




 |
 |
| J Korean Med Assoc > Volume 54(2); 2011 > Article |
Abstract
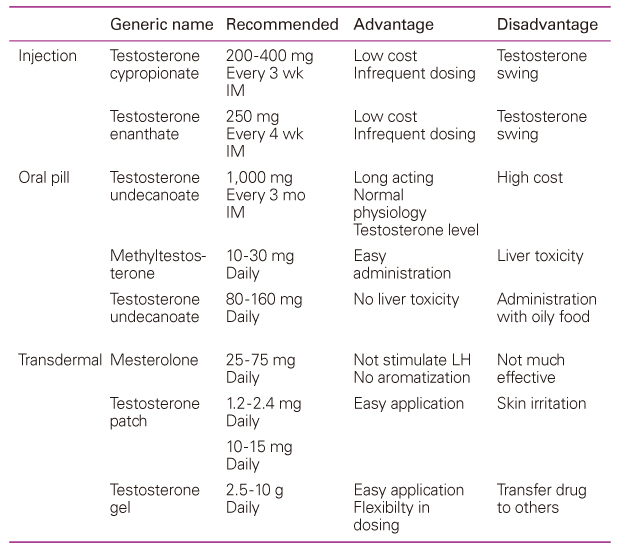
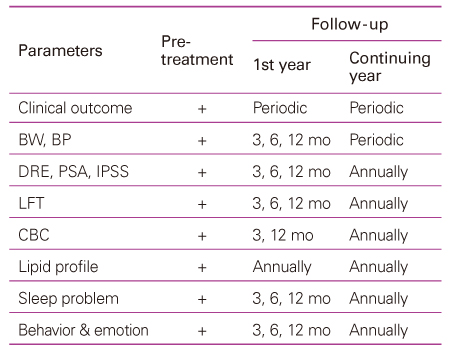
Since the elderly population has been increasing recently in our country, old male patients with testosterone deficiency syndrome (TDS) with a significantly decreasing quality of life are becoming increasingly common. TDS in males is defined as a biochemical syndrome associated with advancing age and characterized by clinical manifestation and a deficiency in the serum testosterone level. These patients should be treated with extrinsic testosterone to improve quality of life. TDS in males should be diagnosed in the case of clinical manifestation with serum total testosterone <8 nmol/L (230 ng/dL) or calculated free testosterone <225 pmol/L (65 pg/mL) but not diagnosed in the case of serum total testosterone >12 nmol/L (350 ng/dL). Products for testosterone replacement therapy (TRT) are administrated orally, transdermally, and through injectable preparations. Daily testosterone undecanoate is widely used for oral administration with good results and no hepatotoxicity. Short-acting intramuscular preparations are very effective but show wide swings in the resulting supra-physiological level of serum testosterone. Long-acting intramuscular preparations is also very effective and lasting for 3 months with normal physiologic levels. Many products for TRT on the market are effective and generally safe. However, those have a few significant adverse events each other. The ideal product should have notable effectsand few side effects, (such as selective androgen receptor modulators), be easy to administrate, maintain physiologic serum concentration, and be inexpensive. TDS in males can easily be correct by TRT. However, the advantages and disadvantages of the individual products and follow-up management of complicated adverse events should be understood before starting and maintaining TRT.
References
1. Araujo AB, Esche GR, Kupelian V, O'Donnell AB, Travison TG, Williams RE, Clark RV, McKinlay JB. Prevalence of sympto-matic androgen deficiency in men. J Clin Endocrinol Metab 2007;92:4241-4247.
2. Buvat J, Maggi M, Gooren L, Guay AT, Kaufman J, Morgentaler A, Schulman C, Tan HM, Torres LO, Yassin A, Zitzmann M. Endocrine aspects of male sexual dysfunctions. J Sex Med 2010;7(4 Pt 2):1627-1656.
3. Isidori AM, Giannetta E, Gianfrilli D, Greco EA, Bonifacio V, Aversa A, Isidori A, Fabbri A, Lenzi A. Effects of testosterone on sexual function in men: results of a meta-analysis. Clin Endocrinol (Oxf) 2005;63:381-394.
4. Calof OM, Singh AB, Lee ML, Kenny AM, Urban RJ, Tenover JL, Bhasin S. Adverse events associated with testosterone replacement in middle-aged and older men: a meta-analysis of randomized, placebo-controlled trials. J Gerontol A Biol Sci Med Sci 2005;60:1451-1457.
