





 |
 |
| J Korean Med Assoc > Volume 54(1); 2011 > Article |
Abstract
Breast reconstruction with autologous tissue has been generally accepted as a reliable procedure, the preferred donor site being lower abdominal tissue. To sacrifice the minimal amount of muscle tissue and to reduce donor site morbidity, the concept of a perforator flap was applied to the fields of breast reconstruction, such as the deep inferior epigastric artery perforator (DIEAp) flap. The DIEAp flap provides essentially the same soft tissue components as the transverse rectus abdominis muscle (TRAM) flap while significantly reducing harvesting of the rectus muscle from the abdominal wall, thereby minimizing donor site morbidity; which includes abdominal weakness, hernia, and postoperative pain, with decreased recovery time. However, there are some concerns about the tedious and risky dissection of intramuscular perforators, and the variable vascularity of the flap supplied by tiny perforators. According to our novel flap harvesting techniques, using bipolar electrocauterization for intramuscular dissection is useful in preventing injury to the tiny perforators. Including some fibers of rectus muscle and soft tissue without full isolation and skeletonization around the pedicles is also useful for prevention of vascular injury and intraoperative vessel spasms. Moreover, the flap must include 2 to 3 reliable perforators, regardless of lateral or medial rows, for prevention of postoperative fat necrosis. The superficial inferior epigastric vein can provide additional venous drainage. These surgical tips can aid in overcoming the pitfalls of the DIEA perforator flap in breast reconstruction. The DIEAp flap is an excellent choice for breast reconstruction. According to our experience, it has been shown to be a safe and reliable method for providing good results and patient satisfaction with minimal donor morbidity in breast reconstruction.
References
1. Koshima I, Inagawa K, Urushibara K, Moriguchi T. Paraumbilical perforator flap without deep inferior epigastric vessels. Plast Reconstr Surg 1998;102:1052-1057.
2. LoTempio MM, Allen RJ. Breast reconstruction with SGAP and IGAP flaps. Plast Reconstr Surg 2010;126:393-401.
3. Chang DW, Youssef A, Cha S, Reece GP. Autologous breast reconstruction with the extended latissimus dorsi flap. Plast Reconstr Surg 2002;110:751-759.
4. Blondeel PN, Boeckx WD. Refinements in free flap breast reconstruction: the free bilateral deep inferior epigastric perforator flap anastomosed to the internal mammary artery. Br J Plast Surg 1994;47:495-501.
5. Hamdi M, Blondeel P, Van Landuyt K, Tondu T, Monstrey S. Bilateral autogenous breast reconstruction using perforator free flaps: a single center's experience. Plast Reconstr Surg 2004;114:83-89.
6. Granzow JW, Levine JL, Chiu ES, Allen RJ. Breast reconstruction with the deep inferior epigastric perforator flap: history and an update on current technique. J Plast Reconstr Aesthet Surg 2006;59:571-579.
7. Lipa JE. Breast reconstruction with free flaps from the abdominal donor site: TRAM, DIEAP, and SIEA flaps. Clin Plast Surg 2007;34:105-121.
8. Tseng CY, Lipa JE. Perforator flaps in breast reconstruction. Clin Plast Surg 2010;37:641-654.
9. Craigie JE, Allen RJ, DellaCroce FJ, Sullivan SK. Autogenous breast reconstruction with the deep inferior epigastric perforator flap. Clin Plast Surg 2003;30:359-369.
10. Koshima I, Soeda S. Inferior epigastric artery skin flaps without rectus abdominis muscle. Br J Plast Surg 1989;42:645-648.
11. Kim JT. Latissimus dorsi perforator flap. Clin Plast Surg 2003;30:403-431.
12. Kim JT, Kim SK. Hand resurfacing with the superthin latissimus dorsi perforator-based free flap. Plast Reconstr Surg 2003;111:366-370.
13. Koshima I, Inagawa K, Urushibara K, Ohtsuki M, Moriguchi T. Deep inferior epigastric perforator dermal-fat or adiposal flap for correction of craniofacial contour deformities. Plast Reconstr Surg 2000;106:10-15.
14. Koshima I, Nanba Y, Tsutsui T, Takahashi Y, Watanabe A, Ishii R. Free perforator flap for the treatment of defects after resection of huge arteriovenous malformations in the head and neck regions. Ann Plast Surg 2003;51:194-199.
15. Kuo YR, Jeng SF, Wei FC, Su CY, Chien CY. Functional reconstruction of complex lip and cheek defect with free composite anterolateral thigh flap and vascularized fascia. Head Neck 2008;30:1001-1006.
16. Imai R, Matsumura H, Tanaka K, Uchida R, Watanabe K. Comparison of Doppler sonography and multidetector-row computed tomography in the imaging findings of the deep inferior epigastric perforator artery. Ann Plast Surg 2008;61:94-98.
