Differential Diagnosis and Management of Abnormal Posture of the Head and Neck
Article information
Abstract
Abstract
Abnormal posture of the head and neck can happen to anybody from neonates to adults, which requires appropriate interventions according to etiologies. Congenital muscular torticollis is the most common cause of abnormal posture of the head and neck in infancy, where early intervention as soon as possible is critical for better therapeutic outcome. Childhood laterocollis is heterogeneous condition, which needs etiological diagnosis for the proper management. Cervical dystonia is the most common form of focal dystonia and an overview on clinical presentations and therapeutic options including chemodenervation with botulinum toxin injection was provided. Abnormal posture of the head and neck of acute onset could be a sign of serious conditions and needs differential diagnosis.

Abnormal posture of the head and neck. (A) Left torticollis, (B) Right laterocollis, (C) Anterocollis, (D) Retrocollis.
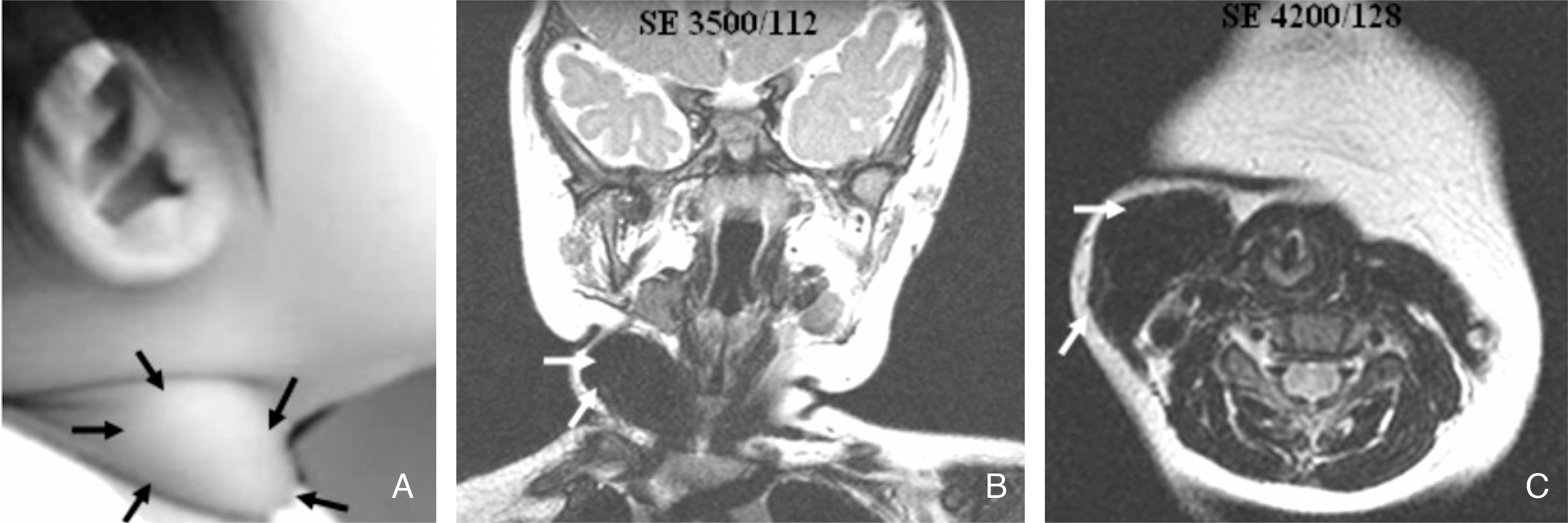
A 10 month-old girl who has right congenital muscular torticollis. (A) Unilateral palpable neck mass of muscle-consistency on right sternocleidomastoid muscle. (B) and (C) Neck MRI findings showing large mass of right sternocleidomastoid muscle.
