



 |
 |
| J Korean Med Assoc > Volume 53(10); 2010 > Article |
Abstract
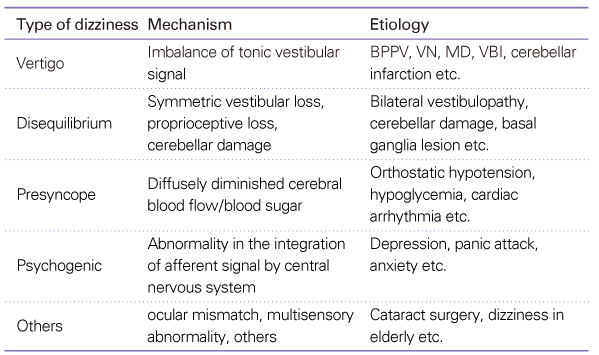
Dizziness is a very common symptom encountered by primary care physicians. Dizziness can be divided into five subgroups according to symptoms. These subgroups can be determined by a patient's history and allow the physician to deduce the etiology. A careful and systematic approach to dizzy patients is the key to a correct diagnosis and finding the optimal treatment. Physicians should obtain a detailed history from the patient in an open-ended fashion. Brief and comprehensive bedside neuro-otologic examinations, such as cranial nerve examinations, the Dix-Hallpike test, and the head thrust test cannot be omitted for an accurate diagnosis. Knowledge about the numerous disease entities that may contribute to dizziness can be essential for differential diagnosis. In addition, this article provides information about frequently prescribed drugs, including vestibular suppressants and antiemetics.
References
1. Nazareth I, Landau S, Yardley L, Luxon L. Patterns of presentations of dizziness in primary care-a cross-sectional cluster analysis study. J Psychosom Res 2006;60:395-401.
2. Karatas M. Central vertigo and dizziness: epidemiology, differential diagnosis, and common causes. Neurologist 2008;14:355-364.
3. Colledge NR, Wilson JA, Macintyre CC, MacLennan WJ. The prevalence and characteristics of dizziness in an elderly community. Age Ageing 1994;23:117-120.
4. Kroenke K, Lucas CA, Rosenberg ML, Scherokman B, Herbers JE Jr, Wehrle PA, Boggi JO. Causes of persistent dizziness. A prospective study of 100 patients in ambulatory care. Ann Intern Med 1992;117:898-904.
5. Dieterich MMD. Dizziness. Neurologist 2004;10:154-164.
6. Chawla N, Olshaker JS. Diagnosis and management of dizziness and vertigo. Med Clin North Am 2006;90:291-304.
7. Egger S, Zee D. In: Cummings C, Flint P, Harker L, editor. Central vestubular disorders. Otolaryngology, Head and Neck Surgery 2005;4 ed. St. Louis: Mosby. 3254-3288.
8. Farrehi PM, Santinga JT, Eagle KA. Syncope: diagnosis of cardiac and noncardiac causes. Geriatrics 1995;50:24-30.
9. Eckhardt A, Tettenborn B, Krauthauser H, Thomalske C, Hartmann O, Hoffmann SO, Hopf HC. [Vertigo and anxiety disordersresults of interdisciplinary evaluation]. Laryngorhinootologie 1996;75:517-522.
10. Chan Y. Differential diagnosis of dizziness. Curr Opin Otolaryngol Head Neck Surg 2009;17:200-203.
11. Hullar T, Zee D, Minor L. In: Flint P, Haughey B, Lund V, et al, editor. Evaluation of the Patient with Dizziness. Cummings Otolaryngology Head&Neck Surgery 2010;5 ed. Philadelphia: Mosby. 2303-2327.
12. Hüfner K, Barresi D, Glaser M, Linn J, Adrion C, Mansmann U, Brandt T, Strupp M. Vestibular paroxysmia: Diagnostic features and medical treatment. Neurology 2008;71:1006-1014.
