



 |
 |
| J Korean Med Assoc > Volume 52(4); 2009 > Article |
Abstract
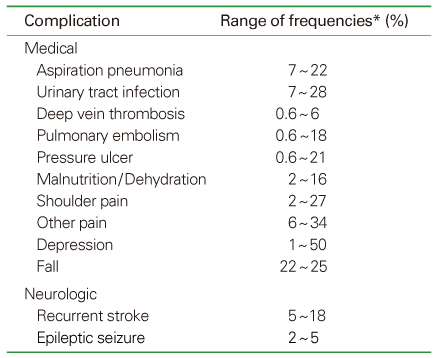
Acute complications following stroke may increase mortality and impede functional recovery. Most of the complications are treatable and preventable. Close monitoring of the complications and proper management are necessary for the better outcome of the patients. Common complications include aspiration pneumonia, dysphagia, urinary tract infection, incontinence, malnutrition, deep vein thrombosis, pressure sore, fall, pain, seizure, and depression. Proper positioning and early mobilization are recommended to prevent major complications. Aspiration pneumonia is one of the frequent causes of death in acute stroke setting. Dysphagia screening should be done to evaluate the risk of aspiration. If oral feeding is not safe, nasogastric tube feeding should be considered. The majority of urinary tract infections in acute stroke are associated with the use of indwelling catheters, therefore prolonged indwelling catheterization should be avoided. Nutritional assessment and supplements are necessary in acute stroke patients. Low dose subcutaneous heparin or low molecular weight heparin should be considered for patients with high risk of deep vein thrombosis. If heparin is contraindicated, compressive stockings are an alternative. Regular assessment for skin breakdown and fall risk is recommended for all patients. Shoulder pain is also one of the frequent complications in stroke patients. Proper handling and mobilization in acute stage may prevent shoulder pain. Administration of anticonvulsants may prevent recurrent post-stroke seizures. Depression may limit functional outcome by inhibiting patient motivation and treatment with antidepressants should be considered. Proper management of acute complications needs multidisciplinary team approach that consists of physicians, nurses, therapists, and nutritionists. Adequate prevention and management of complications may improve functional outcome of acute stroke.
References
1. Oppenheimer S, Hachinski V. Complications of acute stroke. Lancet 1992;339:721-724.
2. Worp HB, Kappelle LJ. Complications of acute ischemic stroke. Cerebrovasc Dis 1998;28:2180-2184.
3. Langhorne P, Stott DJ, Robertson L, MacDonald J, Jones L, McAline C, Dick F, Taylor GS, Murray G. Medical complications after stroke: a multicenter study. Stroke 2000;31:1223-1229.
4. Bae HJ, Yoon DS, Lee J, Kim BK, Koo KJ, Kwon O, Park JM. In-hospital medical complications and long-term mortality after ischemic stroke. Stroke 2005;36:2441-2445.
5. Brandstater ME. In: Delisa JA, editor. Stroke rehabilitation. Physical medicine and rehabilitation 2005;4th ed. Philadelphia: Sauders. 1656-1676.
6. Davenport RJ, Dennis MS, Welwood I, Warlow C. Complications after acute stroke. Stroke 1996;27:415-420.
7. Dobkin BH. Neuromedical complications in stroke patients transferred for rehabilitation before and after diagnostic related groups. J Neurol Rehab 1987;1:3-7.
8. Dromerick A, Reding M. Medical and neurological complications during stroke rehabilitation. Stroke 1994;25:358-361.
9. Indredavik B, Rohweder G, Naalsund E, Lydersen S. Medical complications in a comprehensive stroke unit and an early supported discharge service. Stroke 2008;39:414-420.
10. Johnston KC, Li JY, Lyden PD, Hanson SK, Feasby TE, Adams RJ, Faught RE, Haley EC. for the RANTTAS Investigators. Medical and neurological complications of ischemic stroke: experience from the RANTTAS trial. Stroke 1998;29:447-453.