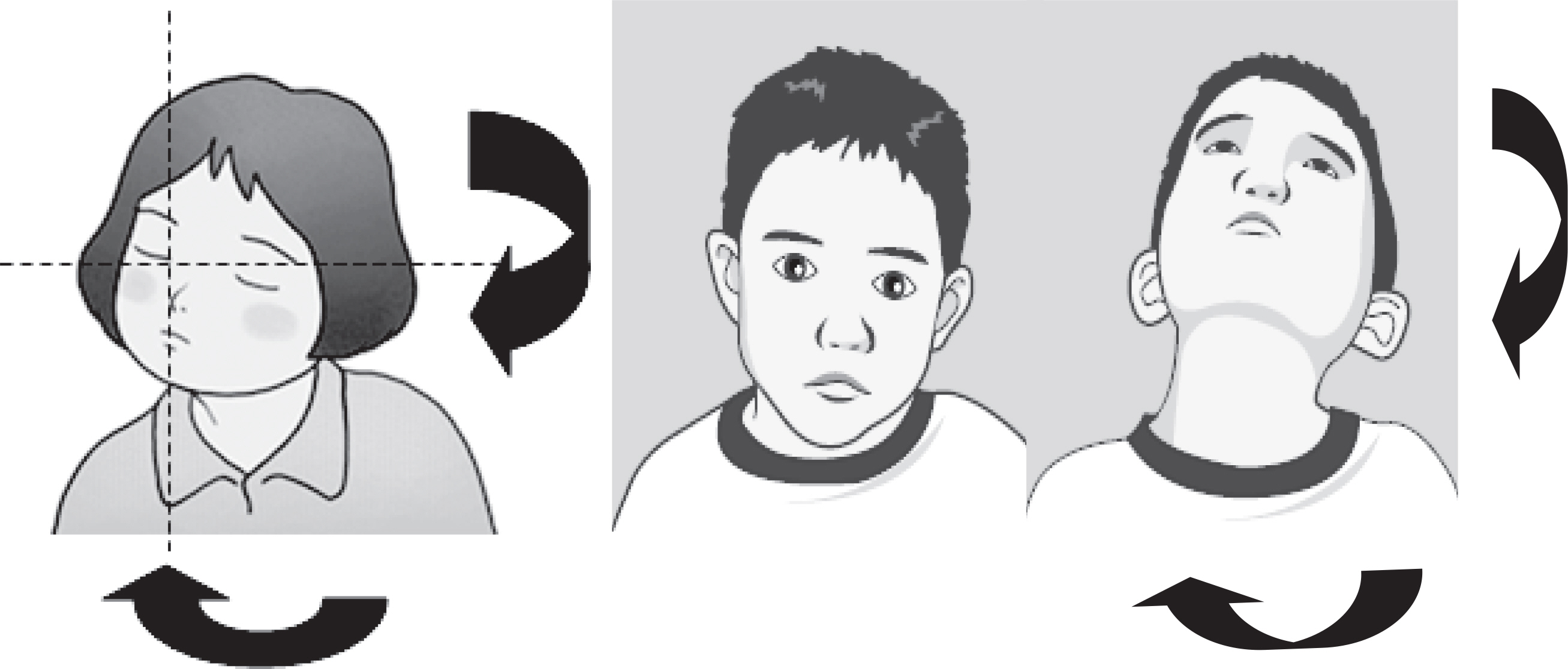
Children who have left congenital muscular torticollis which have thick and short left sternocleidomastoid muscle, ending up with right torticollis and left laterocollis.

(A) Relations between the sternocleidomastoid muscle (SCM) and the internal branch of the superior laryngeal nerve (ibSLN). (B) Relations between the ibSLN and the other anatomic structures. ECA external carotid artery, SLA superior laryngeal artery Adapted from Kiray A, Naderi S, Ergur?, Korman E. Surgical anatomy of the internal branch of the superior laryngeal nerve. Eur Spine J 2006; 15: 1320–1325 with kind permission of Springer Science + Business Media.
