





 |
 |
| J Korean Med Assoc > Volume 50(12); 2007 > Article |
Abstract
Airway management is still perceived as the greatest patient safety issue and the key task that anesthesiologists perform. Management includes mask ventilation, use of a laryngoscope, and the endotracheal intubation and extubation of the patient. Difficulty can be encountered at any of these stages, and can be a major cause of anesthesia-related morbidity and mortality. Competence in airway management requires knowledge of the anatomy and physiology of the airway, ability to access the patient's airway for the anatomic features that correlate with difficulties in airway management, skill with the many devices used in airway management, including a variety of recently-introduced airway tools, and the appropriate application of the sophisticated algorithm for difficult airway management. Development and clinical distribution of supraglottic airway devices and their enhancement, as well as the broad acceptance of awake fiber-optic intubation, has led to profound changes in the strategy for managing a difficult airway. Including the American Society of Anesthesiologists, many countries have developed their own airway management algorithm these days. Nevertheless, massive national and international deficits still exist in implementing these guidelines into practice as well as the implicated structural requirements with respect to education, reflection, team building and equipment concerning each individual institution. In regard to this situation, it is the recommendation of the author that our country develop and institute such a standardized system of airway management.
References
1. Henderson JJ, Popat MT, Latto IP, Pearce AC. Difficult Airway Society guidelines for management of the unanticipated difficult intubation. Anaesthesia 2004;59:675-694.
2. Caplan RA, Posner KL, Ward RJ, Cheney FW. Adverse respiratory events in anesthesia: A closed claims analysis. Anesthesiology 1990;72:828-833.
3. American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Practice guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology 2003;98:1269-1277.
4. Rocke DA, Murray WB, Rout CC, Gouws E. Relative risk analysis of factors associated with difficult intubation in obstetric anesthesia. Anesthesiology 1992;77:67-73.
5. Mallampati SR, Gatt SP, Gugino LD, Desai SP, Waraksa B, Freiberger D, Liu PL. A clinical sign to predict difficult tracheal intubation: a prospective study. Can J Anaesth 1985;32:429-434.
6. Langeron O, Masso E, Huraux C, Guggiari M, Bianchi A, Coriat P, Riou B. Prediction of difficult mask ventilation. Anesthesiology 2000;92:1229-1236.
7. Rose DK, Cohen MM. The airway: problems and predictions in 18,500 patients. Can J Anaesth 1994;41:372-383.
8. Williamson JA, Webb RK, Szekely S, Gillies ER, Dreosti AV. Difficult intubation: an analysis of 2000 incident reports. Anaesth Intensive Care 1993;21:602-607.
9. Yildiz TS, Solak M, Toker K. Comparison of laryngeal tube with laryngeal mask airway in anaesthetized and paralysed patients. Eur J Anaesthesiol 2007;24:620-625.
10. Joshi GP, Inagaki Y, White PF, Taylor-Kennedy L, Wat LI, Gevirtz C, McCraney JM, McCulloch DA. Use of the laryngeal mask airway as an alternative to the tracheal tube during ambulatory anesthesia. Anesth Analg 1997;85:573-577.
11. Parmet JL, Colonna-Romano P, Horrow JC, Miller F, Gonzales J, Rosenberg H. The laryngeal mask airway reliably provides rescue ventilation in cases of unanticipated difficult tracheal intubation along with difficult mask ventilation. Anesth Analg 1998;87:661-665.
12. Cormack RS, Lehane J. Difficult tracheal intubation in obstetrics. Anaesthesia 1984;39:1105-1111.
13. Knill RL. Difficult laryngoscopy made easy with a BURP. Can J Anaesth 1992;40:279-282.
14. Adnet F, Borron SW, Lapostolle F, Lapandry C. The three axis alignment theory and the sniffing position: perpetuation of an anatomic myth? Anesthesiology 1999;91:1964-1965.
15. Chou HC, Wu TL. A reconsideration of the three axes alignment theory and sniffing position. Anesthesiology 2002;97:753-754.
16. Adnet F, Baillard C, Borron SW, Denantes C, Lefebvre L, Galinski M, Martinez C, Cupa M, Lapostolle F. Randomized study comparing the sniffing position with simple head extension for laryngoscopic view in elective surgery patients. Anesthesiology 2001;95:836-841.
17. Mercer MH, Gabbott DA. Insertion of the Combitube airway with the cervical spine immobilized in a rigid cervical collar. Anaesthesia 1998;53:971-974.
18. Agrò F, Hung OR, Cataldo R, Carassiti M, Gherardi S. Lightwand intubation using the Trachlight. Can J Anaesth 2001;48:592-599.
19. Ferson DZ, Rosenblatt WH, Johansen MJ, Osborn I, Ovassapian A. Use of the Intubating LMA-Fastrach in 254 patients with difficult-to-manage airways. Anesthesiology 2001;95:1175-1181.
20. Benemof JL. Management of the difficult adult airway with special emphasis on awake tracheal intubation. Anesthesiology 1991;75:1087-1110.
21. Henderson JJ, Popat MT, Latto IP, Pearce AC. Difficult Airway Society. Difficult Airway Society guidelines for management of the unanticipated difficult intubation. Anaesthesia 2004;59:675-694.
22. Asai T, Koga K, Vaughan RS. Respiratory complications associated with tracheal intubation and extubation. Br J Anaesth 1998;80:767-775.
23. Barron FA, Ball DR, Jefferson P, Norrie J. 'Airway Alerts' How UK anaesthetists organize, document and communicate difficult airway management. Anaesthesia 2003;58:73-77.
24. Kerridge RK, Crittenden MB, Vutukuri VL. A multiple-hospital anaesthetic problem register: establishment of a regionally organized system for facilitated reporting of potentially recurring anaesthetic-related problems. Anaesth Intensive Care 2001;29:106.
25. Rosenblatt WH, Wagner PJ, Ovassapian A, Kain ZN. Practice patterns in managing the difficult airway by anesthesiologists in the United States. Anesth Analg 1998;87:153-157.
Figure 2
Laryngeal Mask Airways.
A) Classic LMATM with different sizes.
B) LMA FastrackTM.
C) LMA ProSealTM (from www.lmana.com).

