서론
뇌졸중, 종양, 뇌염, 외상성뇌손상(traumatic brain injury) 등의 원인에 의해 두개내압(intracranial pressure, ICP)이 정상 범위(5-15 mmHg)를 초과하여 상승하면, 이차 뇌손상(secondary brain injury)이 발생할 수 있다[1-3]. 두개내압이 상승하면 뇌에 혈액을 공급하는 구동력(driving force)이 되는 뇌관류압(cerebral perfusion pressure, CPP)이 감소하여 허혈성 손상이 발생하거나, 뇌압 경사에 의한 뇌탈출로 물리적 뇌손상이 발생하게 된다. 따라서 급성 뇌질환에서는 두개내압을 측정하고, 평균동맥압(mean arterial pressure, MAP)과의 차이를 이용하여 뇌관류압을 추정하며, 이를 기반으로 환자 맞춤형 표적치료를 하는 것은 신경중환자 치료에서 매우 중요한 부분이다[3-5]. 이 논문에서는 두개내압 상승 시 뇌관류압의 중요성에 대해서 알아보고, 뇌관류압을 최적화하여 두개내압 상승을 조절하는 치료에 대해서 논하고자 한다.
두개내압 상승과 두개 내 순응도
두개내 순응도(intracranial compliance)는 뇌압 변화에 따른 뇌 부피의 변화로 정의한다(∆V/∆P). 뇌조직의 순응도가 높을 때는 두개내 병변의 부피가 증가하더라도 두개내압의 상승이 적지만, 점차로 부피가 더욱 증가하면 두개내 순응도가 저하되면서 두개뇌압이 지수곡선처럼 급격히 증가하게 된다[3,6]. 두개내 병변의 부종에 의해 부피가 증가하는 초기 단계에서는 보상작용에 의해 뇌척수액의 용적이 감소하면 두개내 부피의 총 합이 증가하지 않아 뇌압이 증가하지 않는다. 하지만 보상작용이 한계에 도달하게 되면 두개내 용적이 증가하여 두개내 순응도가 낮아지며 결국 뇌압이 증가하게 된다.
뇌관류압
뇌관류압은 뇌조직에 혈액을 공급하게 되는 유효 압력이며, 뇌혈류의 구동력이다. 뇌관류압은 평균동맥압과 두개내압의 차이로 계산한다(CPP=MAP-ICP). 따라서 뇌관류압은 평균동맥압이 낮아지거나 두개내압이 상승하면 감소하게 된다. 뇌관류압은 뇌혈류의 구동력이 되지만, 뇌관류압이 변하더라도 뇌혈류가 직선적으로 변하지는 않는다. 정상상태의 뇌에서는 혈압이 변하더라도 뇌관류압이 50-150 mmHg의 범위에서는 뇌혈관의 수축과 이완작용을 하여 뇌혈류를 일정하게 유지하는데, 이를 뇌혈류의 자동조절능(autoregulation)이라 한다[4,5,7-9]. 뇌혈류의 자동조절능이 정상일 때 혈압이 상승하면 뇌혈관이 수축하여 뇌혈류 증가를 막고, 혈압이 감소하면 혈관이 이완되어 뇌혈류 감소를 막아 항상 일정한 뇌혈류를 유지하게 한다. 만일 뇌관류압이 위의 범위를 벗어나는 경우에는 자동조절능이 소실되어 뇌혈류는 뇌관류압에 직접적으로 비례하게 된다(Figure 1) [5]. 이처럼 뇌관류압은 뇌혈류의 대리 표지자로서의 역할을 하므로 매우 중요한데, 두개내압을 측정해야만 직접 계산이 가능하다[2,4,5,7-9].
두개내압 상승 치료의 기준과 목표
두개내압과 뇌관류압의 관계 및 두개내압 상승의 치료기준에 대해서는 외상성뇌손상에서 시행된 연구결과를 차용하여 다른 질환에도 이용하고 있다. 두개내압 상승의 치료 시점은 일반적으로 20 mmHg로 알려져 왔는데, 2012년 무작위배정 임상연구에서 그 기준 수치가 변하게 되었다. 324명의 중증 외상성뇌손상 환자를 대상으로, 두개내압을 모니터하면서 두개내압이 20 mmHg 이상으로 상승하면 추가 치료를 하여 20 mmHg 이하로 유지하도록 한 치료군과 뇌 영상과 임상 검진을 바탕으로 치료를 진행한 대조군의 사이에 6개월째 예후와 사망률은 차이가 없었다[10]. 따라서 두개내압 20 mmHg라는 임계수치의 의미는 모든 환자에게 적용하는 절대적 기준치가 아님을 보여주었다. 그 이후 외상성 뇌손상 환자를 대상으로 한 후향적 연구에서, 두개내압 22 mmHg을 기준으로 판단할 때 불량한 예후를 정확하게 예측의 정도가 높아 두개내압 관리의 기준이 변하게 되었다[11,12]. 이처럼 여러 연구에서 두개내압이 상승한 외상성뇌 손상 환자에서 특정 두개내압 수치 이하로 유지하도록 치료하는 것이 환자의 예후에 도움된다는 근거는 부족하다. 따라서 특정 두개내압 이하로 관리하기 위한 목적으로 두개내압을 모니터링하는 것 보다는 환자의 뇌혈류와 자동조절능의 생리적 상태와 같은 요인들을 함께 고려하여 치료 목표를 세우는 것이 바람직하다[1,13-15].
