



 |
 |
| J Korean Med Assoc > Volume 50(2); 2007 > Article |
Abstract
Multidetector computed tomography (MDCT) has recently been used as a diagnostic tool for the evaluation of coronary artery morphology and stenosis. The accuracy of MDCT has improved as the number of detectors of MDCT has increased. A 64-MDCT reliably detects significant coronary artery stenosis with a sensitivity and specificity higher than 90%. With its high negative predictive value near 100%, 64-MDCT is very practical for excluding significant coronary artery disease and avoiding unnecessary invasive coronary angiography. Furthermore, preprocedural MDCT coronary angiography is useful to provide additional information and predict the procedural outcomes particularly in patients who have chronic total occlusion and those referred for percutaneous coronary intervention. Postprocedural MDCT coronary angiography usually involves evaluation of in-stent restenosis. Recently, drug-eluting stents are widely used and has notably reduced the rate of in-stent restenosis. However, the rate of in-stent restenosis of drug-eluting stents are still 5~10%. Considering the large number of patients who receive coronary artery stents, MDCT would be clinically useful as a noninvasive tool for the reliable detection of in-stent restenosis. Even with 64-MDCT, 30~40% of stents are not evaluable because the spatial and temporal resolutions are not sufficient for the detection of in-stent restenosis. With the 64-MDCT technology, the accessibility of in-stent restenosis mainly depends on stent size and severity of metal artifact of stents. Although the current MDCT does not permit reliable detection of in-stent restenosis, MDCT can be accepted as a first-line alternative to coronary angiography for the evaluation of stents, especially those with a large diameter such as left main coronary artery stents.
References
1. Kaneda H, Saito S, Shiono T, Miyashita Y, Takahashi S, Domae H. Sixty-four-slice computed tomography-facilitated percutaneous coronary intervention for chronic total occlusion. Int J Cardiol 2007;115:130-132.
2. Yokoyama N, Yamamoto Y, Suzuki S, Suzuki M, Konno K, Kozuma K, Kaminaga T, Isshiki T. Impact of 16-slice computed tomography in percutaneous coronary intervention of chronic total occlusions. Catheter Cardiovasc Interv 2006;68:1-7.
3. Mollet NR, Hoye A, Lemos PA, Cademartiri F, Sianos G, Mc-Fadden EP, Krestin GP, Serruys PW, de Feyter PJ. Value of preprocedure multislice computed tomographic coronary angiography to predict the outcome of percutaneous recanalization of chronic total occlusions. Am J Cardiol 2005;95:240-243.
4. Van Mieghem CA, Cademartiri F, Mollet NR, Malagutti P, Valgimigli M, Meijboom WB, Pugliese F, McFadden EP, Ligthart J, Runza G, Bruining N, Smits PC, Regar E, van der Giessen WJ, Sianos G, van Domburg R, de Jaegere P, Krestin GP, Serruys PW, de Feyter PJ. Multislice spiral computed tomography for the evaluation of stent patency after left main coronary artery stenting: a comparison with conventional coronary angiography and intravascular ultrasound. Circulation 2006;114:645-653.
5. Rixe J, Achenbach S, Ropers D, Baum U, Kuettner A, Ropers U, Bautz W, Daniel WG, Anders K. Assessment of coronary artery stent restenosis by 64-slice multi-detector computed tomography. Eur Heart J 2006;27:2567-2572.
6. Funabashi N, Maeda F, Nakamura K, Suzuki K, Mita Y, Asano M, Narumi H, Kurokawa M, Komuro I. Patency of the left coronary artery by 64-slice multislice computed tomography following implantation of sirolimus-eluting stent. Int J Cardiol 2006;111:333-335.
7. Beohar N, Robbins JD, Cavanaugh BJ, Ansari AH, Yaghmai V, Carr J, Davidson CJ. Quantitative assessment of in-stent dimensions: a comparison of 64 and 16 detector multislice computed tomography to intravascular ultrasound. Catheter Cardiovasc Interv 2006;68:8-10.
8. Holmes DR Jr, Leon MB, Moses JW, Popma JJ, Cutlip D, Fitzgerald PJ, Brown C, Fischell T, Wong SC, Midei M, Snead D, Kuntz RE. Analysis of 1-year clinical outcomes in the SIRIUS trial: a randomized trial of a sirolimus-eluting stent versus a standard stent in patients at high risk for coronary restenosis. Circulation 2004;109:634-640.