13. Kroenke K, Mangelsdorff AD. Common symptoms in ambulatory care: incidence, evaluation, therapy, and outcome. Am J Med 1989;86:262-266.
14. Brandt T, Strupp M. General vestibular testing. Clin Neurophysiol 2005;116:406-426.
15. Baloh RW. In: Baloh RW, editor. Approach to the patient with dizziness. Dizziness, Hearing Loss, and Tinnitus 1998;Philadelphia: F.A. Davis Company.
16. Hain T, Micco A. In: Goetz C, Pappert E, editor. Neuroanatomical localization and syndromes, cranial nerve III: VESTIBULOCOCHLEAR SYSTEM. Textbook of Clinical Neurology 1999;1 ed. Philadelphia: WB saunders company. 184-199.
17. Baloh RW. Vertigo. Lancet 1998;352:1841-1846.
18. Cha CI. Korean society of otorhinolaryngology. Differential diagnosis of dizziness. Otorhinolaryngology Head and Neck Surgery 2009;2nd ed. Ilchokak. 876-897.
19. Solomon D. Distinguishing and treating causes of central vertigo. Otolaryngol Clin North Am 2000;33:579-601.
20. Seemungal BM. Neuro-otological emergencies. Curr Opin Neurol 2007;20:32-39.
21. Chae SW. Acute spontaneous vertigo. J Korean Bal Soc 2008;7:231-238.
22. Harvey SA, Wood DJ, Feroah TR. Relationship of the head impulse test and head-shake nystagmus in reference to caloric testing. Am J Otol 1997;18:207-213.
23. Chung W, Chung K. Diagnostic Approach to a Patient with Dizziness. J Korean Bal Soc 2007;6:73-79.
24. Epley JM. New dimensions of benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg 1980;88:599-605.
25. Prokopakis EP, Chimona T, Tsagournisakis M, Christodoulou P, Hirsch BE, Lachanas VA, Helidonis ES, Plaitakis A, Velegrakis GA. Benign paroxysmal positional vertigo: 10-year experience in treating 592 patients with canalith repositioning procedure. Laryngoscope 2005;115:1667-1671.
26. Bhattacharyya N, Baugh R, Orvidas L, Barrs D, Bronston L, Cass S. Clinical practice guideline: Benign paroxysmal positional vertigo. Otolaryngology-Head and Neck Surgery 2008;139:S47-S81.
27. Bergenius J, Perols O. Vestibular neuritis: a follow-up study. Acta Otolaryngol 1999;119:895-899.
28. Minor LB, Schessel DA, Carey JP. Meniere's disease. Curr Opin Neurol 2004;17:9-16.
29. Crane BT, Schessel DA, Nedzelski J, Minor LB. In: Flint P, Haughey B, Lund V, editor. Peripheral vesibular disorders. Cummings Otolaryngology Head&Neck Surgery 2010;Philadelphia: Mosby. 2328-2345.
30. Lempert T, Neuhauser H. Migrainous vertigo. Neurol Clin 2005;23:715-730. vi.
31. Neuhauser HK, Lempert T. Diagnostic criteria for migrainous vertigo. Acta Otolaryngol 2005;125:1247-1248.
32. Furman JM, Marcus DA, Balaban CD. Migrainous vertigo: development of a pathogenetic model and structured diagnostic interview. Curr Opin Neurol 2003;16:5-13.
33. Lee H, Cho YW. A case of isolated nodulus infarction presenting as a vestibular neuritis. J Neurol Sci 2004;221:117-119.
34. Lee H, Sohn SI, Jung DK, Cho YW, Lim JG, Yi SD, Lee SR, Sohn CH, Baloh RW. Sudden deafness and anterior inferior cerebellar artery infarction. Stroke 2002;33:2807-2812.
35. Baloh RW. Clinical practice. Vestibular neuritis. N Engl J Med 2003;348:1027-1032.
36. Tighilet B, Leonard J, Lacour M. Betahistine dihydrochloride treatment facilitates vestibular compensation in the cat. J Vestib Res 1995;5:53-66.