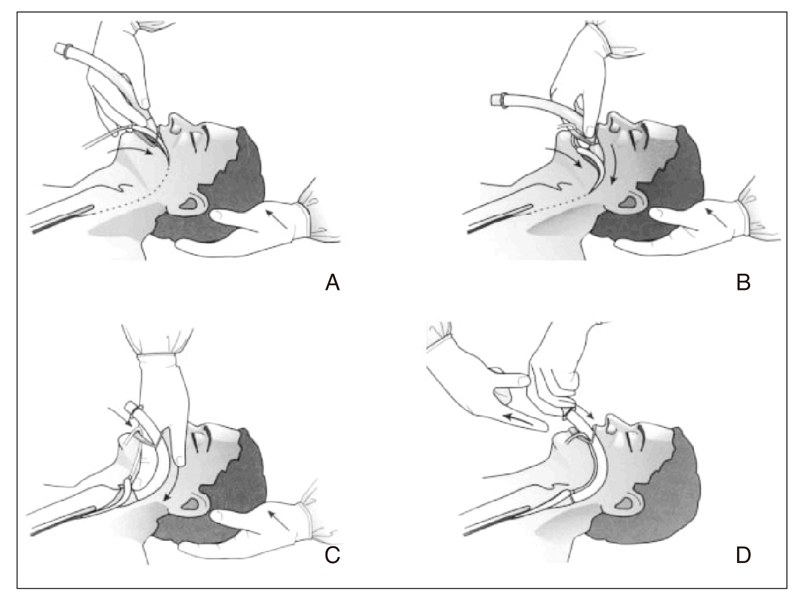
Figure 3
Insertion of the laryngeal mask airway (LMA). A) The tip of the cuff is pressed upward against the hard palate by the index finger while the middle finger opens the mouth. B) The LMA is pressed backward in a smooth movement. Notice that the nondominant hand is used to extend the head. C) The LMA is advanced until definite resistance is felt. D) Before the index finger is removed, the nondominant hand presses down on the LMA to prevent dislodgment during removal of the index finger. The cuff is subsequently inflated, and outward movement of the tube is often observed during this inflation. (from www.lmana.com)
- TOOLS
-
- Share :
-





-
METRICS

-
- 0 Crossref
- Scopus
- 1,239 View
- 9 Download
-

-
Related articles in
J Korean Med Assoc -
Antiviral Agents1998 March;41(3)
Management of matalgia1999 February;42(2)
Alopecia and Treatment1999 July;42(7)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