9. Budoff MJ, Achenbach S, Blumenthal RS, Carr JJ, Goldin JG, Greenland P, Guerci AD, Lima JA, Rader DJ, Rubin GD, Shaw LJ, Wiegers SE. Assessment of coronary artery disease by cardiac computed tomography: a scientific statement from the American Heart Association Committee on Cardiovascular Imaging and Intervention, Council on Cardiovascular Radiology and Intervention, and Committee on Cardiac Imaging, Council on Clinical Cardiology. Circulation 2006;114:1761-1791.
10. Hoffmann U, Nagurney JT, Moselewski F, Pena A, Ferencik M, Chae CU, Cury RC, Butler J, Abbara S, Brown DF, Manini A, Nichols JH, Achenbach S, Brady TJ. Coronary multidetector computed tomography in the assessment of patients with acute chest pain. Circulation 2006;114:2251-2260.
11. Omran H, Schmidt H, Hackenbroch M, Illien S, Bernhardt P, von der Recke G, Fimmers R, Flacke S, Layer G, Pohl C, Luderitz B, Schild H, Sommer T. Silent and apparent cerebral embolism after retrograde catheterisation of the aortic valve in valvular stenosis: a prospective, randomised study. Lancet 2003;361:1241-1246.
12. Budoff MJ, Georgiou D, Brody A, Agatston AS, Kennedy J, Wolfkiel C, Stanford W, Shields P, Lewis RJ, Janowitz WR, Rich S, Brundage BH. Ultrafast computed tomography as a diagnostic modality in the detection of coronary artery disease: a multicenter study. Circulation 1996;93:898-904.
13. Stein PD, Beemath A, Kayali F, Skaf E, Sanchez J, Olson RE. Multidetector computed tomography for the diagnosis of coronary artery disease: a systematic review. Am J Med 2006;119:203-216.
14. Schuijf JD, Bax JJ, Shaw LJ, de Roos A, Lamb HJ, van der Wall EE, Wijns W. Meta-analysis of comparative diagnostic performance of magnetic resonance imaging and multislice computed tomography for noninvasive coronary angiography. Am Heart J 2006;151:404-411.
