Allogeneic Hematopoietic Cell Transplantation: Early Development
Allogeneic hematopoietic cell transplantation (HCT) is a well-established curative treatment modality for a significant proportion of patients with hematologic malignancies and bone marrow failure syndrome. The initial development of allogeneic HCT was conceptually based on the experiments using murine model, where the lethally irradiated animals were salvaged by the infusion of spleen/bone marrow cells from the other animals(1, 2), a seminal observation made in the early 1950's. Early attempts to treat patients with terminal leukemia with total body irradiation (TBI) and subsequent infusion of bone marrow cells from healthy subjects, however, were largely unsuccessful(3, 4). Systematic studies in canine transplantation models showed that the matching for the dog leukocyte antigens (DLA) between littermates was an important determinant for successful HCT(5, 6). Therefore, subsequent development of clinical allogeneic HCT techniques centered around the two premises that were assumed to be important; the first is the conditioning of patients before HCT with radiation and/or chemotherapy regimens that can ablate the bone marrow of the patients (especially for patients with leukemia). The other is that the donor and recipient should carry identical human leukocyte antigens (HLA)(7~10).
These premises, however, impeded the wider application of allogeneic HCT. Patients should be relatively young and fit to tolerate rigorous intensity of conditioning regimens. Moreover, less than one-third of patients who require allogeneic HCT have an HLAmatched family member who can donate hematopoietic cells(11).
Hematopoietic Cell Transplantation from an HLA-mismatched Family Donor: Initial and Subsequent Clinical Studies
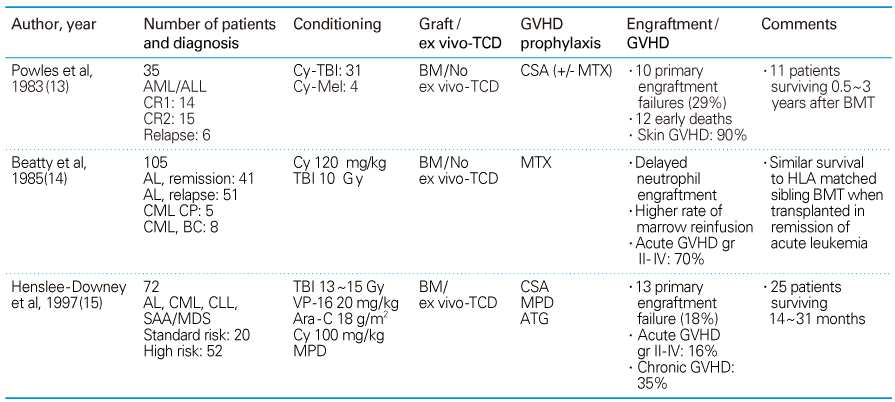
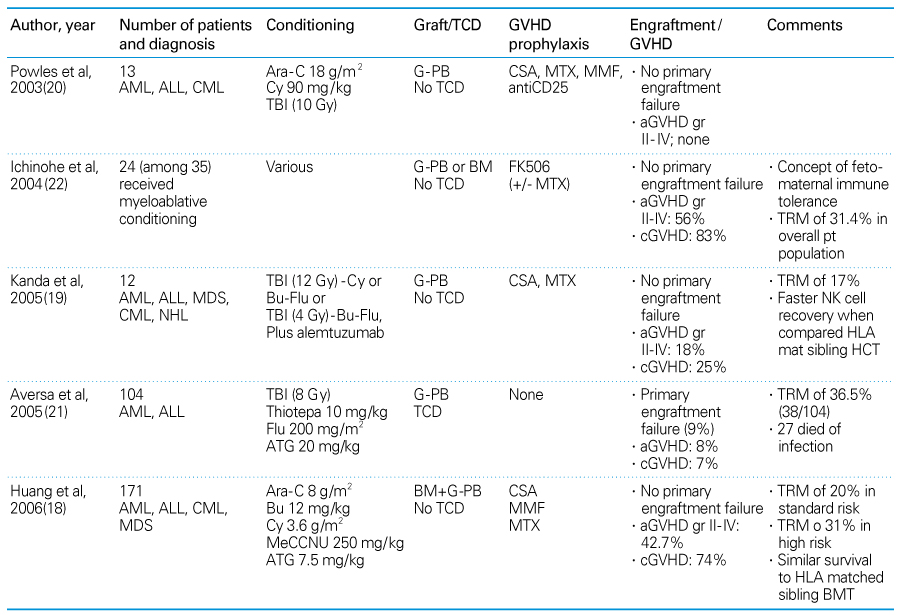
Nearly all patients who are in need of allogeneic HCT have at least one HLA-haploidentical family member who is willing to donate hematopoietic cells immediately, not only for the initial transplantation, but also for any additional donations that may become necessary(12). Early studies attempting to transplant allogeneic hematopoietic cells across the HLA-haplotype barrier used myeloablative conditioning regimens that were similar to those used in HLA-matched sibling HCT (Table 1)(13, 14). These trial showed high frequencies of engraftment failure, delayed neutrophil engraftment, and, when engraftment occurred, excessive graft-versus-host disease (GVHD). Even in these early observations, however, there were small portions of patients who experienced successful donor cell engraftment without serious GVHD, and achieved long-term