



 |
 |
| J Korean Med Assoc > Volume 49(12); 2006 > Article |
Abstract
Minimally invasive surgery (MIS) has been applied to nearly all fields of surgery due to its advantages like reduced morbidity, a better cosmetic outcome and early recovery. The recent advances in its technique have allowed us to use modified MIS technique in the field of kidney transplantation. From January 2004 to Mar 2006, minimally invasive kidney transplantation was carried out in 20 patients. Many clinical variables were compared to the conventional method. The operative procedure began with 7~8cm skin incision. A laparoscopic balloon dissector was used to create the retroperitoneal space for the placement of the grafted kidney. Vascular anastomosis and ureteroneocystostomy were performed under direct vision and with video-assisted TV monitoring. The average length of the wound was 7.8 cm and it was placed below the belt line. The average operating time was 186 minutes. Less analgesic was given compared to conventional methods. There was one postoperative complication, a mild lymphocele. All patients showed normalized serum creatinine levels within 4 days. All grafted kidneys showed normal findings on the postoperative ultrasound and renal scans. Minimally invasive video-assisted kidney transplantation is technically feasible and may offer benefits in terms of better cosmetic outcomes, less pain and quicker recuperation than conventional kidney transplantation.
References
1. Kojima M, Konishi F, Okada M, Nagai H. Laparoscopic colectomy versus open colectomy for colorectal carcinoma: a retrospective analysis of patients followed up for at least 4 years. Surg Today 2004;34:1020-1024.
2. Patankar SK, Larach SW, Ferrara A, Williamson PR, Gallagher JT, Narayanan S, et al. Prospective comparison of laparoscopic vs. open resections for colorectal adenocarcinoma over a ten-year period. Dis Colon Rectum 2003;46:601-611.
3. Huscher CG, Mingoli A, Sgarzini G, Sansonetti A, Di Paola M, Ponzano C, et al. Laparoscopic versus open subtotal gastrectomy for distal gastric cancer: five-year results of a randomized prospective trial. Ann Surg 2005;241:232-237.
4. Greenstein Marc A., Harkaway Richard, Badosa Francisco, Ginsberg Phillip, Yang Shuin-Lin. Minimal incision living donor nephrectomy compared to the hand-assisted laparoscopic living donor nephrectomy. World J Urol 2003;20:356-359.
5. Kurian Marina S., Gagner Michel, Murakami Yasusuke, Andrei Valeriu, Jossart Gregg, Schwartz Myron. Hand-assisted Laparoscopic Donor Hepatectomy for Living Related Transplantation in the Porcine Model. Surg Laparosc Endosc Percutan Tech 2002;12:232-237.
6. Nanni G, Tondolo V, Citterio F, Romagnoli J, Borgetti M, Castagneto M, et al. Comparison of Oblique Versus Hockey-Stick Surgical Incision for Kidney Transplantation. Transplantation Proceedings 2005;37:2479-2481.
7. Aigner C, Jaksch P, Seebacher G, Neuhauser P, Marta G, Klepetko W, et al. Single running suture the new standard technique for bronchial anastomoses in lung transplantation. Eur J Cardiothorac Surg 2003;23:488-493.
8. Van Velthoven RF, Ahlering TE, Peltier A, Skarecky DW, Clayman RV. Technique for laparoscopic running urethrovesical anastomosis:the single knot method. Urology 2003;61:699-702.
9. Demirci D, Gulmez I, Ekmekcioglu O, Karacagil M. Retroperitoneoscopic ureterolithotomy for the treatment of ureteral calculi. Urol Int 2004;73:234-237.
10. Takada M, Ichihara T, Toyama H, Suzuki Y, Kuroda Y. Retroperitoneoscopic laparoscopic distal pancreatectomy with spleen salvage. Hepatogastroenterology 2004;51:925-927.
11. Francis DM, Walker RG, Becker GJ, Millar RJ, Powell HR, Kincaid-Smith PS, et al. Kidney transplantation from living related donors: a 19-year experience. Med J Aust 1993;158:244-247.
12. Matas AJ, Gillingham KJ, Elick BA, Dunn DL, Gruessner RW, Najarian JS, et al. Risk factors for prolonged hospitalization after kidney transplants. Clin Transplant 1997;11:259-264.
Figure 1
(A) The location and course of the external iliac vessels (thick arrow) and the contour of the urinary bladder (thin arrow) were marked preoperatively using ultrasound
(B) A 7~8 cm incision was made from the imaginary line of the external iliac vessels to anterolateral part of bladder

