



 |
 |
| J Korean Med Assoc > Volume 50(10); 2007 > Article |
Abstract
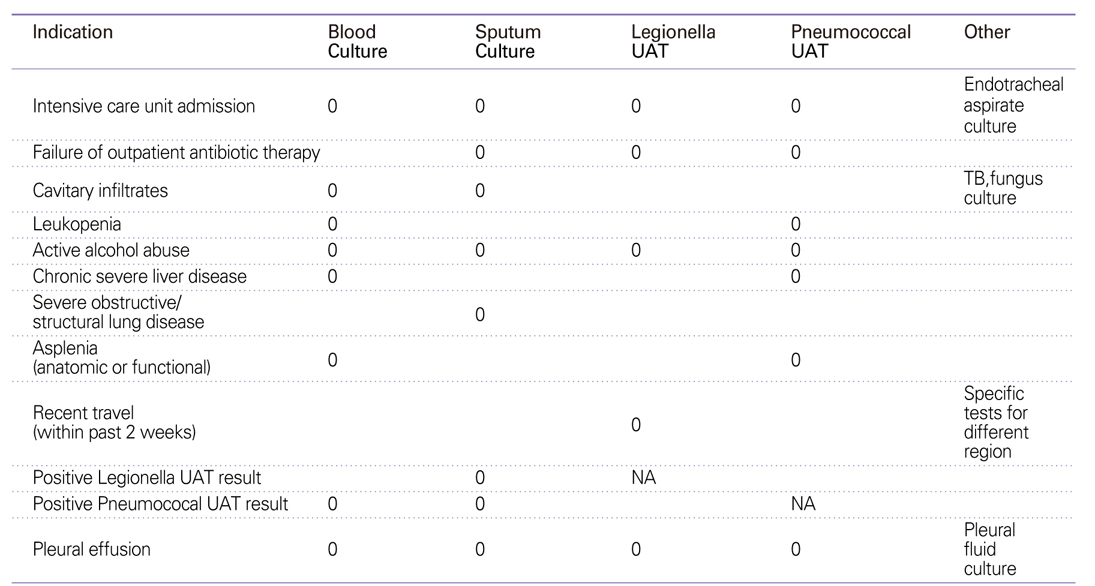
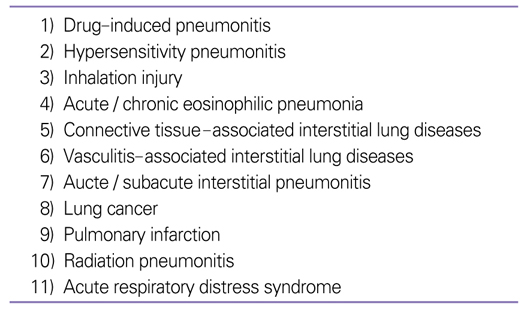
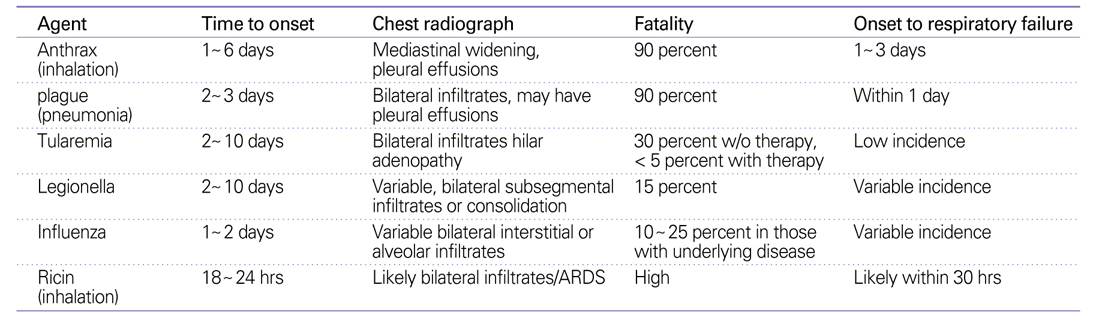
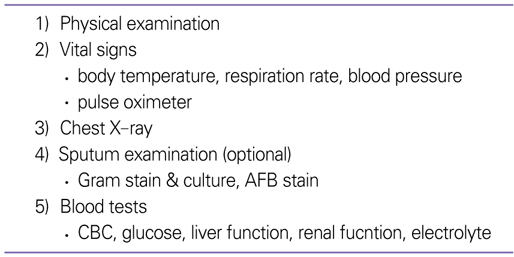
Community-acquired pneumonia (CAP) is defined as an acute infection of pulmonary parenchyma in a patient who has contracted the infection in the community. Diagnostic process includes history taking, physical examination, chest radiograph, blood tests, and microbiologic tests. Common clinical features are cough, sputum, fever, pleuritic chest pain, and dyspnea. There are systemic symptoms such as nausea, vomiting, diarrhea, and changes of mental status. The presence of an infiltrate on chest X-ray is the mainstay for the diagnosis of CAP, although exceptions are early CAP, dehydration, and neutropenia. Prevalent radiographic findings are lobar pneumonia, interstitial infiltrates, and cavitation. Performing diagnostic testing for the microbiologic etiology remains controversial particularly in outpatient settings. The tests are recommended only when pathogens that would not respond to usual empirical antibiotic regimens are suspected. However, for hospitalized patients, routine pursuit of etiologic agents should be done for all occasions. Apart from Gram stain and culture of sputum, blood culture, serologic tests, urine antigen tests, and polymerase chain reactions are being performed in hospitalized patients. Among these, the combination of a good sputum specimen for Gram stain and culture plus urinary antigen testing is most useful for the rapid diagnosis of CAP. The positivity rate of blood culture is relatively low, which makes the test less dependable. We should always consider Mycobacterium as an unpredicted cause of pulmonary infiltrates in Korea. We should also bear in mind unusual pathogens that have an epidemiologic significance or need different regimens from empirical antibiotics. These include Influenza, Legionella, community-acquired methicillin-resistant Staphylococcus aureus, and agents of bioterrorism. In conclusion, any diagnostic tests should not delay the administration of proper antibiotics. Comprehensive knowledge regarding the relevant diagnostic tests is required for the appropriate implementation of diagnostic procedures and empirical antibiotics.
References
1. Korean Academy of Tuberculosis and Respiratory Diseases. Guideline for the management of community-acquired pneumonia 2005.
2. Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean LC, Dowell SF, File TM Jr, Musher DM, Niederman MS, Toress A, Whitney CG. Infectious diseases society of america/american thoracic society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis 2007;44:S2. S27.
4. Craven DE, Palladino R, McQuillen DP. Healthcare-associated pneumonia in adults: management principles to improve outcomes. Infect Dis Clin North Am 2004;18:939.
5. Metlay JP, Fine MJ. Testing strategies in the initial management of patients with community-acquired pneumonia. Ann Intern Med 2003;138:109.
6. Metlay JP, Kapoor WN, Fine MJ. Does this patient have community-acquired pneumonia? Diagnosing pneumonia by history and physical examination JAMA 1997;278:1440.
7. Basi SK, Marrie TJ, Huang JQ, Majumdar SR. Patients admitted to hospital with suspected pneumonia and normal chest radiographs: epidemiology, microbiology, and outcomes. Am J Med 2004;117:305.
