





 |
 |
| J Korean Med Assoc > Volume 51(5); 2008 > Article |
Abstract
Cerebral palsy is a disorder of movement and posture that arises from a congenital or acquired lesion of the immature brain. While the underlying cause is static, the musculoskeletal manifestations are progressive overtime. A variety of gait abnormalities are common, and orthopedic surgery typically is indicated when contractures or deformities decrease functions, cause pain, or interfere with activities of daily life. Surgical procedures should be scheduled to minimize the number of hospitalizations and interference with school and social activities. They can be divided into several groups of procedures; (1) to correct static or dynamic deformity, (2) balance muscle power across a joint, (3) reduce spasticity, and (4) stabilize uncontrollable joints. The clinical decision-making paradigm, consisting of clinical history, physical examination, diagnostic imaging, quantitative gait analysis, and examination under anesthesia makes it possible for single stage multi-level surgeries to reduce the long-term morbidity.
References
1. Sussman MD, Aiona MD. Treatment of spastic diplegia in patients with cerebral palsy. J Pediatr Orthop 2004;13:S1-S12.
2. Bache CE, Selber P, Graham HK. The management of spastic diplegia. Curr Orthop 2003;17:88-104.
3. Novacheck TF, Gage JR. Orthopaedic management of spasticity in cerebral palsy. Childs Nerv Syst 2007;23:1015-1031.
4. Davids JR, Õunpuu S, DeLuca PA, Davis RB. Optimization of walking ability of children with cerebral palsy. J Bone Joint Surg Am 2003;85:2224-2234.
5. Dreher T, Wolf S, Braatz F, Patikas D, Döderlein L. Internal rotation gait in spastic diplegia-Critical considerations for the femoral derotation osteotomy. Gait Posture 2007;26:25-31.
6. Sutherland DH, Zilberfarb JL, Kaufman KR, Wyatt MP, Chambers HG. Psoas release at the pelvic brim in ambulatory patients with cerebral palsy: operative technique and functional outcome. J Pediatr Orthop 1997;17:563-570.
7. Ounpuu S, Muik E, Davis RB 3rd, Gage JR, DeLuca PA. Rectus femoris surgery in children with cerebral palsy. Part I: the effect of rectus femoris transfer location on knee motion. J Pediatr Orthop 1993;13:325-330.
8. Rodda JM, Graham HK, Nattrass GR, Galea MP, Baker R, Wolfe R. Correction of severe crouch gait in patients with spastic diplegia with use of multilevel orthopaedic surgery. J Bone Joint Surg Am 2006;88:2653-2664.
9. Park KB, Park HW, Lee KS, Joo SY, Kim HW. Changes of Dynamic Foot Pressure after Surgical Treatment of Valgus Deformity of Hindfoot in Cerebral Palsy. J Bone Joint Surgery Am 2008;(in press).
10. Seniorou M, Thompson N, Harrington M, Theologis T. Recovery of muscle strength following multi-level orthopaedic surgery in diplegic cerebral palsy. Gait Posture 2007;26:475-481.
Figure 1
Lever-arm dysfunctions at the hip, knee, and the foot produce hip dislocation, patellar alta, and pathologic flatfoot, respectively.
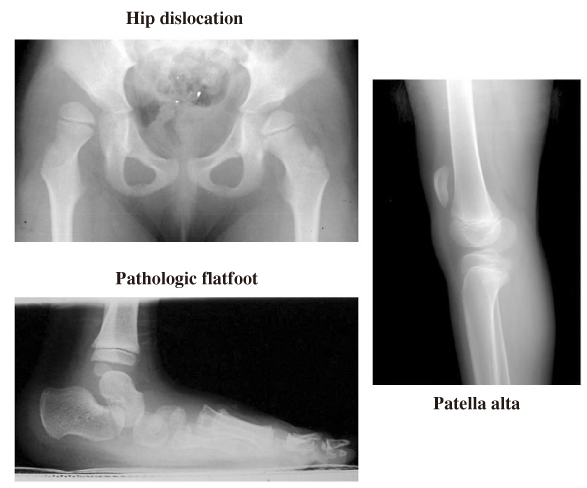
Figure 2
Findings of gait analysis include temporospatial, kinematic, kinetic, and electromyographic parameters.
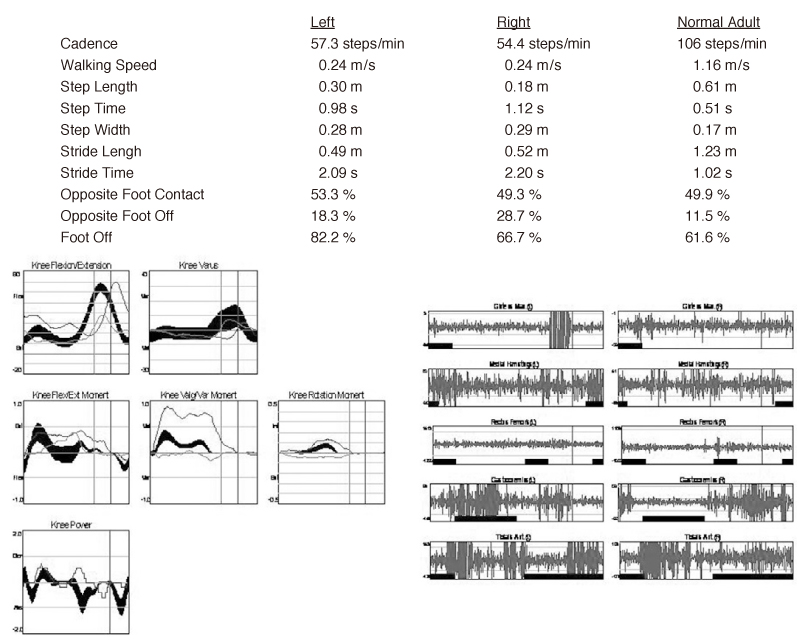
Figure 3
Younger child with spastic diplegia. He walks on his toes in equinus with extended hips and knees.

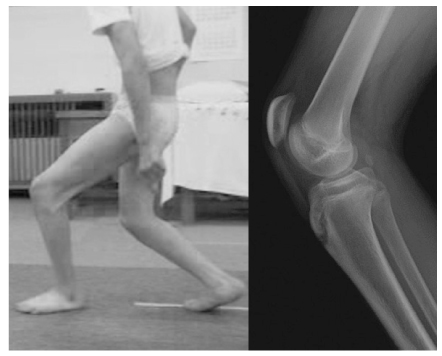
Figure 5
Genu recurvatum gait is generally secondary to pes equinus and incompetent ankle plantarflexion-knee extension couple.

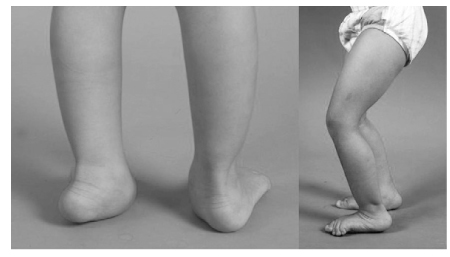
Figure 6
A child showing jumping gait pattern with hips, knees, and ankles in flexion. The patient needs to hold hands or use a walker, and rarely they can balance themselves.

- TOOLS
-
- Share :
-





-
METRICS

-
- 0 Crossref
- Scopus
- 1,063 View
- 7 Download
-

-
Related articles in
J Korean Med Assoc
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