Figure 2
(A) Illustration of the making of retroperitoneal space by balloon dissector. 20~25 ml of room air was insufflated to the balloon (black arrow head) per each compressing of the pump (thick black arrow)
(B) The telescope was inserted through the trocar of the balloon dissector and we investigated whether the space was large enough or if any complications such as bleeding or the perforation of peritoneum existed
(C) For the approach to the retroperitoneal area, the aponeurotic confluence of the three abdominal muscles, just lateral to the rectus muscle, was opened about 2cm
(D) A laparoscopic balloon dissector was inserted into the retroperitoneal area and 250~ 300ml of room air was insufflated to make a retroperitoneal space for the placement of the grafted kidney
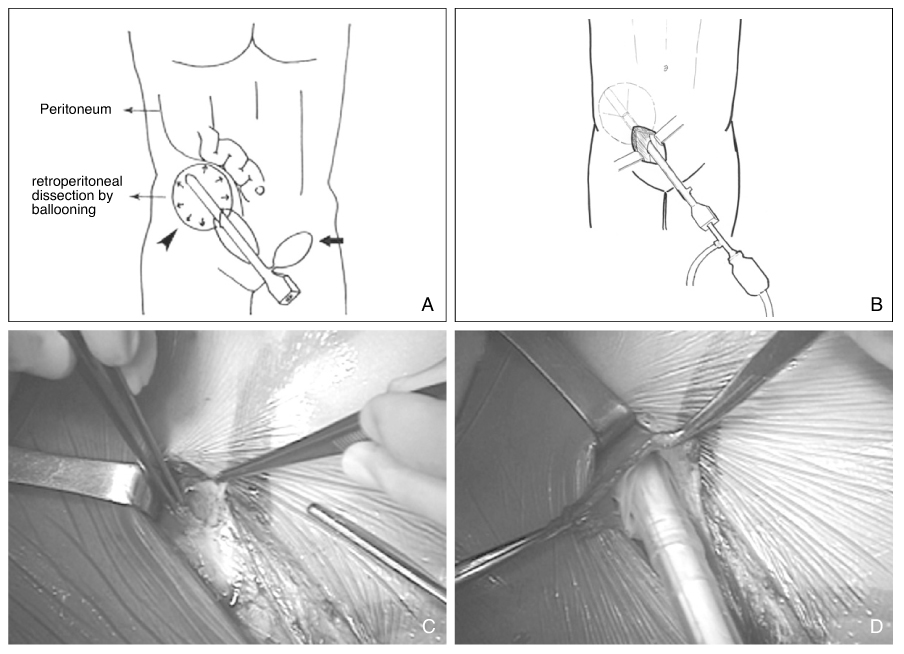
Figure 3
Illustration of the lifting of the external iliac vessels. Nearly all external iliac vessels were dissected as long as possible within the skin incision and lifted up to the level of skin to facilitate the vascular anastomosis
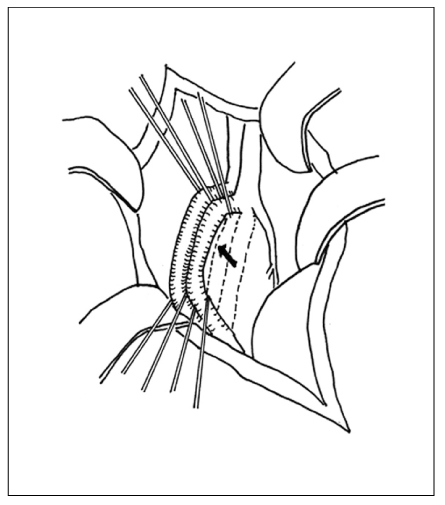
Figure 4
(A) Illustration of the retractor and video-assisted TV monitoring
(B) The kidney was placed just above the skin incision. Surgical retractor made the better operative fields with the help of specially designed blades (thin black arrow). Laparoscope was useful for the visualizing and the illumination of the operative fields that was not exposed well to the assistant surgeon located the opposite side (thin white arrow). In this figure, the left side of venous anastomosis is being performed and assistant surgeon (thick black arrow) is helping the operator (thick white arrow) seeing the TV-monitor located at the left side of the patients

