



 |
 |
| J Korean Med Assoc > Volume 50(1); 2007 > Article |
Abstract
Deep vein thrombosis (DVT) is a common disease; however, it can result in significant disabilities from pulmonary embolism and postphlebitic syndrome, especially when the iliofemoral vein is involved. Although anticoagulation can prevent thrombus propagation and recurrent venous thrombosis, it cannot dissolve the occluding thrombus or reduce venous outflow obstruction, leaving the patients suffering from postphlebitic syndrome. Catheter-directed thrombolysis, with direct delivery of a concentrated lytic agent into the clot, has been proposed as an alternative therapy to anticoagulation. Recent studies have demonstrated that early clot lysis through this technique rapidly restores venous patency, more effectively preserves valvular function, and reduces a risk of postphlebitic syndrome. To decrease clot burden, duration of treatment, and bleeding complications, mechanical thrombectomy may work synergistically with catheter-directed thrombolysis. After clot removal through those therapies, balloon angioplasty and stent placement are needed in patients with venous stricture (eg, iliac vein compression syndrome). Short- and long-term outcomes of stenting in iliofemoral DVT appear to be favorable. When used in conjunction with each other and anticoagulation, these minimally invasive endovascular techniques allow a better resolution of venous clot burden and have the potential to lead to improved long-term outcomes in patients with DVT. This review introduces endovascular treatments of acute DVT in the lower extremities performed in the interventional radiology section.
References
1. Anderson FA, Wheeler HB, Goldberg RJ, Hosmer DW, Patwardhan NA, Jovanovic B, Forcier A, Dalen JE. A populationbased perspective of the hospital incidence and case-fatality rates of deep vein thrombosis and pulmonary embolism. The Worcester DVT Study. Arch Intern Med 1991;151:933-938.
2. Haines ST. Venous thromboembolism: pathophysiology and clinical presentation. Am J Health Syst Pharm 2003;60:S 7. S3-S5.
3. O'Donnell TF Jr, Browse NL, Burnand KG, Thomas ML. The socioeconomic effects of an iliofemoral venous thrombosis. J Surg Res 1977;22:483-488.
4. Akesson H, Brudin L, Dahlstrom JA, Eklof B, Ohlin P, Plate G. Venous function assessed during a 5 year period after acute ilio-femoral venous thrombosis treated with anticoagulation. Eur J Vasc Surg 1990;4:43-48.
5. Augustinos P, Ouriel K. Invasive approaches to treatment of venous thromboembolism. Circulation 2004;110:9 S 1. I27-I34.
6. Blum A, Roche E. Endovascular management of acute deep vein thrombosis. Am J Med 2005;118:S 8A. 31-36.
7. Delis KT, Bountouroglou D, Mansfield AO. Venous claudication in iliofemoral thrombosis: long-term effects on venous hemodynamics, clinical status, and quality of life. Ann Surg 2004;239:118-126.
8. Sherry S. Thrombolytic therapy for deep venous thrombosis. Semin Intervent Radiol 1985;4:331-337.
9. Krupski WC, Bass A, Dilley RB, Bernstein EF, Otis SM. Propagation of deep venous thrombosis identified by duplex ultrasonography. J Vasc Surg 1990;12:467-474. discussion 474-475.
10. Arnesen H, Hoiseth A, Ly B. Streptokinase of heparin in the treatment of deep vein thrombosis. Follow-up results of a prospective study. Acta Med Scand 1982;211:65-68.
11. Semba CP, Razavi MK, Kee ST, Sze DY, Dake MD. Thrombolysis for lower extremity deep venous thrombosis. Tech Vasc Interv Radiol 2004;7:68-78.
12. Hood DB, Alexander JQ. Endovascular management of iliofemoral venous occlusive disease. Surg Clin North Am 2004;84:1381-1396. viii.
13. Mewissen MW, Seabrook GR, Meissner MH, Cynamon J, Labropoulos N, Haughton SH. Catheter-directed thrombolysis for lower extremity deep venous thrombosis: report of a national multicenter registry. Radiology 1999;211:39-49.
