






 |
 |
| J Korean Med Assoc > Volume 51(4); 2008 > Article |
Abstract
Coronary artery disease in young patients (< 40 years) is not common. However, when it occurs it has symptoms that are more frequent and a more rapid progression when compared to older affected patients. Younger patients are more likely to have normal coronary arteries and have nonobstructive disease < 70%, single-vessel disease and less extensive coronary artery atherosclerosis. Therefore, it is likely that there are differences in the cardiac risk factors in young patients undergoing coronary artery bypass surgery. Smoking, hypercholesterolemia, unstable angina, and myocardial infarction were more frequent in the young age group, and diabetes and hypertension were more common in older patients. The need for repeated interventions, additional surgery andlate myocardial infarction were more common in younger patients. Favorable factors associated with increased survival included the absence of unstable angina, a left ventricle ejection fraction of =45% and the use of the internal thoracic artery for procedures. The patency of saphenous vein grafts in younger patients was inferior to vein graft patency in the older patients. Risk factors such as hyperlipidemia, smoking and a family history of coronary artery disease may be related to the early graft failure in young patients. The patency of the internal thoracic artery to the left anterior descending artery was above 90% over 10 years; however, it was around 50% for the saphenous vein. Therefore, the aggressive use of internal thoracic arteries, for coronary artery bypass surgery in young patients, was essential for improved late survival and the event free survival (reduced additional interventions, surgeries and hospital admissions). The Y-composite graft technique or sequential anastomosis, improves the coronary artery anastomosis with fewer arterial grafts. Other arterial grafts such as the gastroepiploic artery, radial artery and inferior epigastric artery could be used for coronary artery bypass surgery in young patients for free grafts, in situ grafts or Y-composite grafts. Young patients that have coronary artery bypass surgery have a favorable prognosis when the internal thoracic arteries or other arterial grafts are used. In addition, such as the Y-composite graft technique and sequential anastomosis can also be used with a high success rate.
References
1. Zimmerman FH, Cameron F, Fisher LD, Ng G. Myocardial infarction in young adults: angiographic characterization, risk factors and prognosis (coronary artery surgery study registry). J Am Coll Cardiol 1995;26:654-661.
2. Kannel WB, Abbott RD. Incidence and prognosis of unrecognized myocardial infarction. N Engl J Med 1984;311:1144-1147.
3. Mosca L. In: Fuster V, Topol EJ, Nabel EG, editor. Estrogen and Atherothrombosis. Atherothrombosis & coronary artery disease 2005;Philadelphia: Lippincott Williams and Wilkins. 297-307.
4. Uddin SN, Siddiqui NI, Bagum F, Malik F, Rahman S, Ali MS. Coronary artery disease in young adults-angiographic profile. Mymensingh Med J 2004;13:11-15.
5. Rohrer-Gubler I, Niederhauser U, Turina MI. Late outcome of coronary artery bypass grafting in young versus older patients. Ann Thorac Surg 1998;65:377-382.
6. Graziosi GC, Wolterbeek DW, Kappetein AP, Huysmans HA. Risk factors in coronary artery bypass surgery for patients 40 years of age and younger. Thorac Cardiovasc Surg 1994;42:259-263.
7. Malinowski M, Mrozek R, Twardowski R, Malinowski M, Mrozek R, Twardowski R, Biernat J, Deja MA, Widenka K, Dalecka AM, Kobielusz-Gembala I, Janusiewicz P, Wos S, Golba KS. Left internal mammary artery improves 5-year survival in patients under 40 subjected to surgical revascularization. Heart Surg Forum 2006;9:E493-E498.
8. Samuels LE, Sharma S, Kaufman MS, Morris RJ, Brockman SK. Coronary artery bypass grafting in patients in their third decade of life. J Card Surg 1996;11:402-407.
