









 |
 |
| J Korean Med Assoc > Volume 52(6); 2009 > Article |
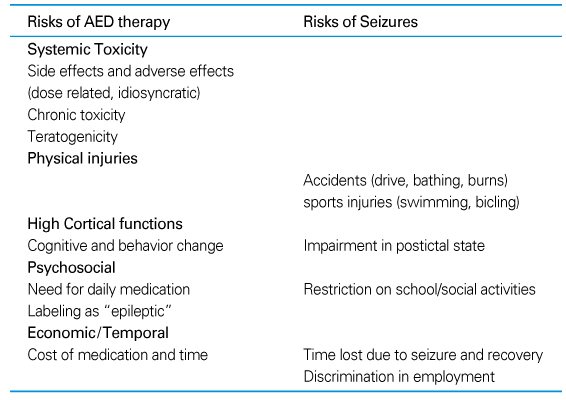
Abstract
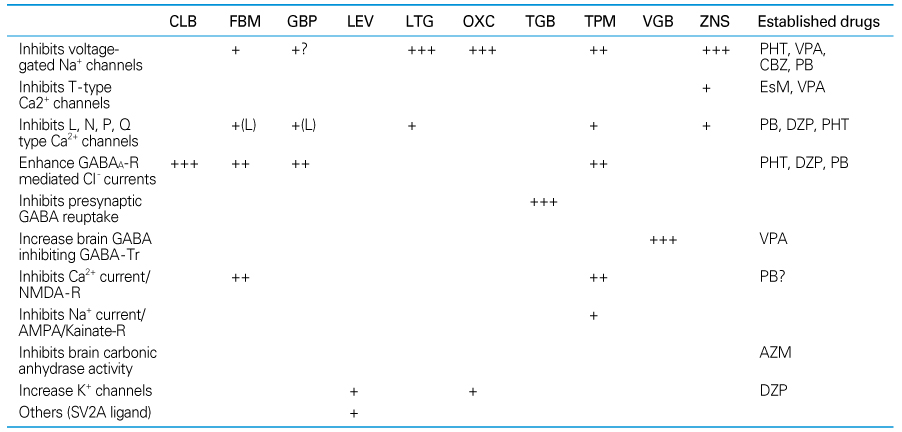
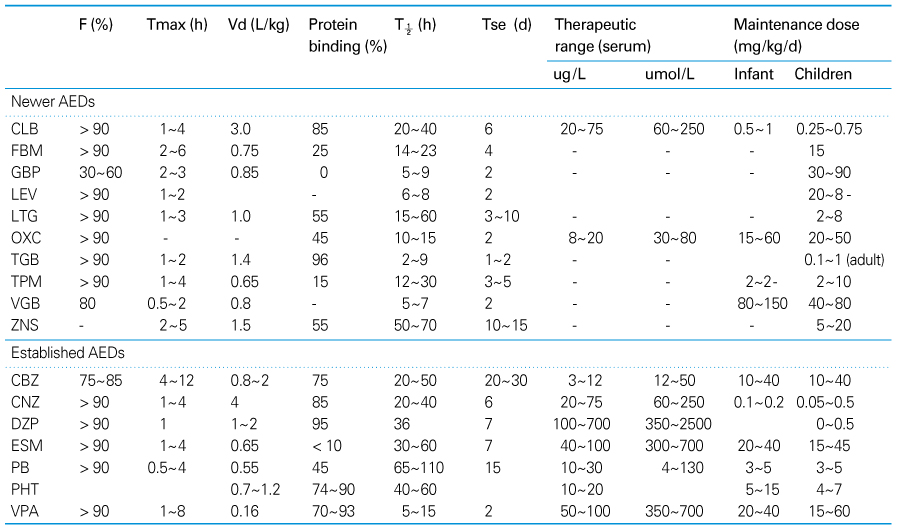
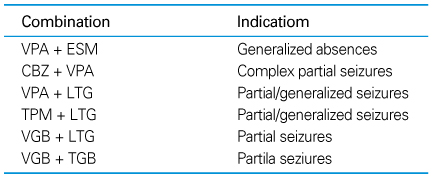
Many new antiepileptic drugs (AEDs) have been developed in the last two decades, contributing to the optimal treatment for childhood epilepsy. The goal of the treatment is to achieve seizure-free without any side effects, that deteriorates the quality of life by causing negative consequences. The new AEDs have not shown better efficacy, but generally seem to be better tolerated, having fewer systemic reactions and better pharmacokinetics than the established AEDs. The new AEDs have a broad spectrum of activities, which offer new opportunities to patients who have not shown any favorable responses to the established ones. There are more choices when trying to select AEDs for epileptic seizures and syndromes. Majority of the new AEDs have more than one action mechanism. AEDs acting selectively through the GABAergic system are tiagabine and vigabatrin; acting by inhibition of voltage-dependent Na+ and Ca2+ channels are lamotirigine, oxcabarbazepine and topiramate; and acting by inhibition of glutamate-mediated excitation are felbamate, topiramate. The pharmacokinetic parameters of the new AEDs compared to the established AEDs, new AEDs have improved in terms of longer half-lives, permitting less frequent daily dosing, reduced potential for drug interactions. Considerations in selecting an AEDs are not only dependent on seizure types or syndromes, side effect profile, action mechanism, drug interaction, pharmacokinetic profile, facility of drug initiation, but also on age and sex of patients. Patients with worsened seizure frequency or development of new types of seizure after the introduction of AEDs, should be questioned on the previously diagnosed seizure types or syndromes.
References
1. Ben-Menachem E. Strategy for utilization of new antiepileptic drugs. Curr Opin Neurol 2008;21:167-172.