Figure 5
The grafted kidney was placed into the retroperitonealspace after the identification of a sufficient urine output. A ureter with good segmental contraction and urination is seen (black arrow)
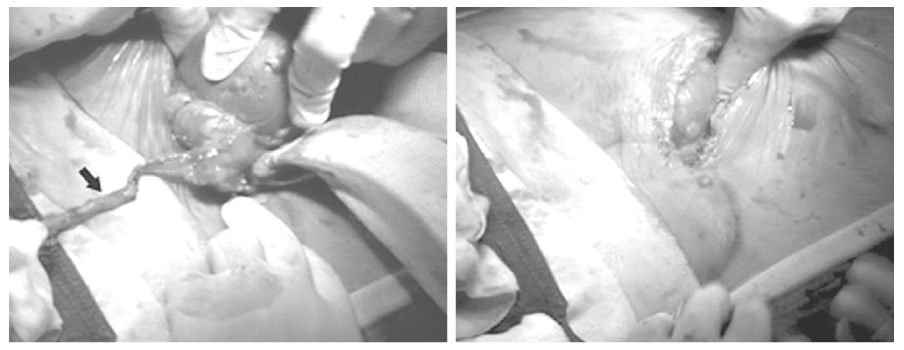
Figure 6
Comparison of the cosmetic outcomes
MIVAKT=minimal invasive video assisted kidney transplantation, CKT=conventional kidney transplantation
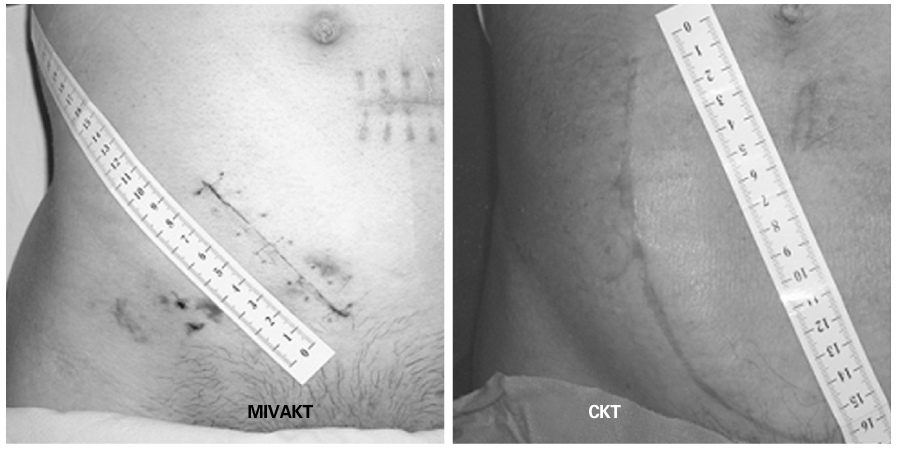
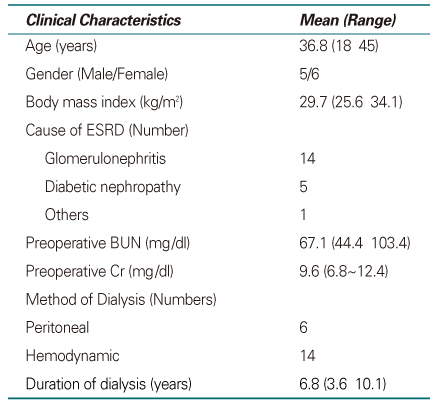
Table 2
Results of MIVAKT Mean value (range)
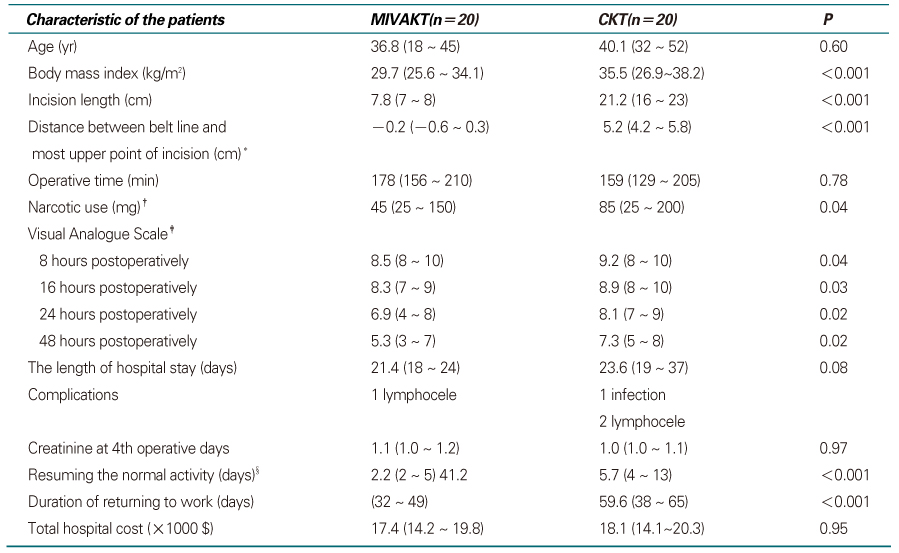
MIVKT=minimal invasive video-assisted kidney transplantation. CKT=conventional kidney transplantation
*A minus means that the most upper point of the incision is located below the belt line and a positive means it is located above the belt line
†Pethidine hydrochloride was used for analgesic
‡0: no pain, 10: maximal pain
§Normal activity includes washing, dressing, brushing of the teeth, making up, using the bathroom, eating, etc.
- TOOLS
-
- Share :
-





-
METRICS

-
- 0 Crossref
- Scopus
- 1,007 View
- 2 Download
-

-
Related articles in
J Korean Med Assoc -
Living Donor Liver Transplantation1998 October;41(10)
Minimally Invasive Surgery for Gastric Cancer2000 January;43(1)
Minimally Invasive Surgery in Hepato-Biliary-Pancreatic Disease2003 August;46(8)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