5. Nieschlag E, Swerdloff R, Behre HM, Gooren LJ, Kaufman JM, Legros JJ, Lunenfeld B, Morley JE, Schulman C, Wang C, Weidner W, Wu FC. International Society of Andrology (ISA). International Society for the Study of the Aging Male (ISSAM). European Association of Urology (EAU). Investigation, treatment and monitoring of late-onset hypogonadism in males: ISA, ISSAM, and EAU recommendations. Eur Urol 2005;48:1-4.
6. Bhasin S, Cunningham GR, Hayes FJ, Matsumoto AM, Snyder PJ, Swerdloff RS, Montori VM. Testosterone therapy in adult men with androgen deficiency syndromes: an endocrine society clinical practice guideline. J Clin Endocrinol Metab 2006;91:1995-2010.
7. Nieschlag E, Swerdloff R, Behre HM, Gooren LJ, Kaufman JM, Legros JJ, Lunenfeld B, Morley JE, Schulman C, Wang C, Weidner W, Wu FC. Investigation, treatment, and monitoring of late-onset hypogonadism in males: ISA, ISSAM, and EAU recommendations. J Androl 2006;27:135-137.
8. Wang C, Nieschlag E, Swerdloff RS, Behre H, Hellstrom WJ, Gooren LJ, Kaufman JM, Legros JJ, Lunenfeld B, Morales A, Morley JE, Schulman C, Thompson IM, Weidner W, Wu FC. ISA, ISSAM, EAU, EAA and ASA recommendations: investigation, treatment and monitoring of late-onset hypogonadism in males. Aging Male 2009;12:5-12.
9. Wang C, Nieschlag E, Swerdloff R, Behre HM, Hellstrom WJ, Gooren LJ, Kaufman JM, Legros JJ, Lunenfeld B, Morales A, Morley JE, Schulman C, Thompson IM, Weidner W, Wu FC. ISA, ISSAM, EAU, EAA and ASA recommendations: investigation, treatment and monitoring of late-onset hypogonadism in males. Int J Impot Res 2009;21:1-8.
10. Bhasin S, Cunningham GR, Hayes FJ, Matsumoto AM, Snyder PJ, Swerdloff RS, Montori VM. Task Force, Endocrine Society. Testosterone therapy in men with androgen deficiency syndromes: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2010;95:2536-2559.
11. Morales A, Schulman CC, Tostain J, C W Wu F. Testosterone deficiency syndrome (TDS) needs to be named appropriately: the importance of accurate terminology. Eur Urol 2006;50:407-409.
12. Derby CA, Zilber S, Brambilla D, Morales KH, McKinlay JB. Body mass index, waist circumference and waist to hip ratio and change in sex steroid hormones: the Massachusetts Male Ageing Study. Clin Endocrinol (Oxf) 2006;65:125-131.
13. Morales A, Spevack M, Emerson L, Kuzmarov I, Casey R, Black A, Tremblay R. Adding to the controversy: pitfalls in the diagnosis of testosterone deficiency syndromes with questionnaires and biochemistry. Aging Male 2007;10:57-65.
14. Vermeulen A. Hormonal cut-offs of partial androgen deficiency: a survey of androgen assays. J Endocrinol Invest 2005;28:3 Suppl. 28-31.
15. Rosner W, Auchus RJ, Azziz R, Sluss PM, Raff H. Position statement: utility, limitations, and pitfalls in measuring testosterone: an Endocrine Society position statement. J Clin Endocrinol Metab 2007;92:405-413.
16. Practice Committee of the American Society for Reproductive Medicine. Treatment of androgen deficiency in the aging male. Fertil Steril 2006;86:5 Suppl 1. S236-S240.
17. Turchi P, Simi S, Pescatori ES. Testosterone replacement therapy in male late onset hypogonadism: available pharma-cological strategies. J Endocrinol Invest 2005;28:11 Suppl Proceedings. 61-68.
18. Barqawi A, Crawford ED. Testosterone replacement therapy and the risk of prostate cancer. Is there a link? Int J Impot Res 2006;18:323-328.
19. Rhoden EL, Morgentaler A. Risks of testosterone-replace-ment therapy and recommendations for monitoring. N Engl J Med 2004;350:482-492.
20. Snyder PJ, Peachey H, Berlin JA, Rader D, Usher D, Loh L, Hannoush P, Dlewati A, Holmes JH, Santanna J, Strom BL. Effect of transdermal testosterone treatment on serum lipid and apolipoprotein levels in men more than 65 years of age. Am J Med 2001;111:255-260.
- TOOLS
-
- Share :
-





- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