11. Kalra L, Yu G, Wilson K, Roots P. Medical complications during stroke rehabilitation. Stroke 1995;26:990-994.
12. Roth JE, Lovell L, Harery RL, Heinemann AW, Semik P, Diaz S. Incidence of and risk factors for medical complications during stroke rehabilitation. Stroke 2001;31:523-529.
13. Weimer C, Ziegler A, Konig IR, Diener HC. on behalf of the German Stroke Date Collaborators. Prediction of functional outcome and survival after acute ischemic stroke. J Neurol 2002;249:888-895.
14. Kaste M, Roine RO. In: Mohr JP, Choi DW, et al, editor. General stroke management and stroke units. Stroke: Pathophysiology, diagnosis, and management 2004;4th ed. Philadelphia: Churchill Livingstone. 971-1024.
15. Adams HP, del Zoppo G, Alberts MJ, Bhatt DL, Brass L, Furlan A, Grubb RL, Higashida RT, Jauch EC, Kidwell C, Lyden PD, Morgenstern LB, Qureshi AI, Rosenwasser RH, Scott PA, Wijdicks EF. Guidelines for the early management of adults with ischemic stroke. Stroke 2007;38:1655-1711.
16. European Stroke Organisation Executive Committee and the ESO Writing Committee. Guidelines of management of ischaemic stroke and transient ischaemic attack 2008. Cerebrovasc Dis 2008;16:311-337.
17. Han TR, Kim YH, Paik NJ. In: Han TR, Bang MS, editor. Stroke rehabilitation. Rehabilitation medicine 2008;3rd ed. Seoul: Koonja Publishing. 509-548.
18. Ellwood PM. In: Kottke FJ, Lehmann JF, editor. Bed positioning. Handbook of physical medicine and rehabilitation 1990;4th ed. Philadelphia: W.B. Saunders. 520-528.
19. Aviv JE, Sacco RL, Thomson J, Tandon R, Diamond B, Martin JH, Close LG. Silent laryngopharyngeal sensory deficits after stroke. Ann Otol Rhinol Laryngol 1997;11:609-622.
20. Martino R, Foley N, Bhogal S, Diamant N, Speechley M, Teasell R. Dysphagia after stroke: incidence, diagnosis, and pulmonary complications. Stroke 2005;36:2756-2763.
21. Daniels SK, Foundas AL. Lesion localization in acute stroke patients with risk of aspiration. J Neuroimaging 1999;9:91-98.
22. Hammond CA, Goldstein LB. Cough and aspiration of foods and liquids due to oral-pharyngeal dyshagia: ACCP evidence-based clinical practice guideline. Chest 2006;129:154-168.
23. DePippo KL, Holas MA, Reding MJ. Validation of the 3-oz water swallow test for aspiration following stroke. Arch Neurol 1992;49:1259-1261.
24. Duncan PW, Zorowitz R, Bates B, Choi JY, Glasberg JJ, Graham GD, Katz RC, Lamberty K, Reker D. Management of adult stroke rehabilitation care: a clinical practice guideline. Stroke 2005;36:e100-e143.
25. Kim IS, Han TR. Evaluation and management of dysphagia. Korean J Stroke 2006;8:40-48.
26. Palmer JB, Drennan JC, Baba M. Evaluation and treatment of swallowing impairments. Am Fam Physician 2000;61:2453-2462.
27. Norton B, Horner-Ward M, Donnely MT, Long RG, Holmes GK. A randomized prospective comparison of percutaneous endoscopic gastrostomy and nasogastric tube feeding after acute dysphagic stroke. BMJ 196;312:13-16.
28. Blauer D. The natural history and functional consequences of dysphagia after hemispheric stroke. J Neurol Neurosurg Psychiatry 1989;52:236-241.
29. Warren JW. Catheter-associated urinary tract infections. Infect Dis Clin North Am 1997;11:609-622.
30. Nakayama H, Jorgensen HS, Pedersen PM, Raaschou HO, Olsen TS. Prevalence and risk factors of incontinence after stroke. The Copenhagen Stroke Study. Stroke 1997;28:58-62.