15. Gilard M, Cornily JC, Rioufol G, Finet G, Pennec PY, Mansourati J, Blanc JJ, Boschat J. Noninvasive assessment of left main coronary stent patency with 16-slice computed tomography. Am J Cardiol 2005;95:110-112.
Figure 1
Total occlusion of left anterior descending artery. Coronary angiography shows total occlusion of the proximal left anterior descending artery (A). The 3-dimensional volume rendered CT image shows calcification along the occluded segments (B). The curved multiplanar image excellently shows not only the extent of total occlusion but also occluding mixed plaques with calcification and fibrous components (C)
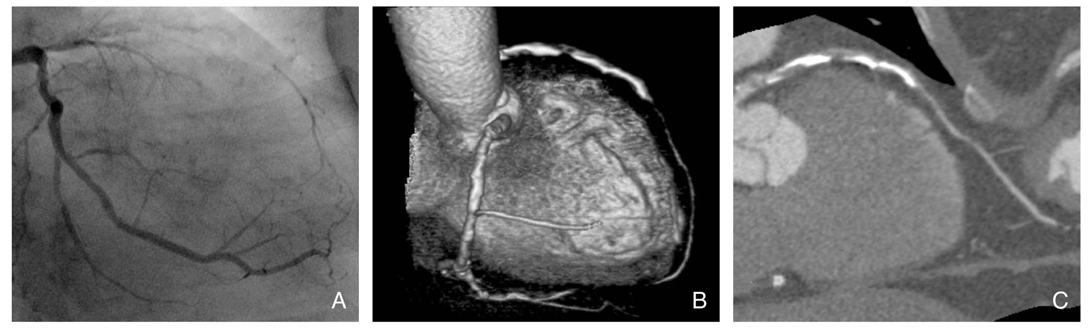
Figure 2
Visualization of patent stent lumen and in-stent restenosis with coronary MDCT angiography. 64-MDCT shows a patent drug-eluting stent in the proximal left anterior descending artery (A). In a different patient, 64-MDCT shows in-stent restenosis in the distal right coronary artery (B). which reveals low-attenuated intra-luminal density
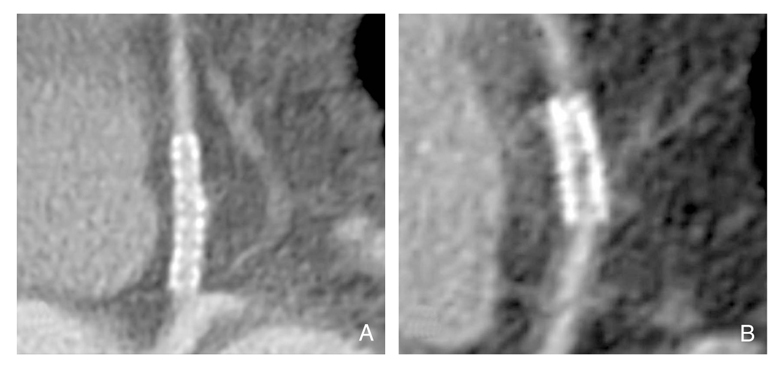
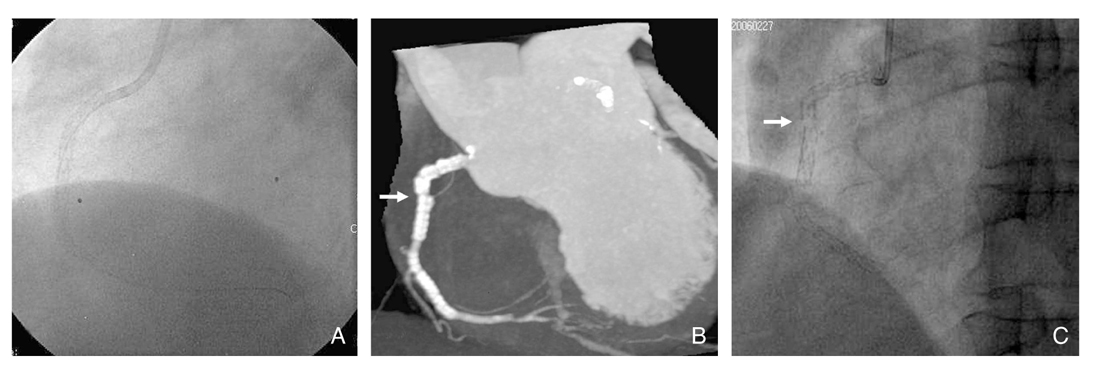
Figure 3
Coronary intervention in chronic total occlusion. A total occlusion is noted from the mid to distal left anterior descending artery (A). The total occlusion is passed by a guide wire with retrograde fashion through a collateral pathway (B). Stenting through the occluded segment is successfully performed (C)
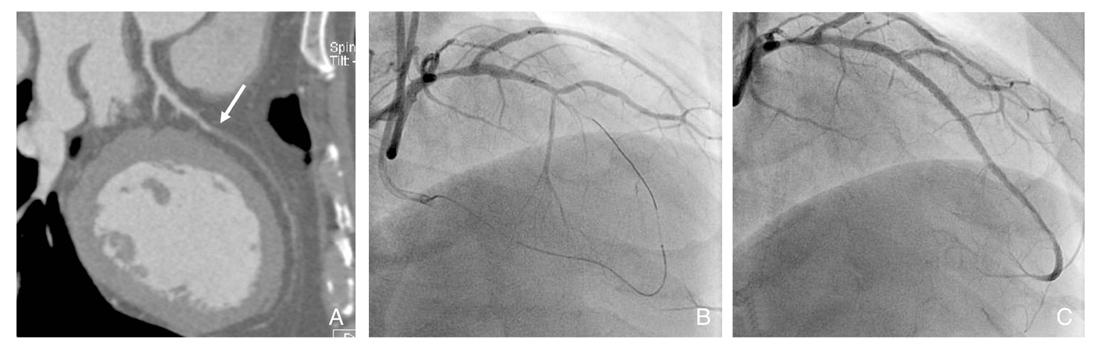
Figure 4
In-stent restenosis in distal right coronary artery. A curved multiplanar MDCT angiography shows a stent at the distal right coronary artery, which was wrongly interpreted as patent (A). The coronary angiogram shows significant in-stent restenosis (B)
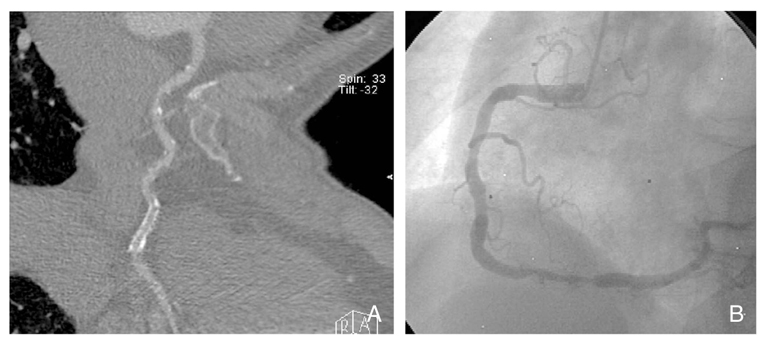
Figure 5