두개내압 상승 치료의 기준과 목표: 뇌관류압
뇌관류압은 뇌혈류를 유지하는 구동력이므로 뇌손상 환자는 적절한 범위의 뇌관류압을 유지하여야 한다. 최적의 뇌관류압은 환자에 따라서 다양한데 이차 허혈손상을 최소화하기 위해서는 뇌관류압이 50-60 mmHg 이상으로 유지하도록 한다. 자동조절능이 유지되는 뇌관류압의 상단 범위는 150 mmHg이지만, 뇌관류압이 지나치게 높으면 과관류와 뇌부종의 악화 위험이 있어 대개 110 mmHg 이하로 유지도록 한다[7,8]. 외상성뇌손상 환자에서 뇌관류압을 50 mmHg 이상 유지한 환자군과 70-80 mmHg로 높게 유지한 환자들 간에 3개월, 6개월째 신경학적 예후에는 차이가 없었다[16]. 뇌관류압을 높게 유지하기 위해서는 추가적으로 승압제나 수액을 많이 사용하게 되므로 급성호흡곤란증후군의 발생율이 5배나 증가하여 현재는 최소 뇌관류압이 50 mmHg 이상만 유지하도록 권고하고, 불필요하게 높은 뇌관류압을 추천하지는 않는다[12,17]. 다만 개별 환자에 따라 적정 뇌관류압의 범위는 차이가 있을 수 있기 때문에 일률적인 두개내압이나 뇌관류압의 수치를 기준으로 환자를 치료를 하기 보다는 각 뇌의 자동조절능 정도를 고려하여 치료 계획을 세우는 것이 바람직하다.
두개내압 상승 시 치료의 첫 단계: 뇌관류압의 최적화
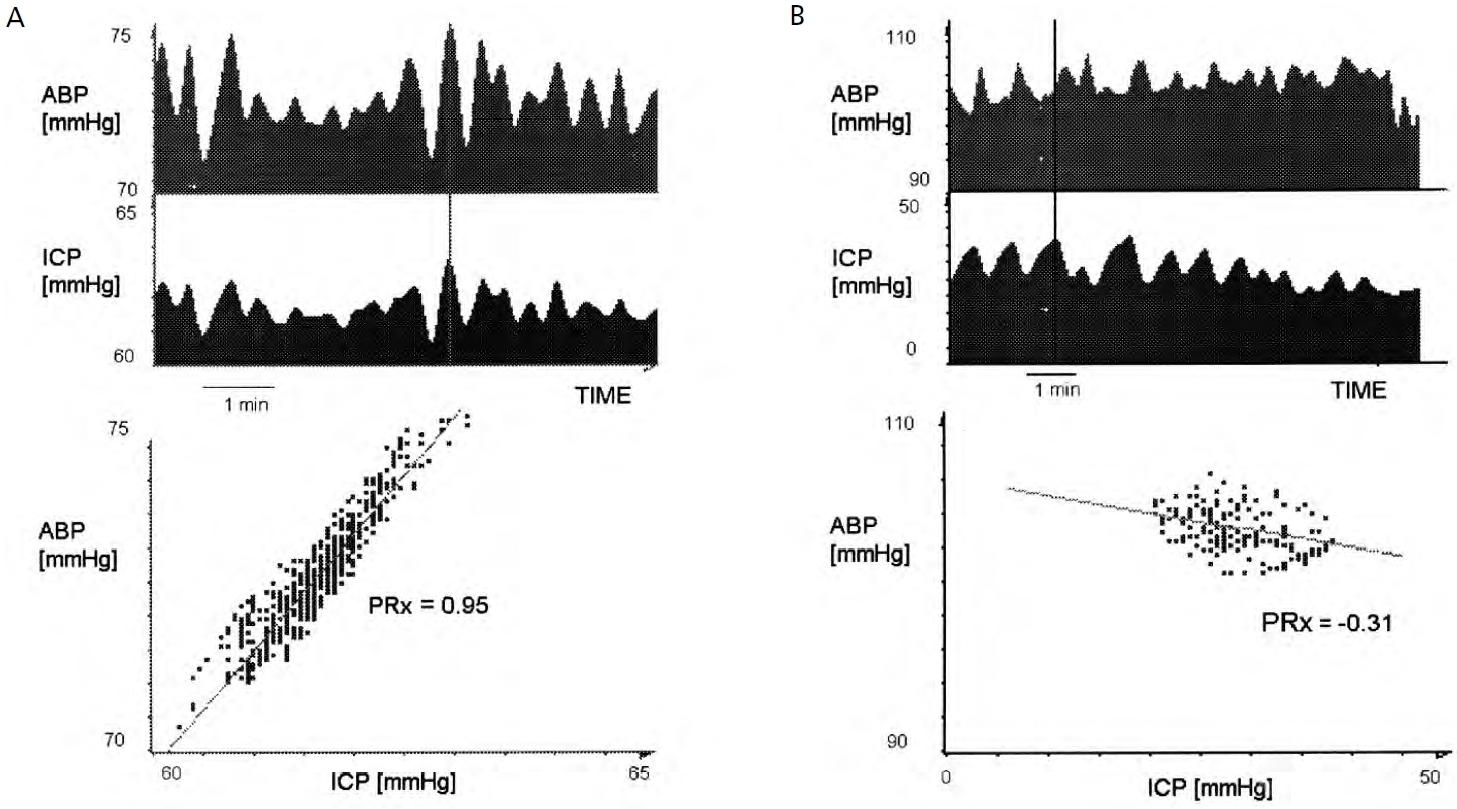
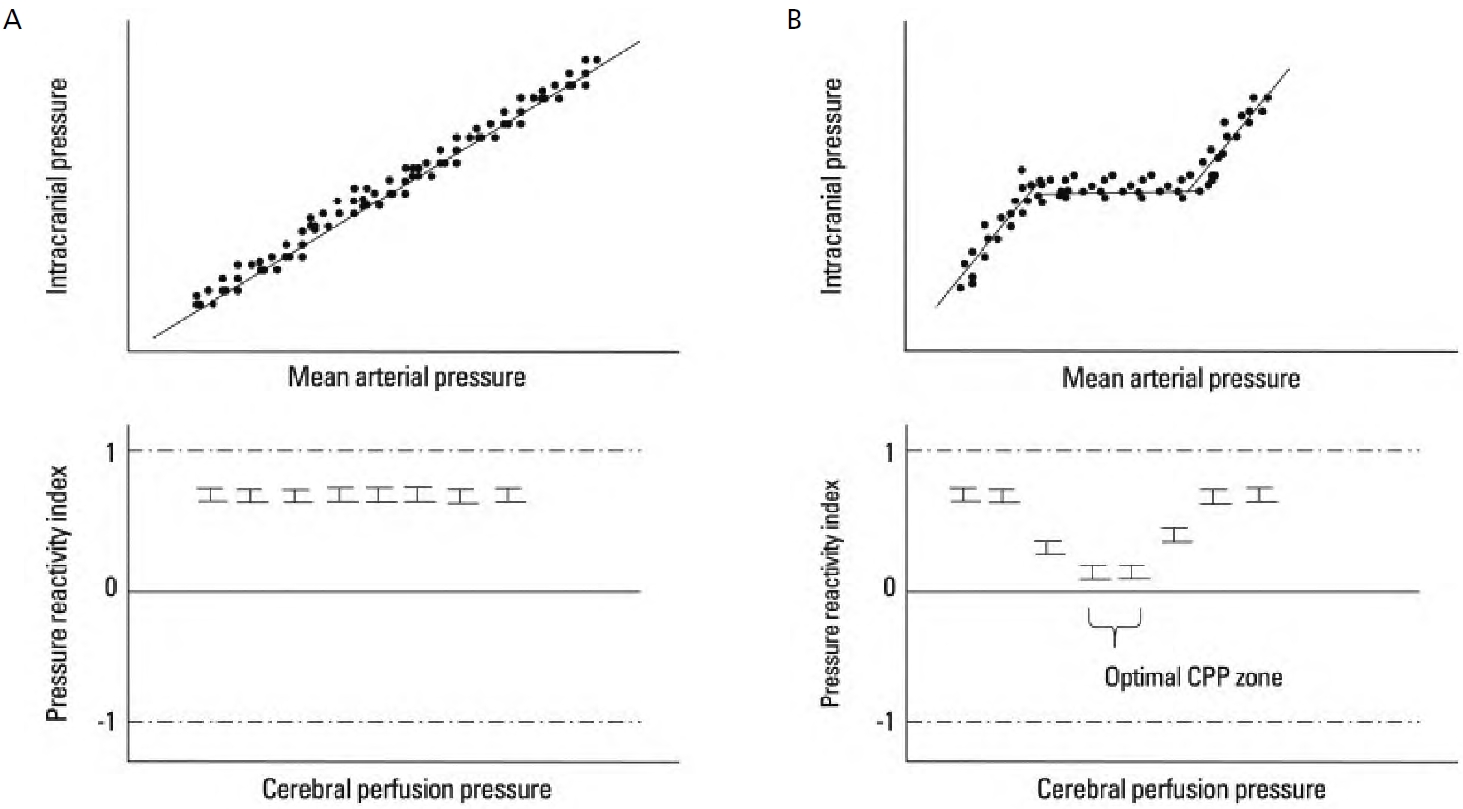