14. Semba CP, Dake MD. Iliofemoral deep venous thrombosis: aggressive therapy with catheter-directed thrombolysis. Radiology 1994;191:487-494.
15. Bjarnason H, Kruse JR, Asinger DA, Nazarian GK, Dietz CA Jr, Caldwell MD, key NS, Hirsch AT, Hunter DW. Iliofemoral deep venous thrombosis: safety and efficacy outcome during 5 years of catheter-directed thrombolytic therapy. J Vasc Interv Radiol 1997;8:405-418.
16. Tarry WC, Makhoul RG, Tisnado J, Posner MP, Sobel M, Lee HM. Catheter-directed thrombolysis following vena cava filtration for severe deep venous thrombosis. Ann Vasc Surg 1994;8:583-590.
17. Comerota AJ, Throm RC, Mathias SD, Haughton S, Mewissen M. Catheter-directed thrombolysis for iliofemoral deep venous thrombosis improves health-related quality of life. J Vasc Surg 2000;32:130-137.
18. Murphy KD. Mechanical thrombectomy for DVT. Tech Vasc Interv Radiol 2004;7:79-85.
19. Kim HS, Patra A, Paxton BE, Khan J, Streiff MB. Adjunctive percutaneous mechanical thrombectomy for lower-extremity deep vein thrombosis: clinical and economic outcomes. J Vasc Interv Radiol 2006;17:1099-1104.
20. Lee KH, Han H, Lee KJ, Yoon CS, Kim SH, Won JY, Lee do Y. Mechanical thrombectomy of acute iliofemoral deep vein thrombosis with use of an Arrow-Trerotola percutaneous thrombectomy device. J Vasc Interv Radiol 2006;17:487-495.
21. Frisoli JK, Sze D. Mechanical thrombectomy for the treatment of lower extremity deep vein thrombosis. Tech Vasc Interv Radiol 2003;6:49-52.
22. Kwak HS, Han YM, Lee YS, Jin GY, Chung GH. Stents in common iliac vein obstruction with acute ipsilateral deep venous thrombosis: early and late results. J Vasc Interv Radiol 2005;16:815-822.
23. Mickley V, Schwagierek R, Rilinger N, Gorich J, Sunder-Plassmann L. Left iliac venous thrombosis caused by venous spur: treatment with thrombectomy and stent implantation. J Vasc Surg 1998;28:492-497.
24. Patel NH, Stookey KR, Ketcham DB, Cragg AH. Endovascular management of acute extensive iliofemoral deep venous thrombosis caused by May-Thurner syndrome. J Vasc Interv Radiol 2000;11:1297-1302.
25. O'Sullivan GJ, Semba CP, Bittner CA, Kee ST, Razavi MK, Sze DY, Dake MD. Endovascular management of iliac vein compression (May-Thurner) syndrome. J Vasc Interv Radiol 2000;11:823-836.
Figure 1
Multi-side hole infusion catheter. Thrombolytic drug are infused through multiple side holes of infusion catheter
Figure 2
A 59-year-old man with acute deep vein thrombosis
(A) Ascending venography shows extensive thrombus in left iliofemoral vein
(B) Multi- side- hole infusion catheter is embedded within thrombosed segment and urokinase is infused for 24 hours
(C) After catheter directed thrombolysis, patency of the iliofemoral vein is restored
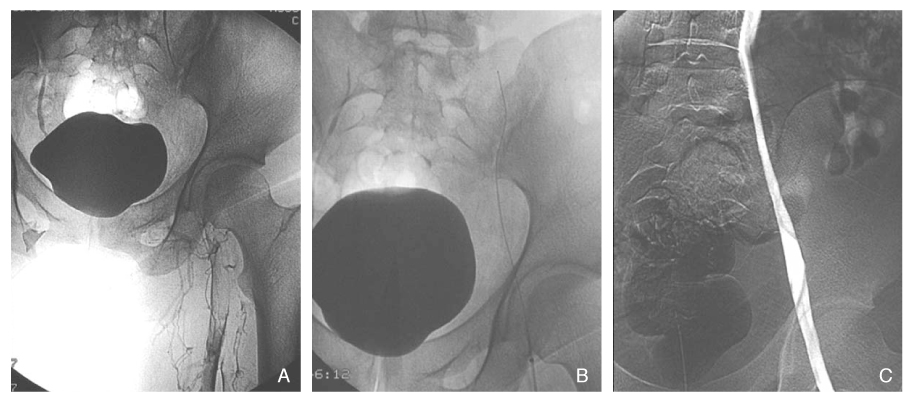
Figure 3
A 44-year-old woman with iliac compression syndrome
(A) CT scan shows compressed left iliac vein (arrow) between right common iliac artery and vertebra body
(B) Venography shows extrinsic compression of proximal left common iliac vein and collaterals to contralateral iliac vein
(C) After placement of self expandable stent in left common iliac vein, venography shows widely patent left common iliac vein

- TOOLS
-
- Share :
-





-
METRICS

-
- 2 Crossref
- Scopus
- 1,415 View
- 7 Download
-

-
Related articles in
J Korean Med Assoc -
Interventional Radiology : Interventional Neuroradiology2002 May;45(5)
Interventional Treatment of Bleeding2002 May;45(5)
Interventional Treatment for Gastrointestinal Tract2002 May;45(5)
Interventional Radiology for the Urogenital System2002 May;45(5)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
