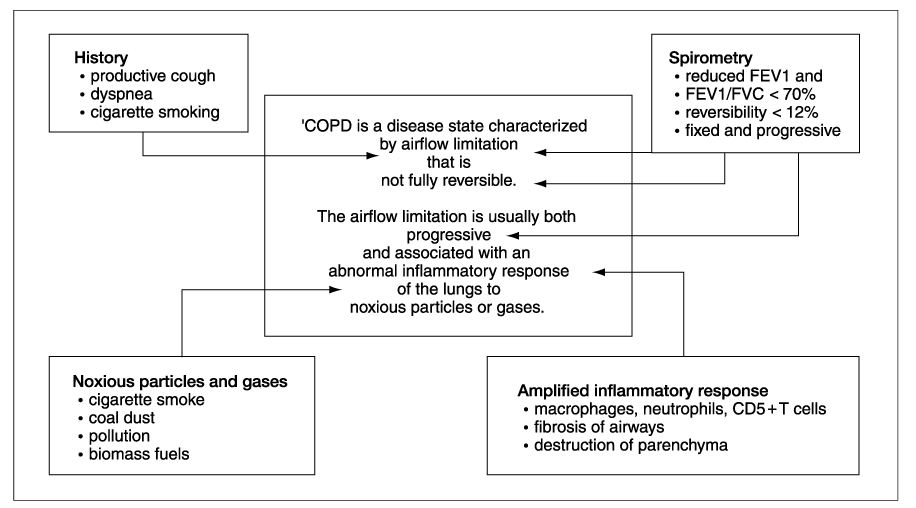
Aworking definition of chronic obstructive pulmonary disease (COPD) is given within the GOLD Global strategy as a disease state characterized by airflow limitation that is not fully reversible. The airflow limitation is usually progressive and associated with an abnormal inflammatory response of the lungs to noxious particles or gases. There is consensus that there has been a world-wide increase in COPD, reflecting increases in cigarette smoking, especially in developing countries. According to the Global Burden of Disease Study, in terms of lost disability-adjusted life years, COPD was ranked the 12th in 1990 and predicted to rise to the 5th ranking by 2020 and COPD was the sixth most common cause of death in the world in 1990 and will rise to the third most common by 2020. COPD is characterized by exaggeration of the normal inflammation response to irritant such as cigarette smoke. The mechanisms for this amplification of inflammation in COPD are not yet certain, but may be determined by genetic factors, latent viruses and impaired histone deacetylase activity. In addition to inflammation, extracellular matrix proteolysis. Cell death and ineffective repair are thought to be important in the pathogenesis of COPD.
References
1. Global Initiative for Chronic Obstructive Lung Disease (GOLD): Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease NHLBI/WHO Workshop Report. National Institutes of Health (NIH), National Heart Lung and Blood Institute (NHLBI), World Health Organiztion (WHO) 2001, 2003, 2004 and update in 2005. www.goldcopd.com/workshop/index.html
2. National Institute for Clinical Excellence (NICE). Chronic Obstructive Pulmonary Disease: national clinical guideline for management of chronic obstructive pulmonary disease in adults in primary and secondary care. Thorax 2004;59:Suppl 1. 1-232.
3. Gross NJ. Extrapulmonary effects of chronic obstructive pulmonary disease. Curr Opin Pulm Med 2001;7:84-92.
4. Hansel TT, Barnes PJ. An Atlas of Chronic Obstructive Pulmonary
Disease COPD 2004;1st ed. New York: Parthenon Publishing. 3-4.
5. Barnes PJ. Chronic obstructive pulmonary disease. N Engl J Med 2000;343:269-280.
6. Halbert RJ, Isonaka S, George D, Iqbal A. Interpreting COPD prevalence estimates: what is the true burden of disease? Chest 2003;123:1684-1692.
7. Fletcher C, Peto R. The natural history of chronic airflow obstruction. Br Med J 1977;1:1645-1648.
8. National Center for Health Statistics. Current estimates from the National Health Interview Survey, United States, 1995 Department of Health and Human Sevices, Public Health Service. Vital Health Stat 1995;96:1527.
9. Murray CJ, Lopez AD. Evidence-based health policy-lessons from the Global Burden Study. Science 1996;274:740-743.
10. Gulsvik A. Mortality in and prevalence of chronic obstructive pulmonary disease. Monaldi Arch Chest Dis 1999;54:160-162.
11. Regional COPD Working Group. COPD prevalence in 12 Asia-Pacific countries and regions: projections based on the COPD prevalence estimation model. Respirology 2003;8:192-198.
12. de Marco R, Accordini S, Cerveri I, Corsico A, Sunyer J, Burney P, et al. An international survey of chronic obstructive pulmonary disease in young adults according to GOLD stages. Thorax 2004;59:120-125.