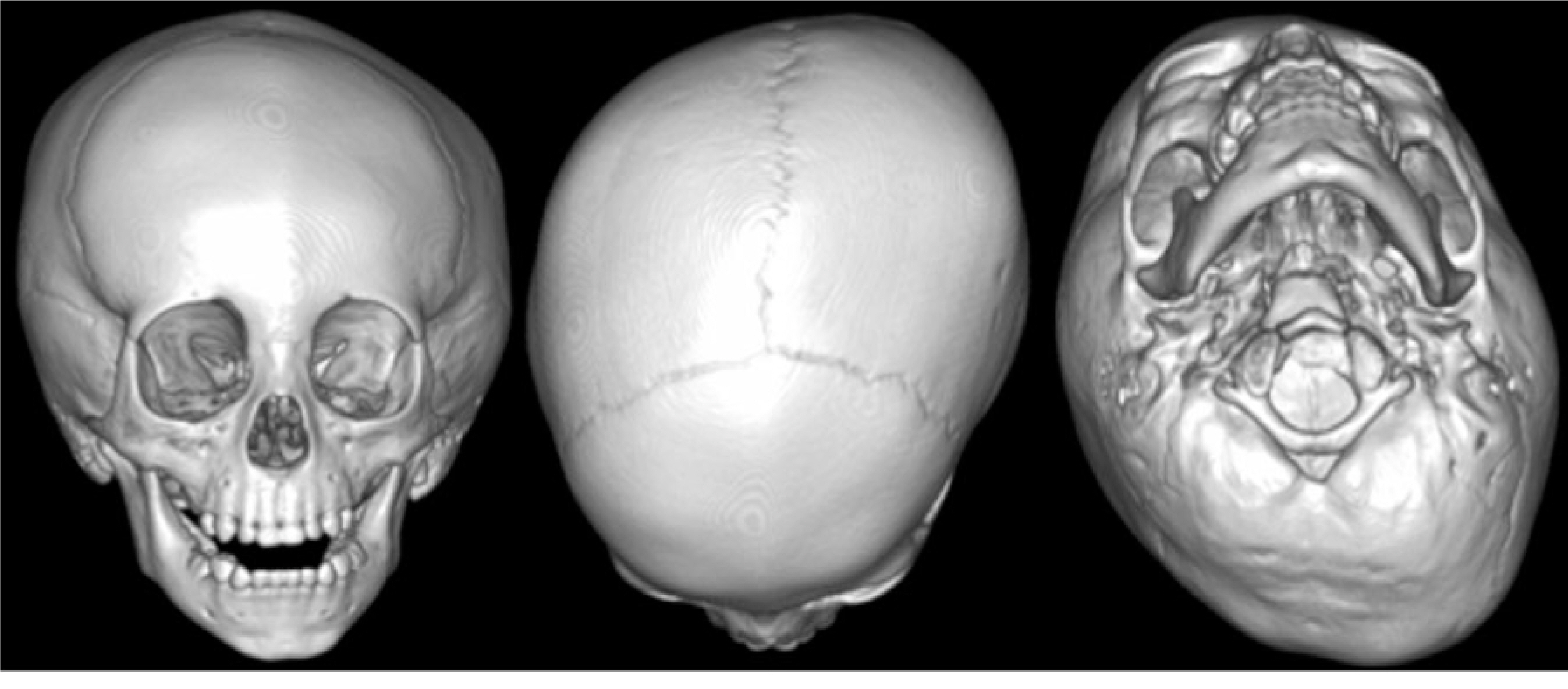
Three-dimensional CT showing left plagiocephaly associated with left congenital muscular torticollis.
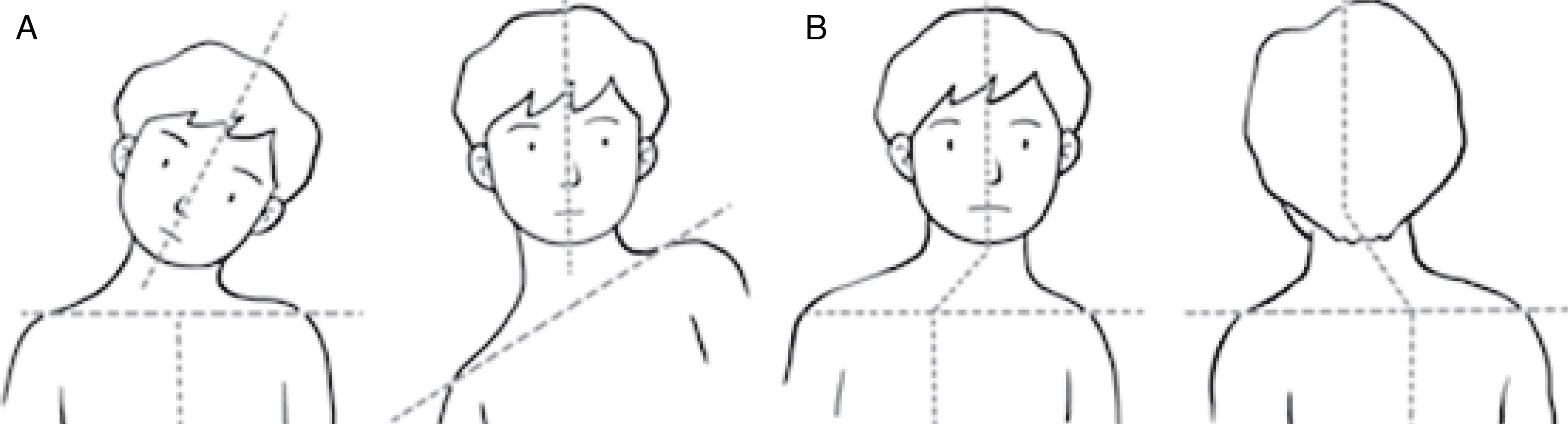
A diagram showing spontaneous compensation for torticollis by (A) elevation of the shoulder on the affected side or by (B) production of cervical scoliosis with two curves.