2. Rho JM, Sanker R. The pharmacologic basis of antiepileptic drug action. Epilepsia 1999;40:1471-1483.
3. Meldrum BS. Update on the mechanism of action of antiepileptic drugs. Epilepsia 1996;37:S6. S4-S11.
4. Bourgeois BFD. In: Wyllie E, editor. Pharmacokinetics and pharmacodynamics of antiepileptic drugs. The treatment odepilepsy. practice & practice 2001;3rd ed. Pholadelphia: Lippincott Williams & Wilkins. 729-757.
5. French JA, Kanner AM, Bautista J, Abou-Khalil B, Browne T, Harden CL, Theodore WH, Bazil C, Stern J, Schachter SC, Bergen D, Hirtz D, Montouris GD, Nespeca M, Gidal B, Marks WJ Jr, Turk WR, Fischer JH, Bourgeois B, Wilner A, Faught RE Jr, Sachdeo RC, Beydoun A, Glauser TA. Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Quality Standards Subcommittee of the American Academy of Neurology. American Epilepsy Society. Efficacy and tolerability of the new antiepileptic drugs I: treament of new onset epilepsy. Neurology 2004;62:1252-1260.
6. Beyenburg S, Bauer J, Reuber M. New drugs for treatment of epilepsy: a practical approach. Postgrad Med J 2004;80:581-587.
7. Brodie MJ, Schachter SC, Kwan P. Fast Facts:Epilepsy 2005;3rd ed. Oxford: Health Press.
8. O'Dell C, Shinnar S. Initiation and discontinuation of antiepileptic drugs. Neurol Clin 2001;19:289-311.
9. Sankar R. Initial treatment of epilepsy with antiepileptic drugs; Pedaitric issues. Neurology 2004;63:S4. S30-S39.
10. Wolfig AA. Monotherapy in children and infants. Neurology 2007;69:S3. 17-22.
11. Sazgar M, Bourgois BFD. Aggravation of epilepsy by abtiepileptic drugs. Pediatr Neurol 2005;33:227-234.
Figure 1
An excitatory synapse. the putative major sites of action of various AEds.
MDA: N-methyl-D-asparate, AMPA: a-amino-3-hydroxy-4-isoxazo-lepropionic acid (2).
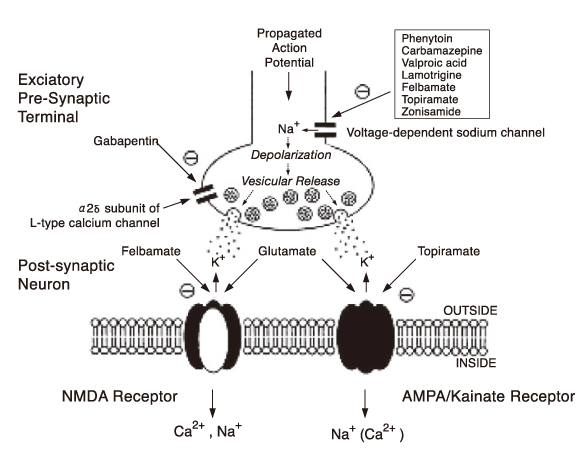
Figure 2
An inhibitory synapse. the putative major sites of action of various AEds.
GABA: γ-aminobutyric acid, GABA-T, GABA transaminase, GAD: glutamic acid decarboxylase (2).