remission of their leukemia. These findings suggested that the HLA- haplotype difference was not an absolute but a relative barrier to successful HCT. Increasing the intensity of conditioning(15) and/or depletion of donor T cells from the grafts prior to HCT (15, 16) decreased the frequency and severity of GVHD, but it also resulted in the increased graft failure, delayed immune reconstitution, and increased fatal infections, thus failing to improve overall outcomes of HLA-mismatched HCT. In subsequent clinical studies, several groups of investigators tried to improve outcomes of HLA-mismatched HCT; these efforts included the use of polyclonal(17, 18) or monoclonal(19, 20) antibodies against T cells as a part of the conditioning regimen (in vivo-T cell depletion), transplantation of higher dose of purified CD34+ cells(21), and incorporation of the concept of fetomaternal immune tolerance in selecting donors from among several available HLA-mismatched family members(Table 2)(22). Overall, these trial showed improved outcomes after HLA-mismatched HCT when compared to earlier trials. However, allogeneic HCT from an HLA-mismatched family member remained a procedure that was associated with high regimen-related toxicities and high transplantation-related mortality (TRM) ranging from 20% to 40%(17, 21, 22).
Advent of Reduced-intensity Conditioning in Allogeneic Hematopoietic Cell Transplantation
In a canine HCT model, Storb et al pioneered a concept of donor hematopoietic cell engraftment in a host after a conditioning regimen that was suppressive of immunity rather than ablative of bone marrow of the host(23). In this model, leukemia cure is dependent more upon graft-versus-leukemia effect than upon high-doses of chemo- or radiotherapy given as a part of conditioning. Various non-myeloablative, immunosuppressive conditioning regimens [collectively called reduced-intensity conditioning (RIC)] have been introduced rapidly into clinical allogeneic HCT from both HLA-matched siblings and unrelated donors. These RIC contained TBI in reduced-dose (24), busulfan in reduced-dose(25, 26), or melphalan(27), along with fludarabine. RIC for allogeneic HCT have shown to be effective in achieving successful engraftment with a reduced frequency of TRM, particularly in elderly patients and in patients with organ dysfunctions. With an advent of RIC, it became possible to perform allogeneic HCT in patients up to 70 years of age. Successful introduction of RIC in clinical HCT demonstrated that, under conditions of adequate immunosuppression of the patients but not necessarily myeloablation, donor hematopoietic cells can engraft and a complete donor hematopoietic chimerism can be achieved.
