







 |
 |
| J Korean Med Assoc > Volume 53(8); 2010 > Article |
Abstract
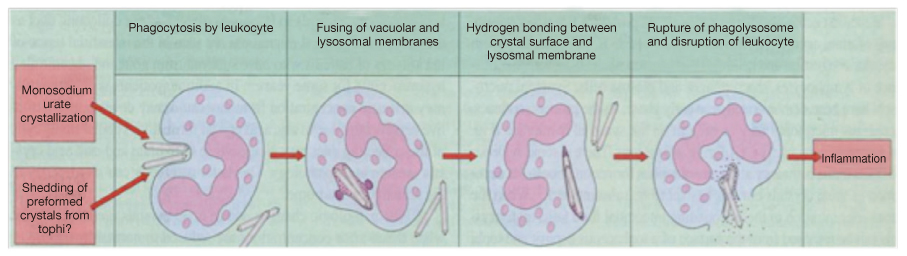
Gout is a medical condition usually characterized by recurrent attacks of acute inflammatory arthritis involving, most commonly, the big toe, ankle, or other joints of the foot resulting from responses to the deposition of urate crystals from extracellular fluids supersaturated with urate. Middle aged men who are obese and drink alcohol regularly are the most susceptible. It is considered a chronic and progressive disease. Chronic gout can also lead to deposits of hard lumps of uric acid in the tissues, particularly in and around the joints, and may cause joint destruction, decreased kidney function, and kidney stones. It is associated with metabolic syndrome including dyslipidemia, hypertension, hyperglycemia, and obesity. Gout is suspected when a patient reports a history of attacks of painful arthritis, particularly at the base of the toes. A confirmative diagnosis of gout requires demonstration of monosodium urate crystals in the synovial fluid, tophi, or tissues.
References
1. Choi HK, Mount DB, Reginato AM. Pathogenesis of gout. Ann Intern Med 2005;143:499-516.
2. Roubenoff R, Klag MJ, Mead LA, Liang KY, Seidler AJ, Hochberg MC. Incidence and risk factors for gout in white men. JAMA 1991;266:3004-3007.
3. Campion EW, Glynn RJ, DeLabry LO. Asymptomatic hyperuricemia. Risks and consequences in the Normative Aging Study. Am J Med 1987;82:421-426.
4. Cronstein BN, Molad Y, Reibman J, Balakhane E, Levin RI, Weiss-mann G. Colchicine alters the quantitative and qualitative display of selectins on endothelial cells and neutrophils. J Clin Invest 1995;96:994-1002.
5. Getting SJ, Flower RJ, Parente L, de Medicis R, Lussier A, Woliztky BA, et al. Molecular determinants of monosodium urate crystal-induced murine peritonitis: a role for endogenous mast cells and a distinct requirement for endothelial-derived selectins. J Pharmacol Exp Ther 1997;283:123-130.
6. Choi HK, Atkinson K, Karlson EW, Willett W, Curhan G. Purine-rich foods, dairy and protein intake, and the risk of gout in men. N Engl J Med 2004;350:1093-1103.
7. Choi HK, Atkinson K, Karlson EW, Willett W, Curhan G. Alcohol intake and risk of incident gout in men: a prospective study. Lancet 2004;363:1277-1281.
8. Grahame R, Scott JT. Clinical survey of 354 patients with gout. Ann Rheum Dis 1970;29:461-468.
9. Becker MA, Jolly M. In: Koopman WJ, Moreland LW, editor. Clinical gout and the pathogenesis of hyperuricemia. Arthritis and allied conditions 2005;15th ed. Philadelphia: Lippincott Williams & Wilkins. 2303-2339.
10. Lally EV, Ho G Jr, Kaplan SR. The clinical spectrum of gouty arthritis in women. Arch Intern Med 1986;146:2221-2225.
11. Nakayama DA, Barthelemy C, Carrera G, Lightfoot RW Jr, Wortmann RL. Tophaceous gout: a clinical and radiographic assessment. Arthritis Rheum 1984;27:468-471.
12. Brown J, Mallory GK. Renal changes in gout. N Engl J Med 1950;243:325-329.
13. Talbott JH, Terplan KL. The kidney in gout. Medicine (Baltimore) 1960;39:405-467.
14. Rho YH, Choi SJ, Lee YH, Ji JD, Choi KM, Baik SH, Chung SH, Kim CG, Choe JY, Lee SW, Chung WT, Song GG. The prevalence of metabolic syndrome in patients with gout: a multicenter study. J Korean Med Sci 2005;20:1029-1033.
15. Emmerson B. Hyperlipidaemia in hyperuricaemia and gout. Ann Rheum Dis 1998;57:509-510.
16. Rathmann W, Funkhouser E, Dyer AR, Roseman JM. Relations of hyperuricemia with the various components of the insulin resistance syndrome in young black and white adults: the CARDIA study. Coronary Artery Risk Development in Young Adults. Ann Epidemiol 1998;8:250-261.
17. Lee J, Sparrow D, Vokonas PS, Landsberg L, Weiss ST. Uric acid and coronary heart disease risk: evidence for a role of uric acid in the obesity-insulin resistance syndrome. The Normative Aging Study. Am J Epidemiol 1995;142:288-294.
18. Choi HK, Atkinson K, Karlson EW, Curhan G. Obesity, weight change, hypertension, diuretic use, and risk of gout in men: the Health Professionals Follow-up Study. Arch Intern Med 2005;165:742-748.
19. Dieppe P, Swan A. Identification of crystals in synovial fluid. Ann Rheum Dis 1999;58:261-263.
20. Wallace SL, Robinson H, Masi AT, Decker JL, McCarty DJ, Yü TF. Preliminary criteria for the classification of the acute arthritis of primary gout. Arthritis Rheum 1977;20:895-900.
21. Choi HK, Al-Arfaj AM, Eftekhari A, Munk PL, Shojania K, Reid G, Nicolaou S. Dual energy computed tomography in tophaceous gout. Ann Rheum Dis 2009;68:1609-1612.
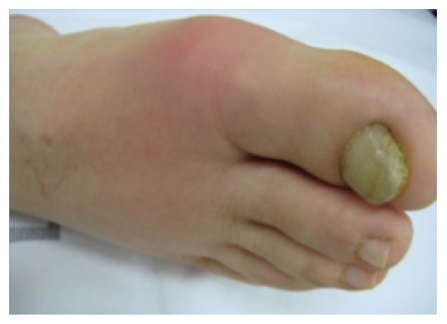
Figure 3
Acute gout attack presenting in the 1st metatarsophalangeal joint. Redness, swelling and severe tenderness on the affected joint are distinctive features.
- TOOLS
-
- Share :
-





-
METRICS

-
Related articles in
J Korean Med Assoc -
Clinical features and treatment of rosacea2024 May;67(5)
Classification and endoscopic diagnosis of colorectal polyps2023 November;66(11)
Clinical guidelines for diagnosis of hematuria2023 June;66(6)
Clinical presentation, diagnosis, and treatment of sleep disorders in adolescents2023 April;66(4)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