37. Shinkawa H, Kimura RS. Effect of diuretics on endolymphatic hydrops. Acta Otolaryngol 1986;101:43-52.
Figure 1
Physiology of the head thrust test. Head movement towards a canal will cause activation of that canal. Reflex movement of the eyes in the opposite direction- that is, away from the canal (A). Head movement towards a defunct canal will result in the failure of activation of the vestibulo-ocular reflex and thus the visual target will be lost from fixation during sudden head movements (B).
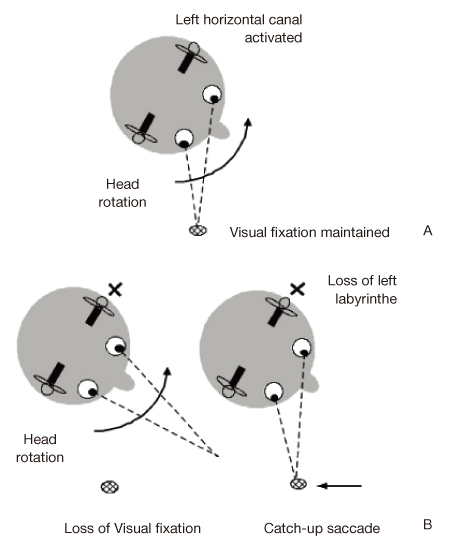
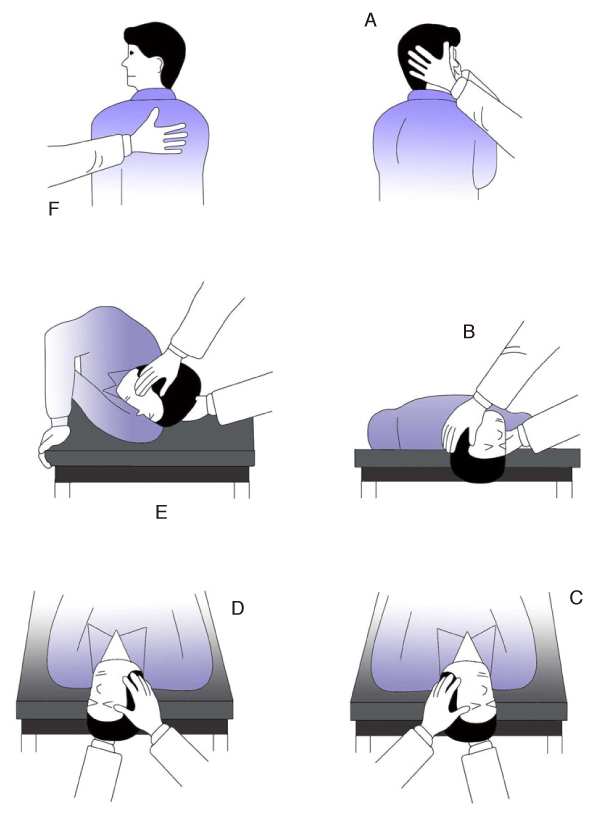
Figure 2
Sit the patient upright. Turn the patient's head to the affected side at a 45 degree angle (A). The patient is brought into the supine position with the head extended below the level of the bed (Dix-Hallpike position) (B). Maintain up to 30 seconds after nystagmus disappears (C). Turn the patient's head 90 degrees to the other side (D). The patient's head is further rotated to the opposite side by rolling until the patient is face down (E). The patient is brought back to the upright position (F).
- TOOLS
-
- Share :
-





-
METRICS

-
Related articles in
J Korean Med Assoc -
Prevalence and treatment status of diabetes mellitus in Korea2023 July;66(7)
Diagnosis and treatment of women with recurrent urinary tract infection2022 September;65(9)
Pharmacological treatment of the patients with croup2021 July;64(7)
Prevalence and treatment of pediatric dyslipidemia2021 June;64(6)
Diagnosis and treatment of patients with heat-related illnesses2021 April;64(4)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