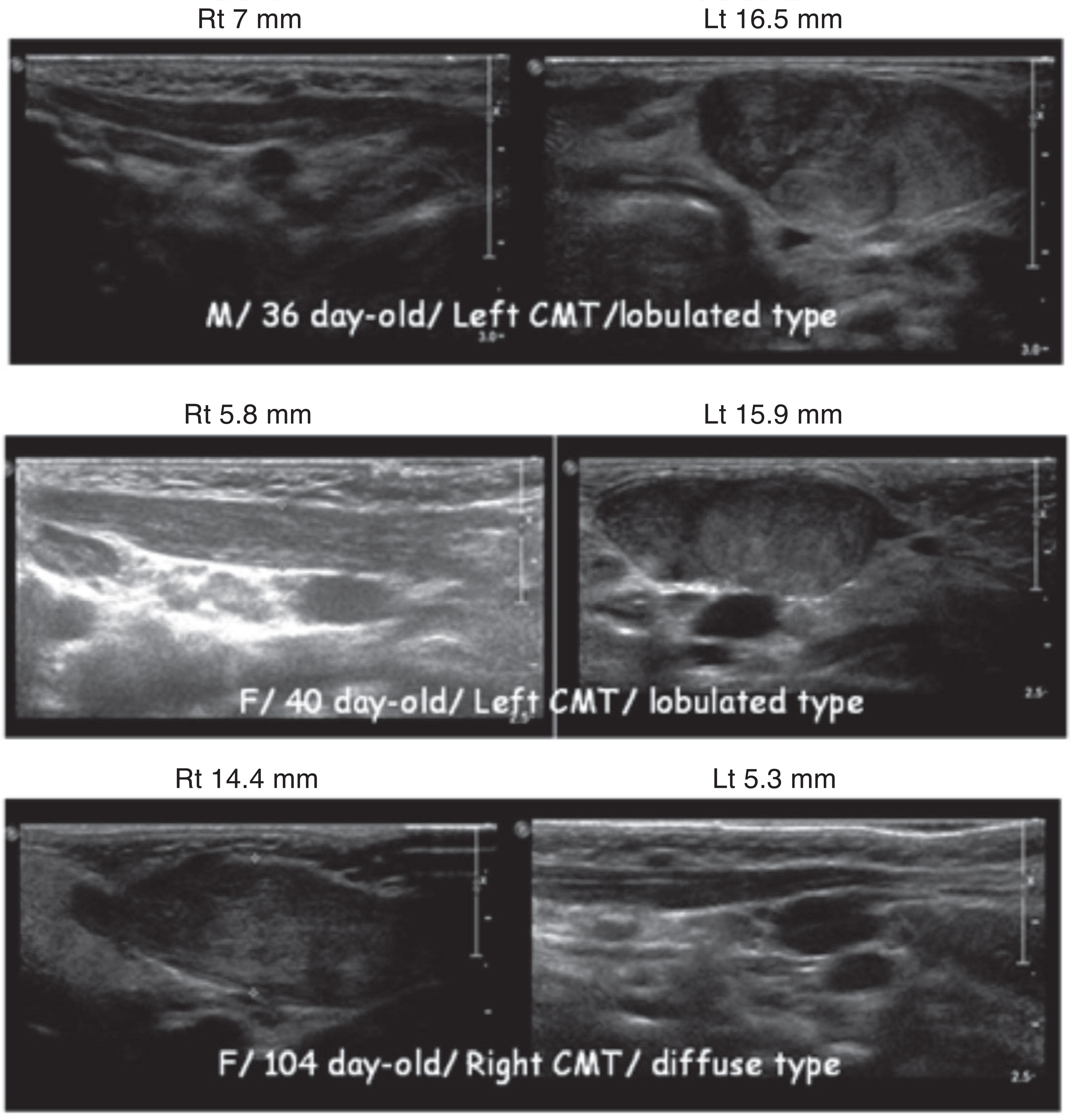
The ultrasonographic findings of the sternocleidomastoid muscle for the children who had congenital muscular torticollis (CMT).