뇌혈류의 자동조절능이 유지되는 뇌관류압 범위라도 자동조절능의 하방경계에서는 혈압이 감소하면 뇌혈류를 유지하기 위해 혈관저항을 감소시켜야 하므로 뇌혈관이 확장되며, 이에 따라 뇌의 총 혈액량이 증가하고, 두개 내 용적이 증가하여 두개내압이 상승한다. 증가된 두개내압에 의해 뇌관류압은 더욱 저하되므로, 뇌혈류가 감소하지 않도록 혈관저항은 더욱 감소하면서 다시 두개내압이 증가하는 연쇄반응이 발생하는데, 이를 혈관확장연쇄반응(vasodilatory cascade)이라고 하며, 중환자실에서 목격하는 두개내압 상승의 고원파(plateau wave)의 주된 발생 기전이 된다. 또한 자동조절능이 손상된 경우에는 혈압이 감소하면 뇌혈류가 혈압에 비례하여 감소하므로 이차 뇌허혈의 위험이 증가하게 된다. 따라서 두개내압이 상승한 환자에서 혈압이 지나치게 낮은 경우에는 혈압을 상승시키는 치료를 첫 단계로 고려해야 하며 이를 뇌관류압의 최적화라고 한다. 두개내압이 상승한 환자에서 지나치게 뇌관류압이 높다면, 과관류에 의한 부종악화를 막기위해서 적절한 수준으로 혈압을 조절하여 뇌관류압을 낮추어야 할 수도 있다. 최적의 뇌관류압을 유지하기 위해 사용할 수 있는 승압제로는 phenylephrine (2-11 μg/kg/min), dopamine (5-30 μg/kg/min), norepinephrine (0.01-0.6 μg/kg/min) 등을 고려할 수 있고, 심장에 부담을 덜기 위해서는 말초혈관에만 작용하는 phenylephrine을 선택하기도 한다. 