Allogeneic Hematopoietic Cell Transplantation Across MHC-barrier after Reduced-intensity Conditioning: Animal Studies
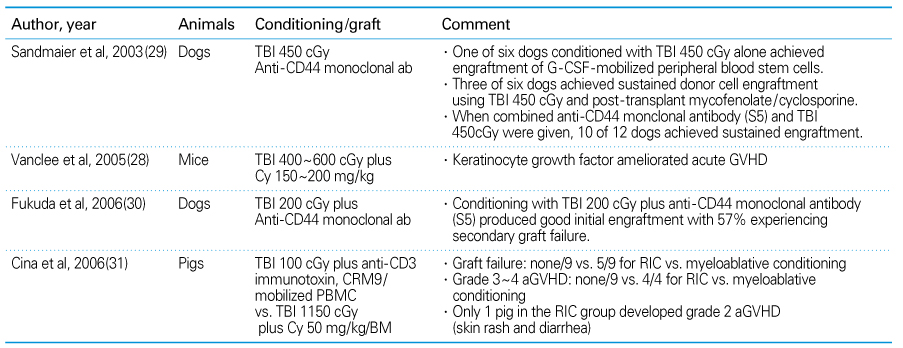
The principle shown in the success of RIC in HLA-matched allogeneic HCT, i.e. the importance of immune-suppression, but not myeloablation, for the donor cell engraftment, might be extended to HLA-mismatched HCT settings. Successful engraftment of allogeneic hematopoietic cells across major histocompatibility complex (MHC) gene-haplotype difference after RIC has been well-documented in murine(28) as well as in large animal HCT models(Table 3)(29~31). In a DLA-haploidentical littermate HCT setting(29), one of 6 dogs conditioned with TBI 450 cGy alone achieved engraftment of granulocyte colony-stimulating factor (G-CSF) mobilized peripheral blood stem cells. When posttransplant immunosuppression with mycofenolate plus cyclo-sporine was added, 3 of 6 dogs achieved sustained donor cell engraftment. When murine anti-CD44 monoclonal antibody, S5, was added to conditioning regimen of TBI, along with posttransplant immuno-suppression, 10 of 12 dogs achieved sustained engraftment. These findings suggested that DLA-haplotype barrier can be overcome after RIC. Furthermore, the addition of anti-CD44 monoclonal antibody to conditioning regimen enhanced engra-ftment potential significantly. A subsequent canine HCT study(30) showed that reducing TBI dose to 200 cGy in the conditioning along with anti-CD44 monoclonal antibody produced good initial engraftment; however over the half of the dogs experienced secondary graft failure subsequently. In a swine leukocyte antigen (SLA)-haploidentical trans-plantation study(31), results from RIC (TBI 100 cGy plus anti-CD3 immunotoxin, CRM9) with mobilized peripheral blood mononuclear cell grafting was compared to those of myeloablative conditioning (TBI 1150 cGy plus cyclophosphamide 50 mg/kg) with bone marrow cell grafting. While all of 9 animals in the RIC group achieved sustained donor cell engraft-ment, 5 of 9 animals in the myeloablative conditioning group failed to engraft. Furthermore, while only 1 animal in the RIC group developed grade 2 acute GVHD (skin rash and diarrhea), all 4 engrafted animals in the myeloablative conditioning group developed grade 3 to 4 acute GVHD. These findings suggested that RIC with TBI 100 cGy plus anti-T cell antibody in the SLA-haploidentical setting was immunosuppressive enough to facilitate efficient donor cell engraftment. In addition, acute GVHD may be decreased in the RIC group probably due to less host tissue damage and less release of proinflam-matory cytokines during conditioning and donor cell infusion.