31. Axelsson K, Asplund K, Norberg A, Alafuzoff I. Nutritional status in patients with acute stroke. Acta Med Scand 1988;224:217-224.
32. Brandstater ME, Roth EJ, Siebens HC. Venous thromboembolism in sroke: Literature review and implications for clinical practice. Arch Phys Med Rehabil 1992;73:s379-s391.
33. Sandercock PA, Counsell C, Tseng MC. Low-molecular-weight heparins or heparinoids versus standard unfractionated heparin for acute ischaemic stroke. Cochrane Database Syst Rev 2008;3:CD000119.
34. Kamran SI, Downey D, Ruff RL. Pneumatic sequential compression reduces the risk of deep vein thrombosis in stroke patients. Neurology 1998;50:1683-1688.
35. Kelly J, Rudd A, Lewis R, Hung BJ. Venous thrombo-embolism after acute stroke. Stroke 2001;32:262-267.
36. Harvey RL, Green D. Deep venous thrombosis and pulmonary embolism in stroke. Top Stroke Rehabil 1996;3:54-70.
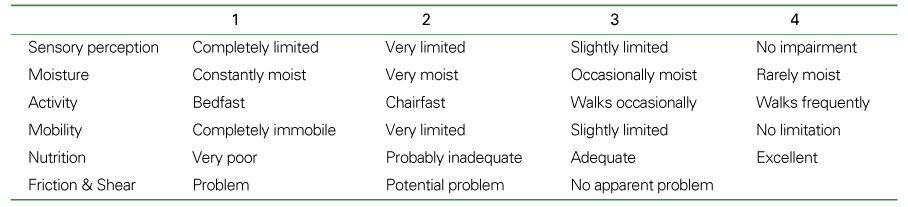
37. Berlowitz Dr, Brandeis GH, Morris JN, Ash AS, Anderson JJ, Kader B, Moskowtz MA. Deriving a risk-adjustment model for pressure ulcer development using the Minum Data Set. J Am Geriatr Soc 2001;49:866-871.
38. Bergstrom N, Braden BJ, Laguzza A, Holman V. The Braden scale for predicting pressure sore risk. Nurs Res 1987;36:205-210.
39. Reddy M, Gill SS, rochon PA. Preventing pressure ulcers: a systematic review. JAMA 2006;296:974-984.
40. Salcido R, Goldman R. In: Braddom RL, Buschbacher RM, et al, editor. Prevention and management of pressure ulcers and other chronic wounds. Physical medicine and rehabilitation 2000;2nd ed. Philadelphia: W.B. Saunders. 645-664.
41. Forster A, Young J. Incidence and consequences of falls due to stroke: a systematic inquiry. BMJ 1995;311:83-86.
42. Teasell R, McRae M, Foley N, Bhardwaj A. The incidence and consequences of falls in stroke patients during inpatient rehabilitation: factors associated with high risk. Arch Phys Med Rehabil 2002;83:329-333.
43. Parker MJ, Gillespie LD, Gillespie WJ. Hip protectors for preventing hip fractures in the elderly. Cochrane Database Syst Rev 2001;CD001255.
44. Van Onwenaller C, LaPlace PM, Chartraine A. Painful shoulder in hemiplegia. Arch Phys Med Rehabil 1985;67:23-26.
45. Lindgren I, Jonsson AC, Norrving B, Lindgren A. Shoulder pain after stroke: a prospective population-based study. Stroke 2007;38:343-348.
46. Ada L, Foongchomcheay A, Canning C. Supportive devices for preventing and treating subluxation of the shoulder after stroke. Cochrane Database Syst Rev 2005;CD003863.
47. van Kuijk AA, Geurts AC, Bevaart BJ, van Limbeek J. Treatment of upper extremity spasticity in stroke patients by focal neuronal or neuromuscular blockade: a systematic review of the literature. J Rehabil Med 2002;34:51-61.
48. Hansson P. Post-stroke pain case study: clinical characteristics, therapeutic options and long-term follow-up. Eur J Neurol 2004;11:22-30.