8. Syrjälä H, Broas M, Suramo I, Ojala A, Lähde s. High-resolution computed tomography for the diagnosis of community-acquired pneumonia. Clin Infect Dis 1998;27:358.
9. van der Eerden MM, Vlaspolder F, de Graaff CS, Groot T, Janson HM, Boersma WG. Value of intensive diagnostic microbiological investigation in low- and high-risk patients with community-acquired pneumonia. Eur J Clin Microbiol Infect Dis 2005;24:241.
10. Chalasani NP, Valdecanas MA, Gopal AK, Mc Gowan JE Jr, Jurado RL. Clinical utility of blood cultures in adult patients with community-acquired pneumonia without defined underlying risks. Chest 1995;108:932.
11. Musher DM, Montoya R, Wanahita A. Diagnostic value of microscopic examination of gram-stained sputum and sputum cultures in patients with bacteremic pneumococcal pneumonia. Clin Infect Dis 2004;39:165.
12. Corbo J, Friedman B, Bijur P, Gallagher EJ. Limited usefulness of initial blood cultures in community acquired pneumonia. Emerg Med J 2004;21:446.
13. Ewig S, Schlochtermeier M, Goke N, Niederman MS. Applying sputum as a diagnostic tool in pneumonia: limited yield, minimal impact on treatment decisions. Chest 2002;121:1486.
14. Reed WW, Byrd GS, Gates RH Jr, Howard RS, Weaver MJ. Sputum gram's stain in community-acquired pneumococcal pneumonia. A meta-analysis. West J Med 1996;165:197.
15. Helbig JH, Uldum SA, Bernander S, Lück PC, Wewalka G, Abraham B, Gaia V, Harrison TG. Clinical utility of urinary antigen detection for diagnosis of community-acquired, travel-associated, and nosocomial legionnaires' disease. J Clin Microbiol 2003;41:838.
16. Murdoch DR. Diagnosis of Legionella infection. Clin Infect Dis 2003;36:64.
17. Templeton KE, Scheltinga SA, van den Eeden WC, Graffelman AW, van den Broek PJ, Claas EC. Improved diagnosis of the etiology of community-acquired pneumonia with realtime polymerase chain reaction. Clin Infect Dis 2005;41:345.
18. Murdoch DR. Impact of rapid microbiological testing on the management of lower respiratory tract infection. Clin Infect Dis 2005;41:1445.
19. Fine MJ, Smith MA, Carson CA, Mutha SS, Sankey SS, Weissfeld LA, Kapoor WN. Prognosis and outcomes of patients with community-acquired pneumonia. A metaanalysis. JAMA 1996;275:134.
20. Hageman JC, Uyeki TM, Francis JS, Jernigan DB, Wheeler JG, Bridges CB, Barenkamp SJ, Sievert DM, Srinivasan A, Doherty MC, McDougal LK, Killgore GE, Lopatin UA, Coffman R, MacDonald JK, McAllister SK, Fosheim GE, Patel JB, McDonald LC. Severe community-acquired Pneumonia Due to Staphylococcus aureus 2003-2004 Influenza Season. Emerg Infect Dis 2006;12:894.
21. Mills GD, Oehley MR, Arrol B. Effectiveness of beta lactam antibiotics compared with antibiotics active against atypical pathogens in non-severe community acquired pneumonia: meta-analysis. BMJ 2005;330:456.
22. Karwa M, Currie B, Kvetan V. Bioterrorism: Preparing for the impossible or the improbable. Crit Care Med 2005;33:S75.
- TOOLS
-
- Share :
-





-
METRICS

-
- 1 Crossref
- Scopus
- 1,178 View
- 8 Download
-

-
Related articles in
J Korean Med Assoc -
Foundations of Community Mental Health1997 February;40(2)
Community Acquired Pheumonia1997 May;40(5)
Hospital Actuired Pneumonia1997 May;40(5)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
