




 |
 |
| J Korean Med Assoc > Volume 55(7); 2012 > Article |
Abstract
Cancer pain is among the most undesirable side effects and complications for cancer patients. Severe cancer pain acts as physical and psychological stress and makes it difficult for patients to perform daily activities. Uncontrolled cancer pain can be emotionally devastating to patients. However, cancer pain can be controlled with pharmacologic treatment. Traditionally, cancer pain was treated according to the WHO three-step analgesic ladder based on the severity of pain. Recently, it has become to administer weak opioids as well as non-opioid analgesics to patients with mild pain. For moderate pain, weak opioids or strong opioids can be used. Non-opioid analgesics and adjuvant analgesics can be used as an adjuvant to opioids for all severities of cancer pain. Effective cancer pain management depends on the proper selection of a drug, dose, and route and depends on treatment of common side effects associated with the medication. The usage of medication should be individualized to each patient. If necessary, we may use other modalities such as radiotherapy, nerve block, and non-pharmacologic interventions for cancer pain control. The goal of treatment of cancer pain is to obtain complete or partial pain relief with tolerable side effects of the medication, and ultimately, to improve the quality of life of cancer patients.
References
1. Ministry of Health & Welfare. Cancer pain management guideline 2012;5th ed. Seoul: Ministry of Health & Welfare.
2. Park JM. Korean Society of Anesthesiologists Anesthesiologists. Cancer pain. Anesthesiology & pain medicine 2010;2nd ed. Seoul: Ryo Moon Gak. 379-398.
3. Azevedo Sao Leao Ferreira K, Kimura M, Jacobsen Teixeira M. The WHO analgesic ladder for cancer pain control, twenty years of use. How much pain relief does one get from using it? Support Care Cancer 2006;14:1086-1093.
4. National Comprehensive Cancer Network. NCCN clinical practice guideline in oncology: adult cancer pain 2012;1:Fort Washington: National Comprehensive Cancer Network.
5. American Pain Society Quality of Care Committee. Quality improvement guidelines for the treatment of acute pain and cancer pain. JAMA 1995;274:1874-1880.
6. Yoon DM. Korean Pain Society. Cancer pain. Pain medicine 2007;3rd ed. Seoul: Koonja. 425-442.
7. Harris JT, Suresh Kumar K, Rajagopal MR. Intravenous morphine for rapid control of severe cancer pain. Palliat Med 2003;17:248-256.
8. Portenoy RK. Treatment of cancer pain. Lancet 2011;377:2236-2247.
9. Ripamonti CI, Bandieri E, Roila F. ESMO Guidelines Working Group. Management of cancer pain: ESMO Clinical Practice Guidelines. Ann Oncol 2011;22:Suppl 6. vi69-vi77.
10. Stockler M, Vardy J, Pillai A, Warr D. Acetaminophen (paracetamol) improves pain and well-being in people with advanced cancer already receiving a strong opioid regimen: a randomized, double-blind, placebo-controlled cross-over trial. J Clin Oncol 2004;22:3389-3394.
11. Israel FJ, Parker G, Charles M, Reymond L. Lack of benefit from paracetamol (acetaminophen) for palliative cancer patients requiring high-dose strong opioids: a randomized, double-blind, placebo-controlled, crossover trial. J Pain Symptom Manage 2010;39:548-554.
12. McNicol E, Strassels SA, Goudas L, Lau J, Carr DB. NSAIDS or paracetamol, alone or combined with opioids, for cancer pain. Cochrane Database Syst Rev 2005;1):CD005180.
13. Bruera E, Kim HN. Cancer pain. JAMA 2003;290:2476-2479.