HLA-mismatched Allogeneic Hematopoietic Cell Transplantation after Reduced-intensity Conditioning: Clinical Settings
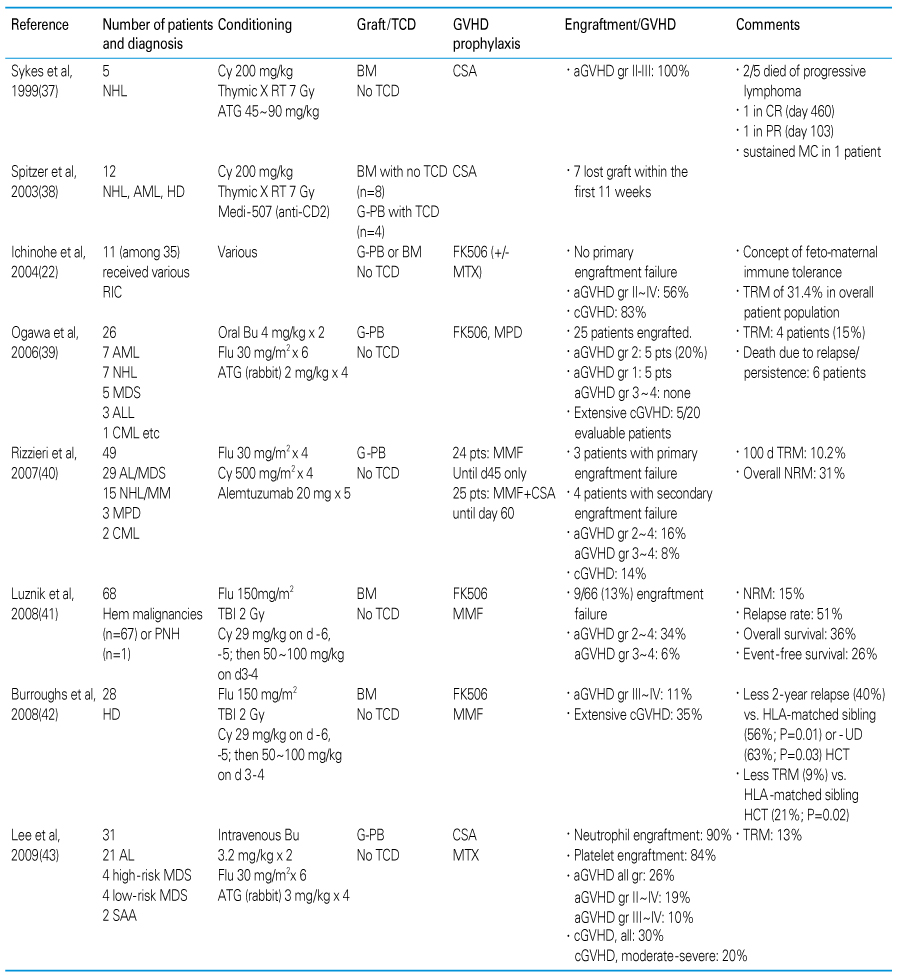
The feasibility of successful donor cell engraftment across HLA-haplotype difference after RIC in a clinical setting was first suggested in children with severe combined immunodeficiency, who were transplanted with hematopoietic cells from HLA-mismatched familial donors after RIC or even without conditioning(32~34). In these studies, durable donor cell engraftment with a full T-and B-cell function recovery after HCT was documented. As per adult patients with hematologic malignancies or bone marrow failure syndrome, other than single case reports(35, 36), there are now six hospitals worldwide which have published results of HLA-mismatched HCT after RIC(Table 4).
Massachusetts General Hospital Study
The first clinical study investigating the role of RIC in HLA-mismatched HCT in adult patients with hematologic malignancy was published by Syke et al(37). The conditioning regimen was based on murine HCT data and included cyclophosphamide (200 mg/kg), irradiation to the thymus (700 cGy), and anti-thymocyte globulin (ATG). All 5 patients in the study had advanced non-Hodgkin's lymphoma and all had grade 2~3 acute GVHD after HCT. Two patients were surviving in complete and partial remission of their lymphoma for 460 and 103 days, respectively, in full donor lymphocyte chimerism (>90%). In a subsequent study(38), anti-CD2 monoclonal antibody, Medi-507, replaced ATG. Mixed donor chimerism was achieved in most of 12 patients studied.