Histologic findings of the sternocleidomastoid muscle with congenital muscular torticollis. (A) Diffuse fibroblastic proliferation with fibrosis and accompanying atrophic muscle fibers. H&E;x100. (B) Irregular arrangement of fibrous trabeculae, mature adipose cells and muscle fibers. H&E;x100.
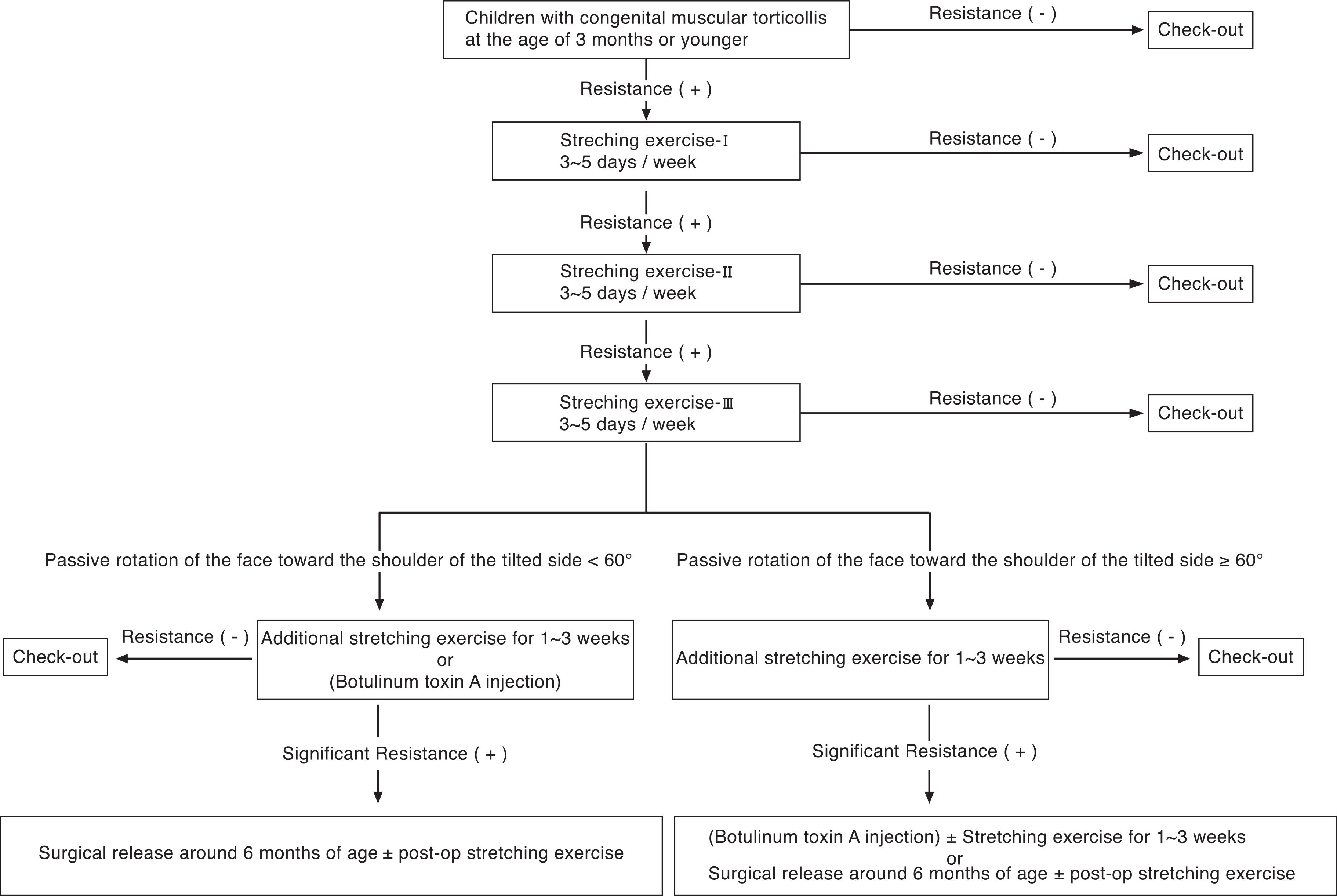
Ajou therapeutic protocol for children with congenital muscular torticollis at the age of 3 months or younger.
