



 |
 |
| J Korean Med Assoc > Volume 49(10); 2006 > Article |
Abstract
There are three groups of patients with constipating symptoms; those with obstructed defecation, slow transit constipation, or both. The treatment of obstructed defecation (pelvic outlet obstruction) is often challenging because the underlying disorders are diverse with a wide range of and clinical symptoms. The underlying anatomical and pathophysiological changes in patients with obstructed defecation are complex and often poorly understood. As a consequence, many medical, surgical, and behavioral approaches have been described, with no single panacea. For successful outcomes, preoperative physiologic testing is mandatory to differentiate between obstructed defecation caused by pelvic outlet obstruction and slow transit constipation. Obstructed defecatory disorders can distress patients both socially and psychologically and greatly impair their quality of life. For the great majority of patients, dietary adjustment with an increased fiber and liquid supplement can resolve the symptoms. The surgical approach depends upon the etiology, severity of symptoms, and operative risks. In a small group of patients with a rectocele or a third degree sigmoidocele, surgical intervention yields a high success rate. Division or resection of the puborectalis muscle is not recommended. In patients with a mixed pattern of slow transit colon and pelvic outlet obstruction, surgical intervention alone is often not successful; these patients can experience better outcomes by conservative treatment of pelvic outlet obstruction, followed by a colectomy. Stapled transanal rectal resection has recently become a recommended surgical procedure for obstructed defecation syndrome. One problem when using a transanal stapling device for rectal surgery is the potential damage to the structures located in front of the anterior rectal wall. The laparoscopic approach can shorten the hospital stay with good outcomes and is well tolerated in elderly patients with rectal prolapse. Despite the progress in modern surgery, the choice of the surgical procedure of pelvic outlet obstruction is still controversial. Preoperative counseling of all patients undergoing surgery is of extreme importance, in particular to explain the evolving nature of pelvic floor dysfunction and the possible need for further reconstructive surgery. To identify patients who will benefit from surgery for obstructed defecation, a careful selection of candidate patients remains the crucial issue in the diagnostic assessment. Surgical intervention should be limited only to the patients with identifiable, surgically correctable causes of outlet obstruction. This review gives an overview of surgical treatment options in patients with obstructed defecation.
References
1. Lane WA. Result of the operative treatment of chronic constipation. BMJ 1908;1:1126-1130.
2. Kuijpers JHC. Application of the colorectal laboratory in diagnosis and treatment of functional constipation. Dis Colon Rectum 1990;33:35-39.
3. Jo JS, Park UC. Diagnostic usefulness of anorectal physiologic investigation in patients with chronic constipation. Korean J Gastroenterol 1998;31:319-334.
4. Ogunbiyi OA, Fleshman JW. Obstructed defecation: definitions and management options. Semin Colon Rectal Surg 1996;7:149-159.
5. Park UC, Choi SK, Piccirillo MF, Verzaro R, Wexner SD. Patterns of anismus and the relation to biofeedback therapy. Dis Colon Rectum 1996;39:768.
6. Kim SK, Park UC. Rectocele : Anorectal physiologic characteristics and their clinical significances. J Korean Soc Coloproctol 1996;12:19-30.
7. Karlbom U, Graf W, Nilsson S. Does surgical repair of a rectocele improve rectal emptying? Dis Colon Rectum 1996;39:1296-1302.
8. Christiansen J, Zhu BW, Rasmussen O, et al. Internal rectal intussusception: Result of surgical repair. Dis Colon Rectum 1992;35:1026-1029.
9. Fleshman JW, Kodner IJ, Fry RD. Internal intussusception of the rectum: a changing perspective. Neth J Surg 1989;41:145-148.
10. Jorge JMN, Yang YR, Wexner SD. Incidence and clinical significance of sigmoidoceles as determined by a new classification system. Dis Colon Rectum 1994;37:1112-1117.
11. Yoshioka K, Keighley MRB. Anorectal myectomy for outlet obstruction. Br J Surg 1987;74:373-376.