9. Kelly TF, Craver JM, Jones EL, Hatcher CRJ. Coronary revascularization in patients 40 years and younger: survival experience and long-term follow-up. Am Surg 1978;44:675-678.
10. Lytle BW, Loop LD. Coronary artery bypass grafting in young adults. Chest 1987;91:291-292.
11. van Son JAM, Smedts F, Vincent JG, van Lier HJJ, Kubat K. Comparative anatomic studies of various arterial conduits for myocardial revascularization. J Thorac Cardiovasc Surg 1990;99:703-707.
12. Li XN, Stulz P, Siebenmann PP, Li XN, Stulz P, Siebenmann RP, Yang Z, Lüscher TF. Different effects of activated platelets in the right gastroepiploic and internal mammary arteries. J Thorac Cardiovasc Surg 1992;104:1294-1302.
13. Rosenfeldt FL, He GW, Buxton BF, Angus JA. Pharmacology of coronary artery bypass grafts. Ann Thorc Surg 1999;67:878-888.
14. Tector AJ, Amundsen S, Schmahl TM, et al. Total revas-cularization with T grafts. Ann Thorac Surg 1994;57:33-39.
15. Pick AW, Orszulak TA, Anderson BJ, et al. Single versus bilateral internal mammary artery grafts: 10-year outcome analysis. Ann Thorac Surg 1997;64:599-605.
16. Lytle BW, Blackstone EH, Loop FD. Two internal thoracic artery grafts are better than one. J Thorac Cardiovasc Surg 1999;117:855-872.
17. Pym J, Brown PM, Charrette EJ, Parker JO, West RO. Gastroepiploic-coronary anastomosis. A viable alternative bypass graft. J Thorac Cardiovasc Surg 1997;94:256-259.
18. Acar C, Jebara VA, Portoghese M, Acar C, Jebara VA, Portoghese M, Beyssen B, Pagny JY, Grare P, Chachques JC, Fabiani JN, Deloche A, Guermonprez JL. Revival of the radial artery for coronary artery bypass grafting. Ann Thorac Surg 1992;54:652-659.
19. Maniar HS, Sundt TM, Barner HB, Maniar HS, Sundt TM, Barner HB, Prasad SM, Peterson L, Absi T, Moustakidis P. Effect of target stenosis and location on radial artery graft patency. J Thorac Cardiovasc Surg 2002;123:45-52.
20. Sauvage LR, Wu H, Kowalsky TE, Sauvage LR, Wu HD, Kowalsky TE, Davis CC, Smith JC, Rittenhouse EA, Hall DG, Mansfield PB, Mathisen SR, Usui Y. Healing basis and surgical techniques for complete revascularization of the left ventricle using only the internal mammary arteries. Ann Thorac Surg 1986;57:33-39.
21. Tector A, McDonald ML, Kress DC, Downey FX, Schmahl TM. Purely internal thoracic artery grafts: outcomes. Ann Thorac Surg 2001;72:450-455.
22. Calafiore AM, Di Giammarco G. Complete revascularization with three or more arterial conduits. Sem Thorac Cardiovasc Surg 1996;8:15-23.
23. Mavroudis C, Backer CL, Muster AJ, Mavroudis C, Backer CL, Muster AJ, Pahl E, Sanders JH, Zales VR, Gevitz M. Expanding indications for pediatric coronary artery bypass. J Thorac Cardiovasc Surg 1996;111:181-189.
24. Basso C, Maron BJ, Corrado D, Thiene G. Clinical profile of congenital coronary artery anomalies with origin from the wrong aortic sinus leading to sudden death in young competitive atheletes. J Am Coll Cardiol 2000;35:1493-1501.
25. Ghosh PK. Anomalous origin of the right coronary artery. Eur J Cardiothorac Surg 1997;12:164-165.
26. Daehnert I, Rotzsch C, Krause S, Dorszewski A, Kostelka M. Synconpe in a child owing to intramural course of the left coronary artery. Acta Paediatr 2003;92:1339-1342.
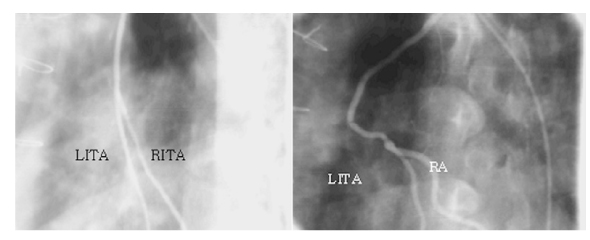
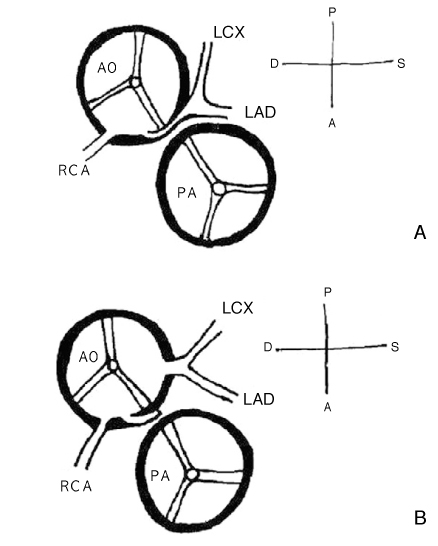
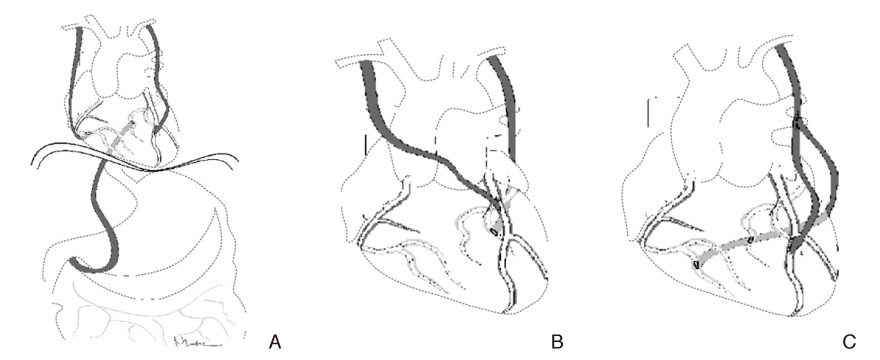
Figure 1
Variable techniques of total arterial revascularization.
(A) In situ LITA to left anterior descending artery (LAD), in situ RITA to distal right coronary artery (RCA), in situ GEA to posterolateral branch or obtuse marginal (OM) branch
(B) In situ RITA to LAD, in situ LITA to OM
(C) Y-composite graft
LITA to LAD, RITA (from LITA) to OM to PDA ( sequential anastomosis)
- TOOLS
-
- Share :
-





-
METRICS

-
- 0 Crossref
- Scopus
- 1,095 View
- 7 Download
-

-
Related articles in
J Korean Med Assoc
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