CT image reconstruction affecting evaluation of coronary stents. The image that is reconstructed with a sharpkernel for evaluation of stents (B) is superior in evaluation of in-stent lumen to the image that is reconstructed with a soft-kernel for angiographic images (A)
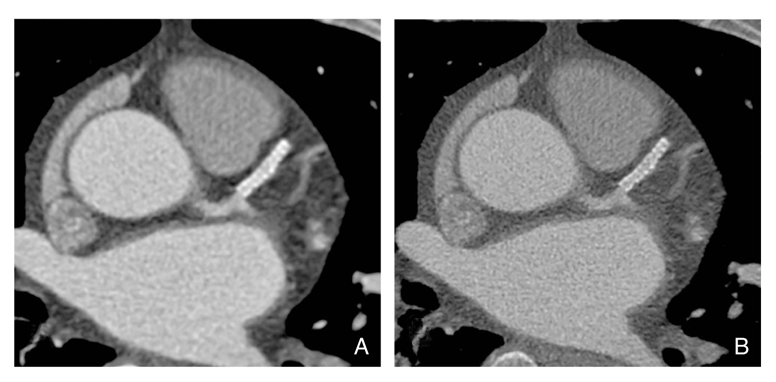
Figure 6
In-stent restenosis and peri-stent small aneurysms of drug-eluting stent. The 64-MDCT image shows in-stent restenosis (arrow) at the distal part with eccentric neointimal proliferation as a low density (A). The coronary angiogram confirms in-stent restenosis (B). Small peri-stent aneurysms are noted (arrowheads in A and B)
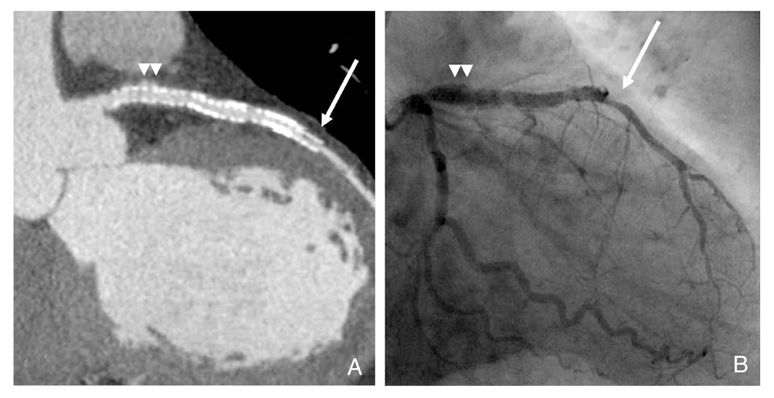
Figure 7
Stenting of left main artery and bifurcation. The stents in the left main and bifurcation shows low luminal density, which is suggesting significant restenosis (A). The coronary angiogram confirms significant restenosis of the stents (B)

Figure 8
Stent fracture. A stent was inserted at the proximal right coronary artery. In 2-year follow-up, a stent was inserted at the distal right coronary artery, where significant stenosis was newly developed (A). In 4-year follow up, stent fracture at the proximal segment is noted, which is well depicted in MDCT (arrow in B) and coronary angiography (arrow in C)
- TOOLS
-
- Share :
-





-
METRICS

-
- 0 Crossref
- Scopus
- 1,108 View
- 5 Download
-

-
Related articles in
J Korean Med Assoc -
Pharmacologic Therapy of Coronary Artery Disease2001 May;44(5)
Percutaneous Coronary Intervention2002 May;45(5)
Diagnosis of Coronary Artery Disease2004 August;47(8)
Medical Management of Coronary Artery Disease2004 August;47(8)
Percutaneous Coronary Intervention for Coronary Artery Disease2004 August;47(8)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