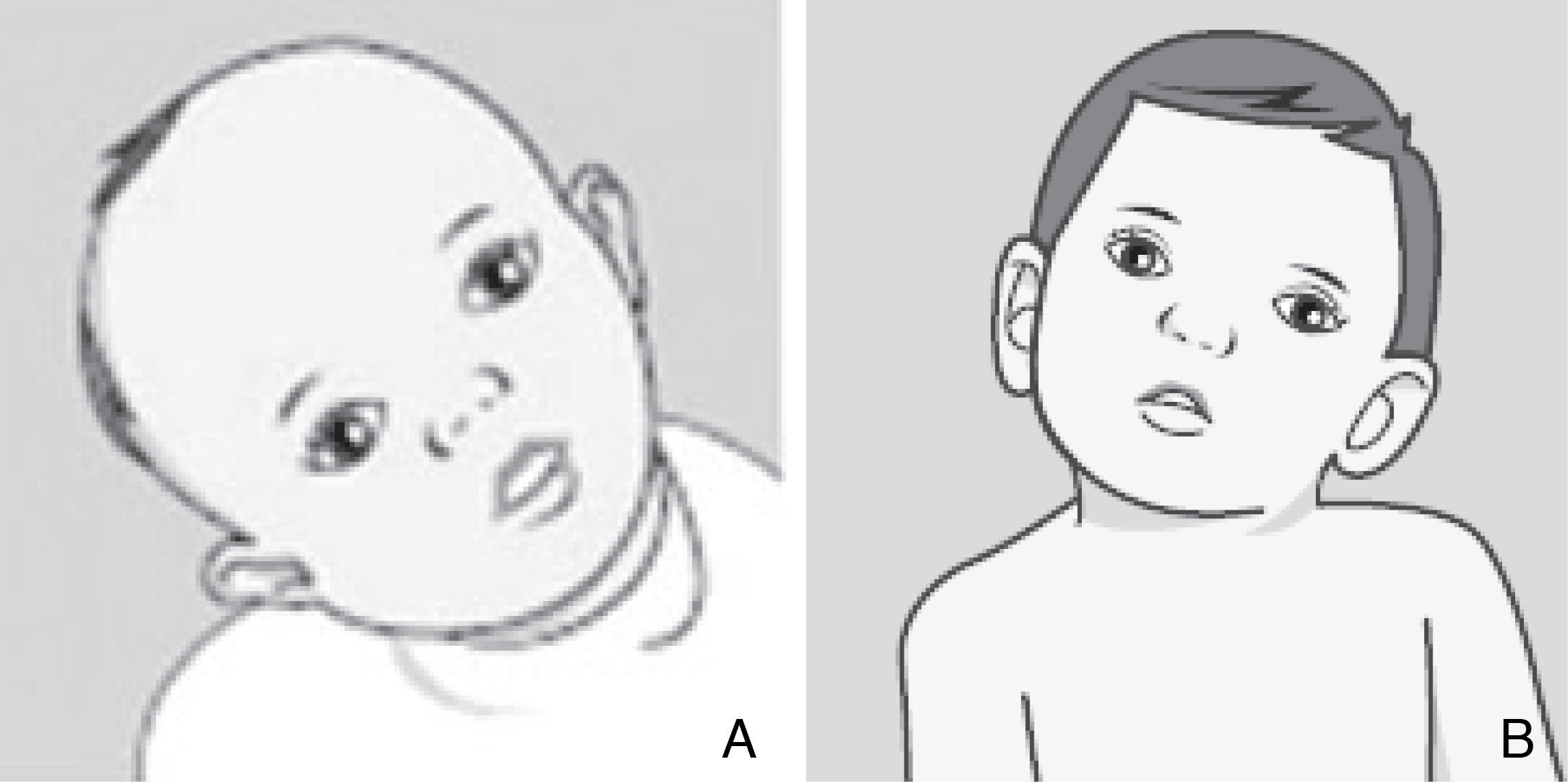
The boys who show (A) right laterocollis and (B) left laterocollis.