49. Frese A, Husstedt IW, Ringelstein EB, Evers S. Pharmacologic treatment of central post-stroke pain. Clin J Pain 2006;22:252-260.
50. Olsen TS. Post-stroke epilepsy. Curr Atheroscler Rep 2001;3:340-344.
51. Camilo O, Goldstein LB. Seizures and epilepsy after ischemic stroke. Stroke 2004;35:1769-1775.
52. Ryvlin P, Montavont A, Nighoghossian N. Optimizing therapy of seizures in stroke patients. Neurology 2006;67:S3-S9.
53. Robinson RG, Starr LB, Kubos KL, Price TR. A two-year longitudinal study of post-stroke mood disorders: findings during the initial evaluation. Stroke 1983;14:736-741.
54. Robinson RG, Szetela B. Mood change following left hemisphere brain injury. Ann Neurol 1981;9:447-453.
55. Thomas SA, Lincoln NB. Factors relating to depression after stroke. Br J Clin Psychol 2006;45:49-61.
56. Kauhanen M, Korpelainen JT, Hiltunen P, Brusin E, Mononen H, Maatta R, Nieminen P, Sotaniemi KA, Myllyla VV. Poststroke depression correlates with cognitive impairment and neurological deficits. Stroke 1999;30:1875-1880.
57. Hackett ML, Anderson CS, House AO. Management of depression after stroke: a systematic review of pharmacological therapies. Stroke 2005;36:1098-1103.
58. Bhogal SK, Teasell R, Foley N, Speechley M. Heterocyclics and selective serotonin reuptake inhibitors in the treatment and prevention of poststroke depression. J Am Geriatr Soc 2005;53:1051-1057.
Table 2
AHA/ASA-endorsed guidelines for assessment of swallowing

*Recommendation level
A: a strong recommendation that the intervention is always indicated and acceptable, B: a recommendation that the intervention may be useful/effective, C: a recommendation that the intervention may be considered, D: a recommendation that a procedure may be considered not useful/effective, or may be harmful, I: Insufficient evidence to recommend for or against; clinical judgment should be used.
Table 3
AHA/ASA-endorsed guidelines for prevention of deep vein thrombosis
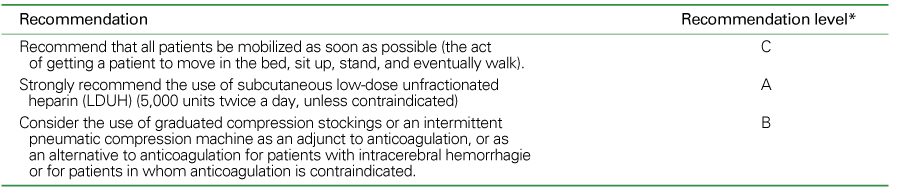
*Recommendation level
A: a strong recommendation that the intervention is always indicated and acceptable, B: a recommendation that the intervention may be useful/effective, C: a recommendation that the intervention may be considered, D: a recommendation that a procedure may be considered not useful/effective, or may be harmful, I: Insufficient evidence to recommend for or against; clinical judgment should be used.
Table 5
AHA/ASA-endorsed guidelines for prevention of pressure ulcer

*Recommendation level
A: a strong recommendation that the intervention is always indicated and acceptable, B: a recommendation that the intervention may be useful/effective, C: a recommendation that the intervention may be considered, D: a recommendation that a procedure may be considered not useful/effective, or may be harmful, I: Insufficient evidence to reco-mmend for or against; clinical judgment should be used.
- TOOLS
-
- Share :
-





-
METRICS

-
Related articles in
J Korean Med Assoc -
Treatment of neuropathic pain2021 July;64(7)
Management of severe pediatric obesity2021 June;64(6)
Evaluation and improvement of adherence to medication2021 February;64(2)
Anesthetic management of hypertensive patients2020 September;63(9)
Orthopaedic Management of Ankylosing Spondylitis1997 January;40(1)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