13. Kim DS, Kim YS, Jung K-S, Chang JH, Lim C-M, Lew WJ, et al. Prevalence of Chronic Obstructive Pulmonary Disease in Korea: A Population-based Spirometry Survey. Am J Respir Crit Care Med 2005;172:842-847.
14. Slusarcick A, McCaig L. National Hospital Ambulatory Medical Care Survey: 1988 outpatient department summary. Adv Data 2000;317:1-23.
15. Mannino DM. COPD: epidemiology, prevalence, morbidity and mortality, and disease heterogeneity. Chest 2002;121:121S-126S.
16. Popovic JR, Kozak LJ. National hospital discharge survey: annnual summary, 1998. Vital Health Stat 13 2000;148:1-194.
17. Mannino DM, Homa DM, Akinbami LJ, Ford ES, Redd SC. Chronic obstructive pulmonary disease surveillance-United States, 1971~2000. Respir Care 2002;47:1184-1199.
18. Hurd S. The Impact of COPD on Lung Health Worldwide: Epidemiology and Incidence. Chest 2000;117:1S-4S.
20. Murray CJ, Lopez AD. Mortality by cause for eight regions of the world : Global Burden of Disease Study. Lancet 1997;339:1269-1276.
21. Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990~2020: Global Burden of Disease Study. Lancet 1997;349:1498-1504.
22. Barnes PJ. Molecular genetics of chronic obstructive pulmonary disease. Thorax 1999;54:245-252.
23. Meshi B, Vitalis TZ, Ionescu D, Elliott WM, Liu C, Wang XD, et al. Emphysematous lung destruction by cigarette smoke. The effects of latent adenoviral infection on the lung inflammatory response. Am J Respir Cell Mol Biol 2002;26:52-57.
24. Ito K, Lim S, Caramori G, Chung KF, Barnes PJ, Adock IM. Cigarette smoking reduces histone deacetylase 2 expression, enhances cytokine expression and inhibits glucocorticoid actions in alveolar macrophages. FASEB J 2001;15:1110-1112.
25. Laurell CB, Eriksson S. The electrophoretic alpha-globulin pattern of serum in alpha-antitrypsin deficiency. Scand J Clin Invest 1963;15:132-140.
26. Stockley RA. The role of proteinases in the pathogenesis of chronic bronchitis. Am J Respir Crit Care Med 1994;150:S109-S113.
27. Shapiro SD. Elastolytic metalloproteinases produced by human mononuclear phagocytes. Potential roles in destructive lung disease. Am J Respir Crit Care Med 1994;150:S160-S164.
28. MacNee W, Rahman I. Is oxidative stress central to the pathogenesis of chronic obstructive pulmonary disease? Trends Mol Med 2001;7:55-62.
29. Aoshiba K, Yokohori N, Nagai A. Alveolar wall apoptosis causes lung destruction and emphysematous changes. Am J Respir Cell Mol Biol 2003;28:555-562.
30. Kasahari Y, Tuder RM, Cool CD, Lynch DA, Flores SC, Voelkel NF. Inhibition of VEGF receptors causes lung cell apoptosis and emphysema. J Clin Invest 2000;106:1311-1319.
31. Massaro GD, Massaro D. Retinoic acid treatment abrogates elastase elastase-induced pulmonary emphysema in rats. Nat Med 1997;6:675-677.
- TOOLS
-
- Share :
-





-
METRICS

-
- 1 Crossref
- Scopus
- 1,141 View
- 1 Download
-

-
Related articles in
J Korean Med Assoc -
Diagnosis and evaluation of nontuberculous mycobacterial pulmonary disease2024 January;67(1)
Epidemiology and pathogenesis of scabies2023 December;66(12)
Epidemiology and diagnosis of inflammatory bowel diseases2021 September;64(9)
Updated view on the treatment of chronic obstructive pulmonary disease in Korea2021 March;64(3)
Anesthetic management of patients with chronic obstructive pulmonary disease2020 September;63(9)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
