






 |
 |
| J Korean Med Assoc > Volume 49(10); 2006 > Article |
Abstract
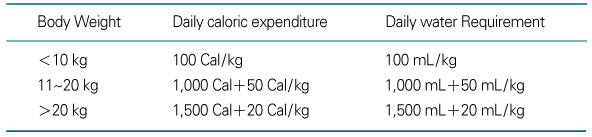
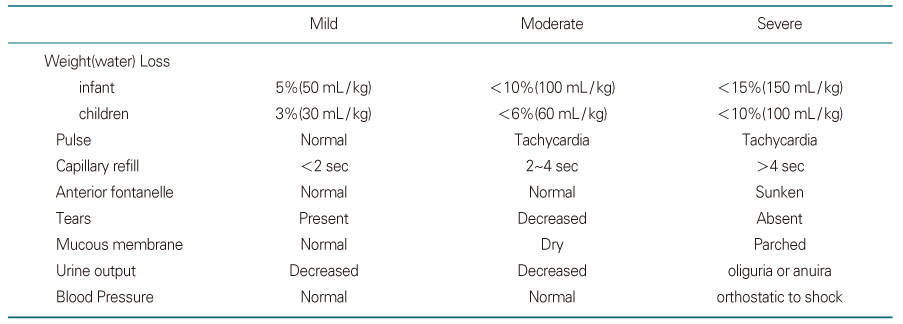
The administration of adequate fluid to the severely dehydrated patients takes precedence over all other treatment regardless of the underlying disease. Although the understanding of pathogenesis and the appropriate management of water, electrolytes, and acid-base disturbance are emphasized in medical education, many physicians are not very confident in treating the patients with those disturbances. The first thing that should be remembered in fluid therapy is how much of water and sodium is required to the patients-in other words, how much water with what concentration of sodium should be given to the patients. Water deficit can be estimated by assessing the severity of dehydration, while the sodium deficit from the types of dehydration, that is, the plasma sodium concentration of the patients. This review will summarize the principles of how to choose and give the adequate fluid according to the severity and the types of dehydration.
References
1. Greenbaum LA. In: Behrman RE, Kliegman RM, Jenson HB, editor. Pathophysiology of body fluids and fluid therapy. Nelson Textbook of Pediatrics 2003;17th ed. Philadelphia: WB Saunders. 191-252.
2. Holiday MA, Segar WE. The maintenance need for water in parenteral fluid therapy. Pediatrics 1957;19:823-832.
3. Moritz ML, Ayus JC. Prevention of hospital acquired hyponatremia; a case for using isotonic saline in maintenance therapy. Pediatrics 2003;111:227-230.
4. Kaneko K, Shimojima T, Kaneko K. Risk of exacerbation of hyponatremia with standard maintenance fluid regimens. Ped Nephrol 2004;19:1185-1186.
5. Holliday MA, Friedman AL, Wassner SJ. Extracellular fluid restoration in dehydration: a critique of rapid versus slow. Pediatr Nephrol 1999;13:292-297.
6. AAP Provisional Committee on Quality Improvement, Subcommittee on Acute Gastroenteritis. Practice parameter: the management of acute gastroenteritis in young children. Pediatrics 1996;97:424-435.
7. Arieff AI, Ayus JC, Fraser CL. Hyponatremia and death or permanent brain damage in healthy children. BMJ 1992;304:1218-1222.
8. Laureno R, Karp BI. Myelinolysis after correction of hyponatremia. Ann Intern Med 1997;126:57-62.
9. Lein YH, Shapiro JI, Chan L. Effects of hypernatremia on organic brain osmoles. J Clin Invest 1990;85:1427-1435.
10. Thaper N, Sanderson IR. Diarrhea in children; an interface between developing and developed children. Lancet 2004;363:641-653.
11. International Study Group on Reduced-Osmolarity ORS solutions. Multicentre evaluation of reduced-osmolarity oral rehydration salts solution. Lancet 1995;345:282-285.
12. Thillanagayam AV, Hunt JB, Farthing MJ. Enhancing clinical efficacy of oral rehydration therapy; is low osmolality the key? Gastroenterol 1998;114:197-210.
- TOOLS
-
- Share :
-





-
METRICS

-
- 0 Crossref
- Scopus
- 1,099 View
- 0 Download
-

-
Related articles in
J Korean Med Assoc -
Principles and Precautions of Drug Therapy in Children1998 May;41(5)
Current Trends and Prospect of Cell Therapy using Hematopoietic Stem Cells2004 October;47(10)
Growth Hormone Therapy in Short Stature Children2008 September;51(9)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