14. Stevens RA, Ghazi SM. Routes of opioid analgesic therapy in the management of cancer pain. Cancer Control 2000;7:132-141.
15. Ripamonti C, Bandieri E. Pain therapy. Crit Rev Oncol Hematol 2009;70:145-159.
16. Foley KM. The treatment of pain in the patient with cancer. CA Cancer J Clin 1986;36:194-215.
17. Kornick CA, Santiago-Palma J, Khojainova N, Primavera LH, Payne R, Manfredi PL. A safe and effective method for converting cancer patients from intravenous to transdermal fentanyl. Cancer 2001;92:3056-3061.
18. Meuser T, Pietruck C, Radbruch L, Stute P, Lehmann KA, Grond S. Symptoms during cancer pain treatment following WHO-guidelines: a longitudinal follow-up study of symptom prevalence, severity and etiology. Pain 2001;93:247-257.
19. McNicol E, Horowicz-Mehler N, Fisk RA, Bennett K, Gialeli-Goudas M, Chew PW, Lau J, Carr D. Americal Pain Society. Management of opioid side effects in cancer-related and chronic noncancer pain: a systematic review. J Pain 2003;4:231-256.
20. Holzer P, Ahmedzai SH, Niederle N, Leyendecker P, Hopp M, Bosse B, Spohr I, Reimer K. Opioid-induced bowel dysfunction in cancer-related pain: causes, consequences, and a novel approach for its management. J Opioid Manag 2009;5:145-151.
21. Stone P, Minton O. European Palliative Care Research collaborative pain guidelines. Central side-effects management: what is the evidence to support best practice in the management of sedation, cognitive impairment and myoclonus? Palliat Med 2011;25:431-441.
22. Tassinari D, Drudi F, Carloni F, Possenti C, Santelmo C, Castellani C. Neuropathic pain in oncology. Novel evidence for clinical practice. Recenti Prog Med 2011;102:220-227.
23. Saarto T, Wiffen PJ. Antidepressants for neuropathic pain: a Cochrane review. J Neurol Neurosurg Psychiatry 2010;81:1372-1373.
24. Wiffen P, Collins S, McQuay H, Carroll D, Jadad A, Moore A. Anticonvulsant drugs for acute and chronic pain. Cochrane Database Syst Rev 2005;3):CD001133.
25. Mercadante SL, Berchovich M, Casuccio A, Fulfaro F, Mangione S. A prospective randomized study of corticosteroids as adjuvant drugs to opioids in advanced cancer patients. Am J Hosp Palliat Care 2007;24:13-19.
26. Vasudev NS, Brown JE. Medical management of metastatic bone disease. Curr Opin Support Palliat Care 2010;4:189-194.
27. Slatkin NE, Rhiner M. Ketamine in the treatment of refractory cancer pain: case report, rationale, and methodology. J Support Oncol 2003;1:287-293.
Figure 1
Managenent of cancer pain with opioid analgesics. IV, intravenous. *If there is no response after 2-3 cycles, reassess the pain (e.g., neuropathic pain) and consider the use of adjuvant analgesics and pain specialty consultation.
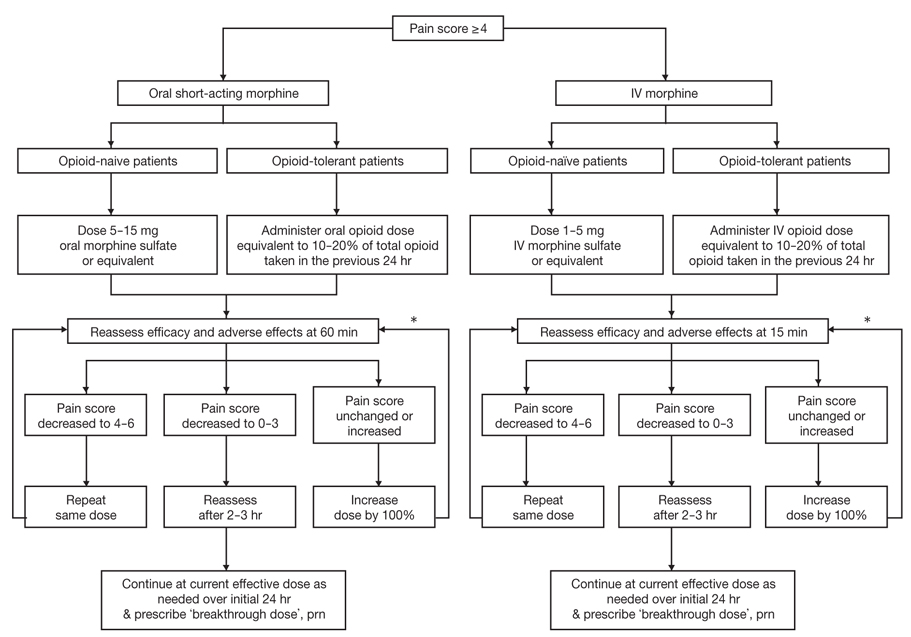
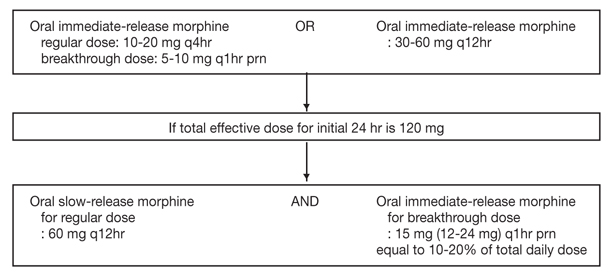
Figure 2
Example of titration of total daily dose of morphine. From Ministry of Health & Welfare. Cancer pain management guideline. Seoul: Ministry of Health & Welfare; 2012 [1].
- TOOLS
-
- Share :
-





-
METRICS

-
Related articles in
J Korean Med Assoc -
Surgical treatment of esophageal cancer2024 February;67(2)
Intratympanic injection for treatment of inner ear diseases2023 October;66(10)
Pharmacological treatment of Ménière disease2023 October;66(10)
Diagnosis and pharmacological management of allergic conjunctivitis2023 September;66(9)
Recent trends in the management of anterior knee pain2023 August;66(8)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