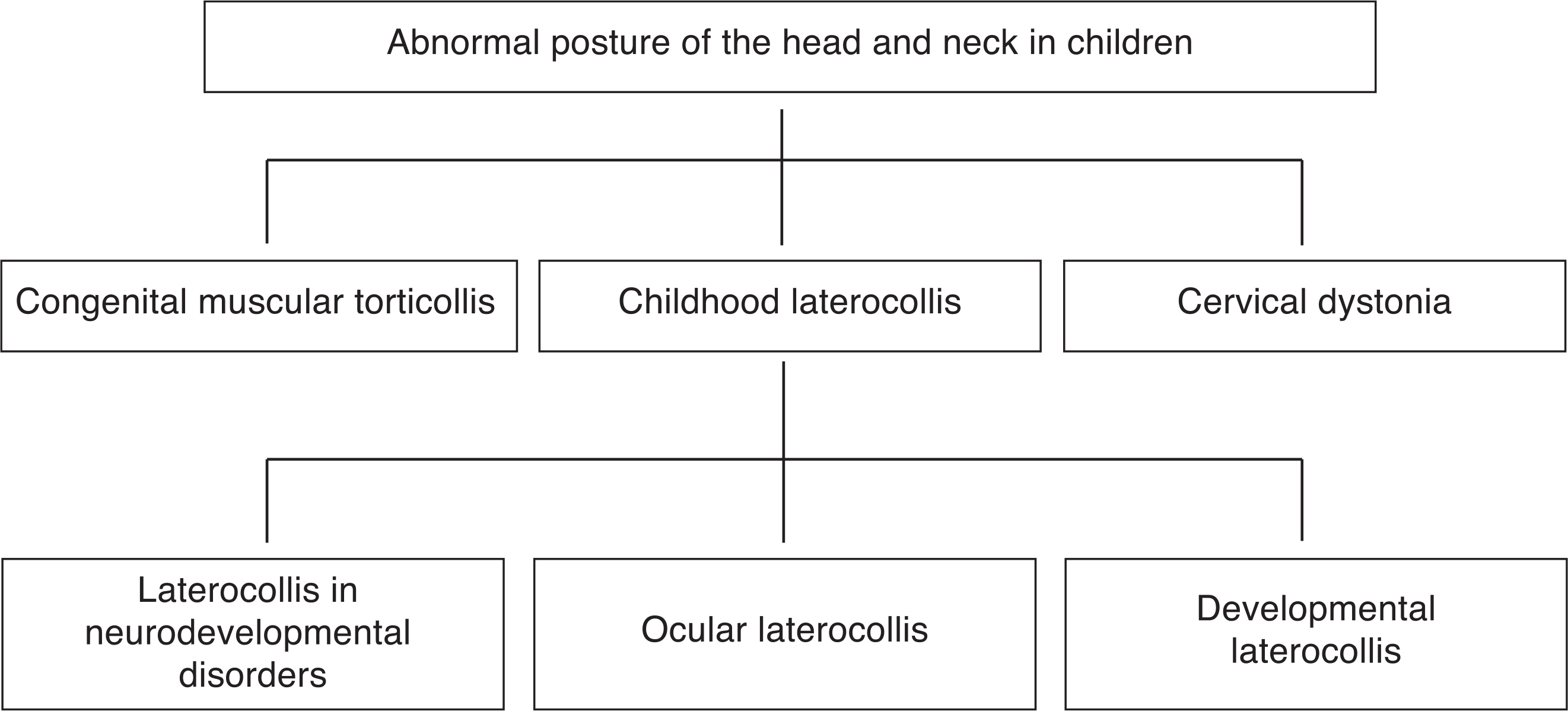
Differential diagnosis of abnormal posture of the head and neck in children.