17. Mun GH, Kim HJ, Cha MK, Kim WY. Impact of perforator mapping using multidetector-row computed tomographic angiography on free thoracodorsal artery perforator flap transfer. Plast Reconstr Surg 2008;122:1079-1088.
18. Masia J, Clavero JA, Larranaga JR, Alomar X, Pons G, Serret P. Multidetector-row computed tomography in the planning of abdominal perforator flaps. J Plast Reconstr Aesthet Surg 2006;59:594-599.
19. Mathes DW, Neligan PC. Current techniques in preoperative imaging for abdomen-based perforator flap microsurgical breast reconstruction. J Reconstr Microsurg 2010;26:3-10.
20. Hijjawi JB, Blondeel PN. Advancing deep inferior epigastric artery perforator flap breast reconstruction through multidetector row computed tomography: an evolution in preoperative imaging. J Reconstr Microsurg 2010;26:11-20.
21. Feng LJ. Recipient vessels in free-flap breast reconstruction: a study of the internal mammary and thoracodorsal vessels. Plast Reconstr Surg 1997;99:405-416.
22. Serletti JM, Moran SL, Orlando GS, Fox I. Thoracodorsal vessels as recipient vessels for the free TRAM flap in delayed breast reconstruction. Plast Reconstr Surg 1999;104:1649-1655.
23. Majumder S, Batchelor AG. Internal mammary vessels as recipients for free TRAM breast reconstruction: aesthetic and functional considerations. Br J Plast Surg 1999;52:286-289.
24. Sacks JM, Chang DW. Rib-sparing internal mammary vessel harvest for microvascular breast reconstruction in 100 consecutive cases. Plast Reconstr Surg 2009;123:1403-1407.
25. Parrett BM, Caterson SA, Tobias AM, Lee BT. The rib-sparing technique for internal mammary vessel exposure in microsurgical breast reconstruction. Ann Plast Surg 2008;60:241-243.
26. Rad AN, Flores JI, Rosson GD. Free DIEP and SIEA breast reconstruction to internal mammary intercostal perforating vessels with arterial microanastomosis using a mechanical coupling device. Microsurgery 2008;28:407-411.
27. Munhoz AM. Internal mammary perforator recipient vessels for breast reconstruction using free TRAM, DIEP, and SIEA flaps. Plast Reconstr Surg 2008;122:315-316.
28. Wu LC, Iteld L, Song DH. Supercharging the transverse rectus abdominis musculocutaneous flap: breast reconstruction for the overweight and obese population. Ann Plast Surg 2008;60:609-613.
29. Marck KW, van der Biezen JJ, Dol JA. Internal mammary artery and vein supercharge in TRAM flap breast reconstruction. Microsurgery 1996;17:371-374.
30. Baumann DP, Lin HY, Chevray PM. Perforator number predicts fat necrosis in a prospective analysis of breast reconstruction with free TRAM, DIEP, and SIEA flaps. Plast Reconstr Surg 2010;125:1335-1341.
31. Kim JT, Kim CY, Kim YH. T-anastomosis in microsurgical free flap reconstruction: an overview of clinical applications. J Plast Reconstr Aesthet Surg 2008;61:1157-1163.
32. Kim JT, Kim YH. Initial temporary vascular insufficiency in latissimus dorsi and thoracodorsal perforator flaps. Plast Reconstr Surg 2009;124:6 Suppl. e408-e418.
33. Bailey SH, Saint-Cyr M, Wong C, Mojallal A, Zhang K, Ouyang D, Arbique G, Trussler A, Rohrich RJ. The single dominant medial row perforator DIEP flap in breast reconstruction: three-dimensional perforasome and clinical results. Plast Reconstr Surg 2010;126:739-751.
34. Schaverien MV, Perks AG, McCulley SJ. Comparison of outcomes and donor-site morbidity in unilateral free TRAM versus DIEP flap breast reconstruction. J Plast Reconstr Aesthet Surg 2007;60:1219-1224.
35. Chen CM, Halvorson EG, Disa JJ, McCarthy C, Hu QY, Pusic AL, Cordeiro PG, Mehrara BJ. Immediate postoperative complications in DIEP versus free/muscle-sparing TRAM flaps. Plast Reconstr Surg 2007;120:1477-1482.
Figure 1
Evolution of flap concept. The conventional flap was based on source vessel (blue dots) and it has been advanced to the branch (red dots) and finally to the perforator-based concept (green dots). Therefore, more selective tissues are harvested to preserve more tissues in donor site. P, perforator.
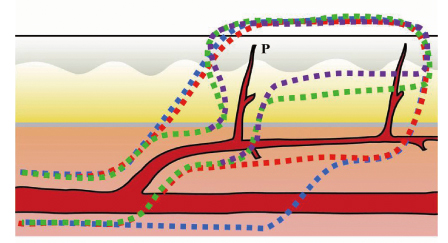
Figure 2
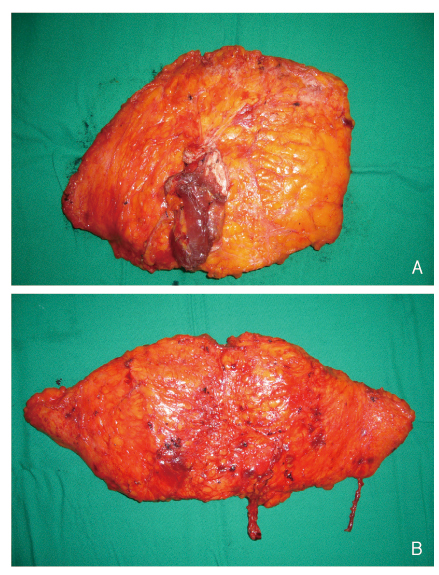
Comparison of conventional bulky transverse rectus abdominis muscle flap (A) and deep inferior epigastric artery perforator flap based on perforators (B).
- TOOLS
-
- Share :
-





-
METRICS

-
- 0 Crossref
- Scopus
- 1,425 View
- 5 Download
-

-
Related articles in
J Korean Med Assoc -
Breast reconstruction using implants2011 January;54(1)
Breast reconstruction using extended latissimus dorsi muscle flap2011 January;54(1)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