Figure 3
Plasma concentration of a drug following repeated oral drug administration (4) as a function of interval of administration measured as multiples of elimination half-life.

Figure 4
Relationship between serum drug concentration (ordinate) and drug dose (abscissa) for a drug observing (B) first-order kinetics (linear) and (A, C) zero-order kinetics (4) A, PHT, ZNS; B, FBM, ESM, PB, TPM, VPA,OXC, LEV, ZNS; C, LTG, VPA.
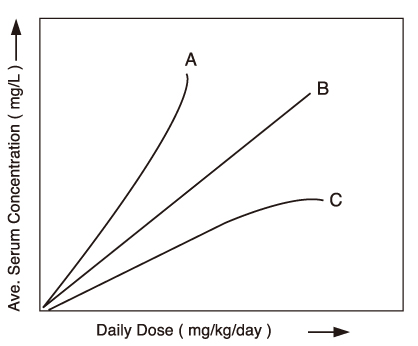
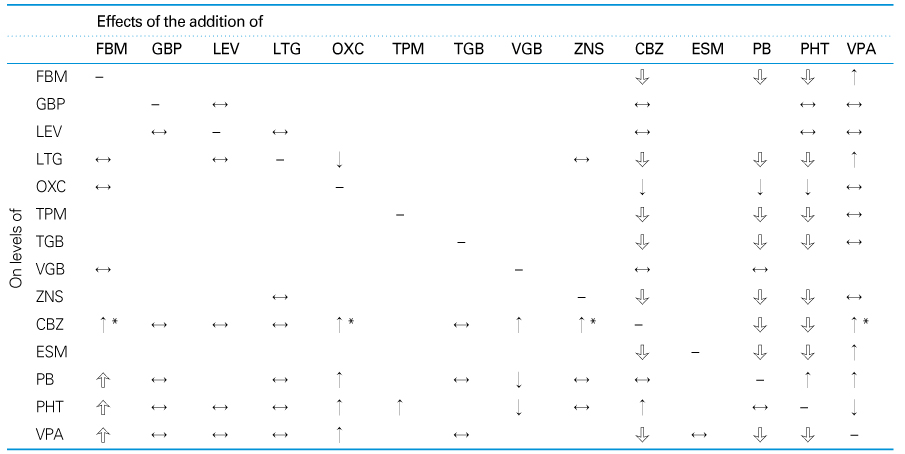
Table 6
The changes of concentration by the interaction between new AEDs and other drugs

↔, no interaction, F-1, decrease in progestin; F-2, increase in wafarin; G-1and G-2, decrease in GBP L-1, decrease in LTG; L-2, increase in LTG; O-1, decrease in cyclosporine; O-2, decrease in ethinyl estradiol; T-1, decrease in digoxin; T-2, decrease in ethinyl estradiol; T-3, increase in haloperidol.
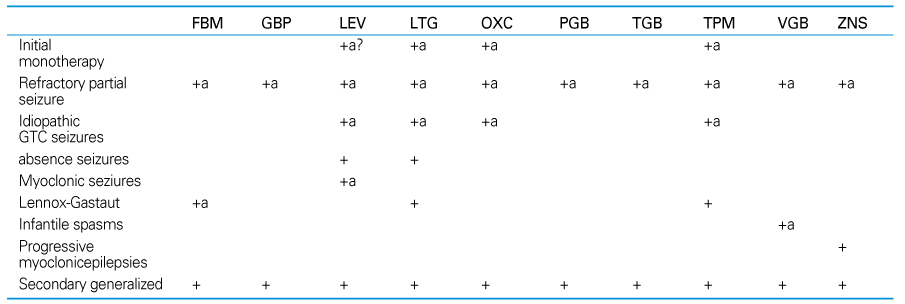
Table 10
Summary of Pediatric epilepsy syndromes and treatments*