12. Yoshioka K, Keighley MRB. Randomized trial comparing anorectal myectomy and controlled anal dilatation for outlet obstruction. Br J Surg 1987;74:1125-1128.
13. Guillemot F, Leroi H, Lone YC, Rousseau CG, Lamblin MD, Cortot A. Action of in situ nitroglycerin on upper anal canal pressure of patients with terminal constipation: a pilot study. Dis Colon Rectum 1993;36:372-376.
14. Lubowski DZ, King DW. Obstructed defecation: current status of pathophysiology and management. Aust N Z J Surg 1995;65:87-92.
15. Park UC, Baik HK, Kim BG, Cho JS. Anal achalasia: Physiologic characteristics and their clinical significance. Collegium Internationale Chirurgiae Digestivae 1996;549.
16. Park CJ. A clinical review of the rectocele. J Korean Soc Coloproctol 1995;11:115-121.
17. Ommer A, Kohler A, Athanasiadis S. Results of transperineal levator-plasty in treatment of symptomatic rectocele. Chirurg 1998;09. 69:966-972.
18. Lechaux JP, Lechaux D, Bataille P, Bars I. Transperineal repair of rectocele with prosthetic mesh. A prospective study. Ann Chir 2004;129:211-217.
19. Ayav A, Bresler L, Brunaud L, Boissel P. Long-term results of transanal repair of rectocele using linear stapler. Dis Colon Rectum 2004;47:889-894.
20. Altomare DF, Rinaldi M, Veglia A, Petrolino M, De Fazio M, Sallustio P. Combined perineal and endorectal repair of rectocele by circular stapler: a novel surgical technique. Dis Colon Rectum 2002;45:1549-1552.
21. Baessler K, Stanton SL. Sacrocolpopexy for vault prolapse and rectocele: do concomitant Burch colposuspension and perineal mesh detachment affect the outcome. Am J Obstet Gynecol 2005;192:1067-1072.
22. Petersen S, Hellmich G, Schuster A, Lehmann D, Albert W, Ludwig K. Stapled transanal rectal resection under laparoscopic surveillance for rectocele and concomitant enterocele. Dis Colon Rectum 2006;49:685-689.
23. Longo A. Stapled anopexy and stapled hemorrhoidectomy: two opposite concepts and procedures. Dis Colon Rectum 2002;45:571-572.
24. Pescatori M, Boffi F, Russo A, Zbar AP. Complications and recurrence after excision of rectal internal mucosal prolapse for obstructed defaecation. Int J Colorectal Dis 2006;21:160-165.
25. Tsiaoussis J, Chrysos E, Athanasakis E, Pechlivanides G, Tzortzinis A, Zoras O, Xynos E. Rectoanal intussusception: presentation of the disorder and late results of resection rectopexy. Dis Colon Rectum 2005;48:838-844.
26. Abbas SM, Bissett IP, Neill ME, Macmillan AK, Milne D, Parry BR. Long-term results of the anterior Delorme's operation in the management of symptomatic rectocele. Dis Colon Rectum 2005;48:317-322.
27. D'Hoore A, Cadoni R, Penninckx F. Long-term outcome of laparoscopic ventral rectopexy for total rectal prolapse. Br J Surg 2004;91:1500-1505.
28. Gadonneix P, Ercoli A, Salet-Lizee D, Cotelle O, Bolner B, Villet R, et al. Laparoscopic sacrocolpopexy with two separate meshes along the anterior and posterior vaginal walls for multicompartment pelvic organ prolapse. J Am Assoc Gynecol Laparosc 2004;11:29-35.
29. Fenner DE. Diagnosis and assessment of sigmoidoceles. Am J Obstet Gynecol 1996;175:1438-1441.
30. Farrell SA. Vaginal repair of a sigmoidocele. Int Urogynecol J Pelvic Floor Dysfunct 2000;11:325-327.
31. Martelli H, Devroede G, Arhan P, Duguay C. The mechanism of idiopathic constipation: outlet obstruction. Gastroenterology 1978;75:623-631.
32. Lysy J, Israeli E, Levy S, Rozentzweig G, Strauss-Liviatan N, Goldin E. Chemical sphincterotomy Long-Term Results of "Chemical Sphincterotomy" for Chronic Anal Fissure: A Prospective Study. Dis Colon Rectum 2006;06. 49:858-864.
33. Heymen S, Wexner SD, Gulledge AD. MMPI assessment of patients with functional bowel disorders. Dis Colon Rectum 1993;36:593-596.
34. Devroede G, Gilles G, Bouchoucha M, et al. Idiopathic constipation by colonic dysfunction: relationship with personality and anxiety. Dig Dis Sci 1989;34:1428-1433.
35. Park UC, Yoo YB, Kim JJ, Nam BW. Psychiatric investigation by using the Minnesota multiphasic Personality Inventory in patients with chronic constipation. J Korean Soc Coloproctol 2002;18:95-103.
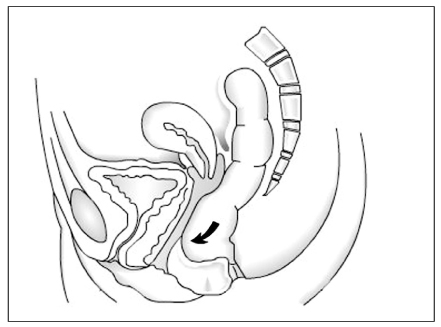
Figure 2
Illustration of cinedefecography showing progression of internal intussusception. Findings suggestive of preprolapse include funnel-shaped confuguration of the rectum and the formation of a "ring pocket"