Kyoto University study
Ichinohe, et al(22) selected their potential hematopoietic cell donors among several HLA-mismatched family members based on the concept of fetomaternal immune tolerance (microchimerism occurring during pregnancy with subsequent immunologic tolerance between mother and offspring). Accordingly, mothers, not fathers, were preferred donors for offspring patients. Among HLA-haploidentical siblings, ones with mismatched haplotype not shared by mother were chosen as cell donors. Of 35 patients reported, 12 patients received various RIC regimens and 11 achieved successful donor cell engraftment.
Osaka University study
Ogawa, et al(39) used RIC of oral busulfan (8 mg/kg), fludarabine (180 mg/m2), and rabbit-ATG (8 mg/kg; Fresnius, Munich, Germany), a similar conditioning regimen originally used by Slavin, et al(25) for HLA-mismatched HCT in 26 patients with various hematologic malignancies. Hematopoietic cells were harvested from the donor peripheral blood after mobilization with G-CSF. Post-transplant immunosuppression for GVHD prophylaxis included FK506 and methylprednisolone. Twenty-five patients achieved primary donor cell engraftment. Five patients (20%) experienced grade 2 acute GVHD. None experienced acute GVHD over grade 2. Extensive chronic GVHD occurred only in 5 of 20 evaluated patients. Four patients died without recurrence/persistence of underlying malignancy giving TRM of 15%. Fifteen patients survived in CR with 3-year event free survival rate of 55%. Donor chimerism was achieved rapidly with all of 25 patients with primary engraftment showing 95% to 100% donor chimerism by 2 weeks after transplantation. CD8+ cells recovered rapidly after HCT with a median count of about 1,000/µl at 9 months although CD4+ cells recovered more slowly (median 100/µl at 9 months).
Duke University study
Rizzieri, et al(40) used RIC of cyclophosphamide (2 g/m2), fludarabine (120 mg/m2), and a humanized anti-CD52 monoclonal antibody (Alemtuzumab) 100 mg in 49 patients undergoing HCT from HLA-mismatched family donors who donated G-CSF mobilized peripheral blood mononuclear cells. Three and 4 patients experienced primary and secondary graft failure, respectively. Grade 2~4 acute GVHD was not frequent and observed in 16% of patients. Chronic GVHD occurred only in 14% of patients. Overall, 31% of patients experienced TRM, mostly due to infections.
Johns Hopkins University/Fred Hutchinson Cancer Center studies
Luznik, et al(41) used RIC of TBI 200 cGy, fludarabine 150 mg/m2, and cyclophos-phamide 29 mg/kg in 68 patients undergoing HLA-mismatched HCT. Bone marrow cell grafts were used without ex vivo -T cell depletion. On days 3 to 4 of HCT, cyclophosphamide 50~100 mg/kg was given additionally. Post-transplant immunosuppression included FK506 and mycophenolate. Graft failure occurred in 9 patients (13%). Grade 2~4 acute GVHD occurred in 34%. Oneyear TRM and relapse rates were 15% and 51%, respectively. Burroughs, et al(42) applied similar RIC in 90 patients with advanced Hodgkin's disease. Of those, 38 patients were transplanted with cells from HLA-matched related donors; 24 from HLA-matched unrelated donors; and 28 from HLA-haploidentical related donors. The frequencies of acute GVHD grade 3~ 4 and extensive chronic GVHD were 16%/50% (HLA-matched related), 8%/63% (unrelated), and 11%/35% (HLA-haploidentical related). Interestingly, patients who underwent HLA-haploidentical HCT experienced significantly less disease recurrence/progression when compared to HLA-matched HCT from related or unrelated donors [2-year rates; 40% vs. 56% (P=0.01) vs. 63% (P=0.03)]. TRM was also significantly lower for HLA-haploidentical HCT when compared to HLA-matched related HCT (9% vs. 21% at 2 years; P=0.02).