* based on less than class I and class II evidence (5).
BECTS, benign epilepsy of childhood with centrotemporal spikes; CJAE, childhood and juvenile absence epilepsy; JME, juvenile myoclonic epilepsy; GTC, generalized tonic-clonic seizures.
Table 12
Comparison of recommendations for treatment of pediatric epilepsy (10)
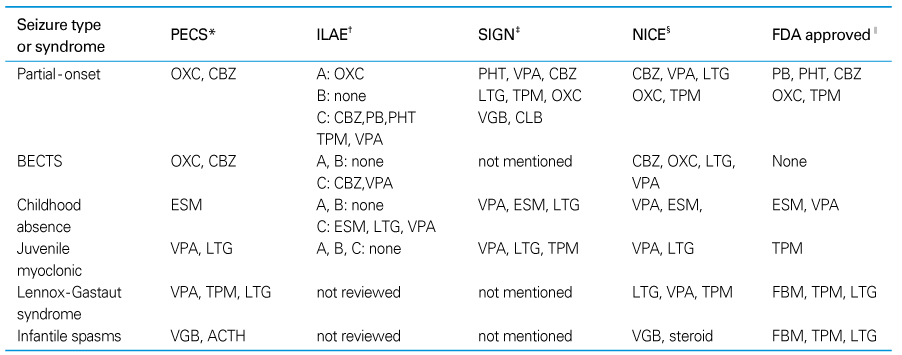
BECT, BECTS, benign epilepsy of childhood with centrotemporal spikes.
* Pediatric Expert Consensus survey. Drugs rated as treatment of choice listed
† International League Against Epilepsy, Recommendations listed according to levels of evidence supporting the efficacy options. Level A, B, C (French JA, Kanner AM, Bautista J, et al. Efficacy and tolerability of the new antiepileptic drug I: treatment of new onset epilepsy. Neurology 2004; 62: 1252 -1260)
‡ SIGN: scottish intercollegiate guideline network. Diagnosis and manegement of epilepsies in children and young people; A national clinical guideline Edinburgh, SIGN: MArch 2005. (Copies available at: http://www.sign.ac.uk/pdf/sign81.pdf)
§ National Institute for Clincal Excellence, Technology Appraisal Guidance 79. Newer drugs for epilepsy in children (www.nice.org/uk/TA079 guidance) and Clinical guidance 20. The epilepsies: The diagnosis and mangement of the epilepsies in adults and children in primary and secondary care, October 2004 (www.nice.org/uk/CG020NICE guideline).
∥ FDA approval for each selzures type or epilepsy syndrome.
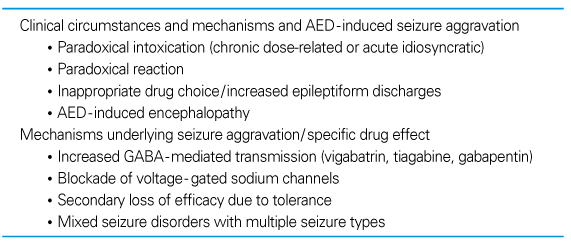
Table 18
AED-induced aggravation of seizures or epileptic syndromes (11)

+, limited; ++, moderate; +++. significant.
JME, juvenile myoclonic epilepsy; LGS, Lennox-Gastaut syndrome; MAE, myoclonic astatic epilepsy; BECTS, benign epilepsy of childhood with centrotemporal spikes; SMEI, severe myoclonic epilepsy of infancy; LKS, Landau-Kleffner syndrome; ESES, electrical status epilepticus of sleep.
- TOOLS
-
- Share :
-





-
METRICS

-
- 1 Crossref
- Scopus
- 1,366 View
- 19 Download
-

-
Related articles in
J Korean Med Assoc -
Adverse Effects of Antiepileptic Drugs2005 June;48(6)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