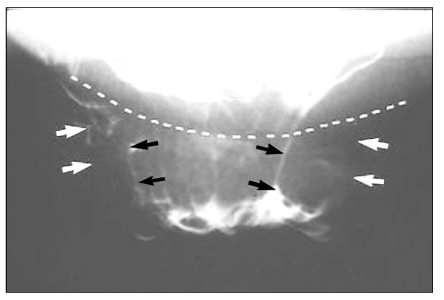
Figure 3
Left: Full thickness rectal prolapse (note concentric folds).
Right: Rectal mucosal prolapse (note radial folds)

Figure 5
Defecography demonstrates a third degree sigmoidocele in patient with pelvic outlet obstruction (black arrow). The contrast material is also in the lower rectum showing rectocele (white arrow)
Sig.: sigmoid colon, RC: rectocele
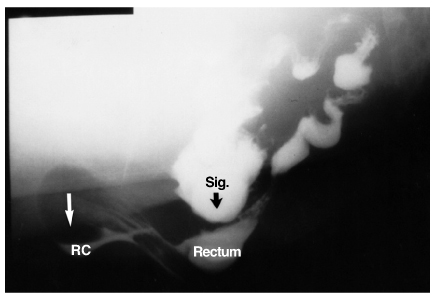
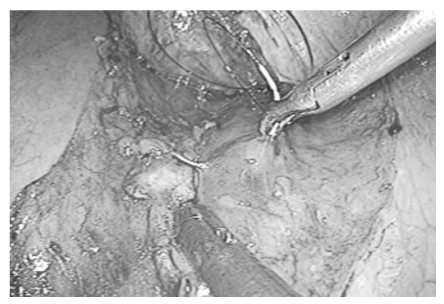
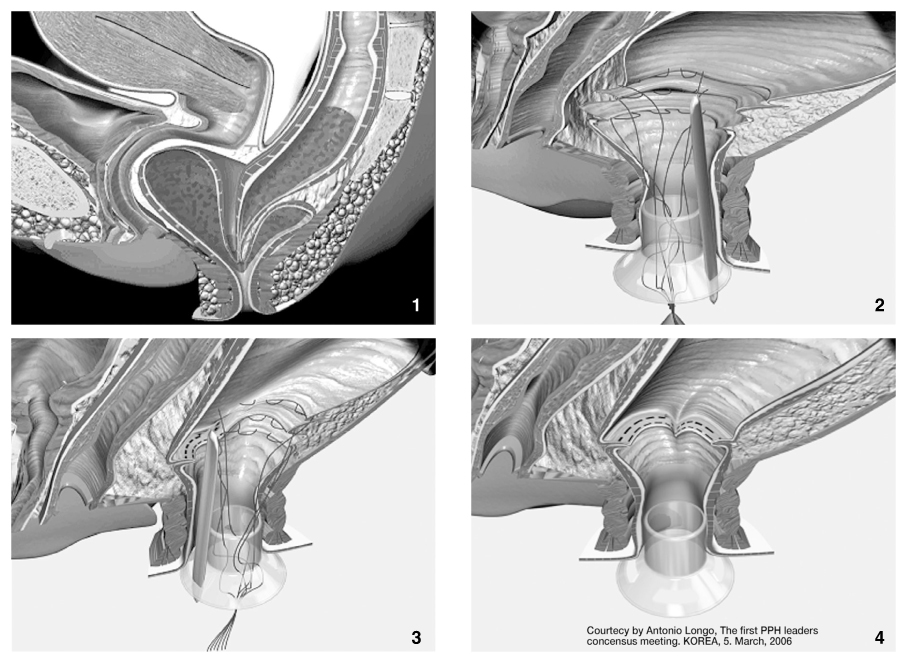
Figure 6
STARR (stapled trans-anal rectal resection) procedure. The operation was carried out by circular stapled prolapsectomy in the treatment of rectal internal mucosal prolapse(23)
- TOOLS
-
- Share :
-





-
METRICS

-
- 1 Crossref
- Scopus
- 1,118 View
- 2 Download
-

-
Related articles in
J Korean Med Assoc -
Diagnosis and management of sarcopenia2024 July;67(7)
Surgical treatment of esophageal cancer2024 February;67(2)
Surgical treatment for gastroesophageal reflux disease2022 December;65(12)
Surgical treatment for metastatic colorectal cancer2022 September;65(9)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