혈압이 높아 조절이 필요하다면 labetalol (5-150 μg/kg/min)이나 nicardipine (5-25 mg/hr)의 투약을 고려할 수 있다. 다만 nitroprusside는 뇌혈관 확장효과를 유발하여 뇌압 상승을 악화시킬 수 있기 때문에 사용하지 않는 것이 좋다. 혈압이 낮은 상태에서 두개내압을 조절하기 위해 고삼투압제제(만니톨과 고장성 식염수 등)를 빠르게 주사하는 경우에는 일시적인 혈압 감소를 유발하고, 이에 의해 혈관확장연쇄반응이 발생할 위험이 있기 때문에 항상 뇌관류압을 최적화한 후에 사용하도록 한다[2,8,15,18,19]. 뇌손상 환자에서 혈압과 두개내압을 연속 모니터링 하고 있다면, 혈압과 두개내압을 이용하여 자동조절능 반응을 수치화 한 압력반응지표(pressure reactivity index)를 계산하여 그 값을 기반으로 최적의 뇌관류압을 확인하여 환자별 맞춤형 치료 계획을 세울 수 있다(Figures 2, 3) [5,20-22].
결론
뇌질환으로 인하여 두개내압이 상승하면 이차 뇌손상의 발생위험도가 높아지고, 이로 인해 환자들의 신경학적 예후가 불량하게 된다. 상승된 두개내압을 조절하기 위해 다양한 치료 방법을 고려할 때 환자의 뇌관류압이 현재 적절한 상태인지를 가장 먼저 생각하여야 한다. 동일한 두개내압이라고 할지라도 뇌관류압이 낮으면 뇌허혈의 위험과 함께 낮은 혈압에 의한 뇌압 상승의 연쇄반응이 발생할 수 있기 때문이다. 이처럼 최적의 뇌관류압을 유지할 수 있도록 개별 환자에 따른 치료 목표를 세우고 뇌압상승 치료를 진행한다면 뇌손상 환자의 치료와 신경학적 예후에 도움이 될 것이다.