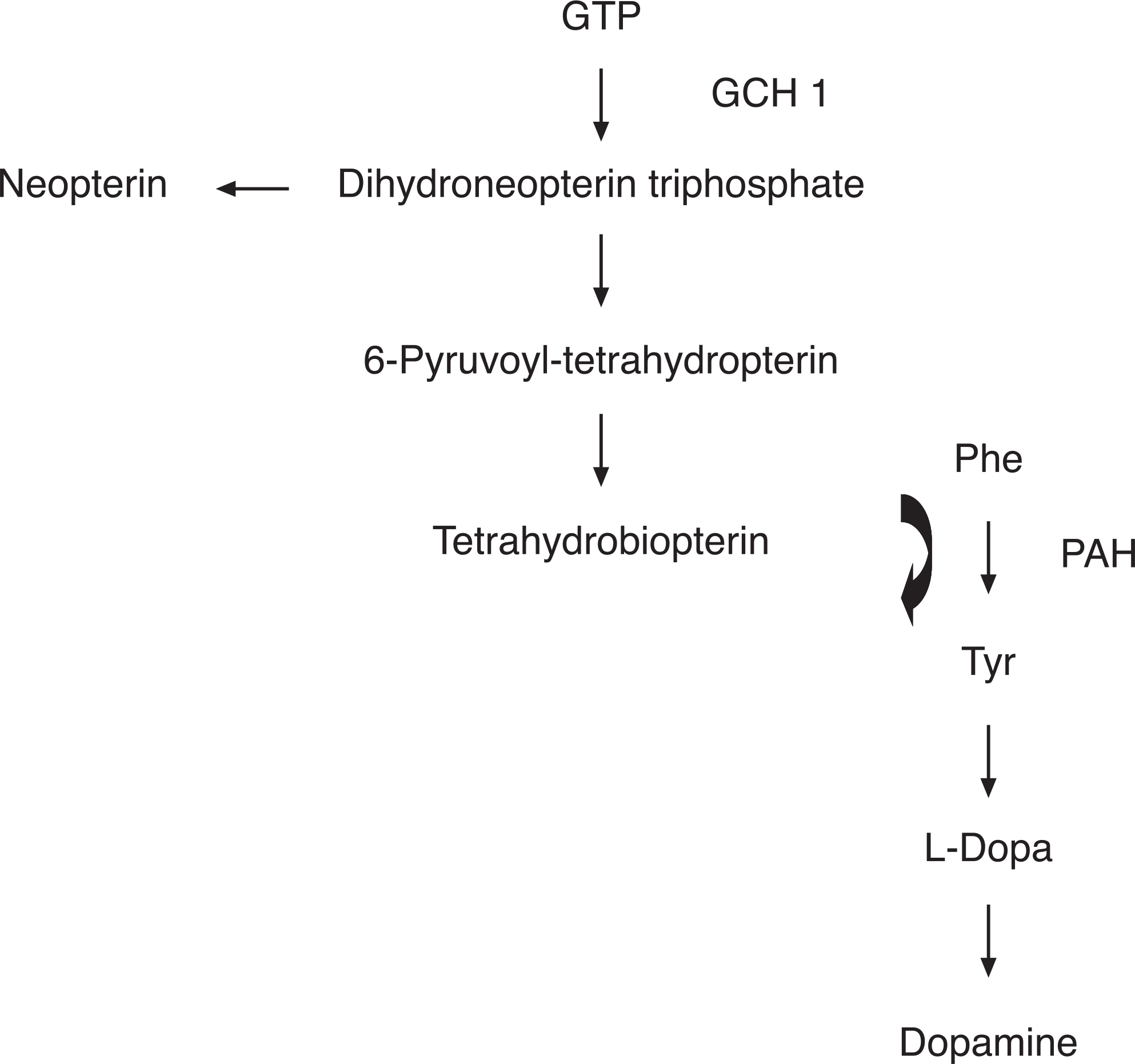
The biosynthetic pathway of tetrahydrobiopterin and dopa from guanosine triphosphate (GTP). GCH 1:GTP cyclohydrolase I, Phe: phenylalanine, Try: tyrosine.

Doses and muscles to inject as first line therapy, as well as maximum does, depending on the type of cervical dystonia