University of Ulsan, Asan Medical Center study
In our hospital, an allogeneic HCT protocol for patients with high-risk hematologic disorders, utilizing an HLAmismatched family member as the donor, was initiated in April 2004(43). Thirty-one patients (median age, 34 years; range, 16~69 years) were enrolled before April 2008. The cell donors were either mother (n=14), offspring (n=9), or siblings (n=8) of these patients. The conditioning regimen consisted of busulfan 6.4 mg/kg/day intravenously, fludarabine 180 mg/m2, and rabbit-ATG (12 mg/kg; Genzyme Transplant) or horse-ATG (45 mg/kg), a variation of original RIC of Slavin, et al(25). Hematopoietic cells were collected from the donors via leukapheresis after G-CSF mobilization and infused without further manipulation. Cyclosporine and methotrexate were administered for GVHD prophylaxis. Excluding 3 patients who died or relapsed with leukemia within 3 weeks after HCT, all remaining 28 patients engrafted with neutrophil (>500/µl) at a median of 16.5 days. Over 90% of evaluated patients (22/24) achieved donor chimerism 95% or over at 2 weeks after HCT and none experienced secondary graft failure. Acute GVHD grade 2~4 and moderate-severe chronic GVHD were observed in 19% and 20%, respectively. Four patients died due to transplantation related causes (3 sepsis; 1 acute GVHD) giving TRM of 13%. The patients showed a prompt recovery of their lymphocyte subset counts with mean CD4+ and CD8+ cell counts over 250/µland 1,000/µl, respectively from 2 months after HCT.
The consistent engraftment with low frequencies of acute and chronic GVHD observed following HLA-mismatched HCT after RIC, as demonstrated in the aforementioned studies, is intriguing and in contrast to the traditional concept of allogeneic HCT, where an increasing number of HLA disparities is considered as one of the most important determinants for increasing graft failure, as well for increasing GVHD(11). Decreased tissue damage induced by RIC, as opposed to myeloablative conditioning, may lead to reduced release of tissue antigens and proinflammatory cytokines, thereby favoring a post-transplant host environment with less triggering of acute GVHD. In addition, changes in the conditioning regimen given prior to allogeneic HCT can increase the contents and functions of regulatory T cells, resulting in an immune-modulatory rather than an immune-stimulating environment after HCT(44). Taken together, these findings suggest that the role of disparities in major MHC antigens as a determinant of adverse outcomes of HCT may vary according to the intensity and type of conditioning regimens.
HLA-mismatched Hematopoietic Cell Transplantation: The Future
The fact that it is now possible to perform allogeneic HCT from an HLA-mismatched family member using RIC without excessive morbidity and mortality to the patients is likely to change the way we apply allogeneic HCT in clinic in a major way. Allogeneic HCT now can be used in patients with high-risk hematologic malignancies and bone marrow failure syndrome, even when an HLA-matched donor is not available or when allogeneic HCT is needed urgently (therefore there is no time for unrelated donor search and coordination for cell collection). Moreover, due to the less intense nature of conditioning regimen, elderly patients (up to 70 years of age) and patients who have been treated a great deal, particularly with a previous HCT, can also be treated.
Stronger graft-versus-leukemia effect after HLAmismatched HCT compared to HLA-matched HCT was shown in a murine model; (45) the same effect was also suggested in a clinical trial(42). Therefore, further prospective clinical studies are needed to determine whether a stronger graft-versus-leukemia effect would result from HLA-mismatched HCT compared with HLA-matched HCT. Finally, HLA-mismatched HCT may provide a clinical setting where donor natural killer cell infusion therapy may be utilized for effective immunotherapy for advanced malignancies (46) (and unpublished data, Lee K-H and Choi I).