



 |
 |
| J Korean Med Assoc > Volume 49(4); 2006 > Article |
Abstract
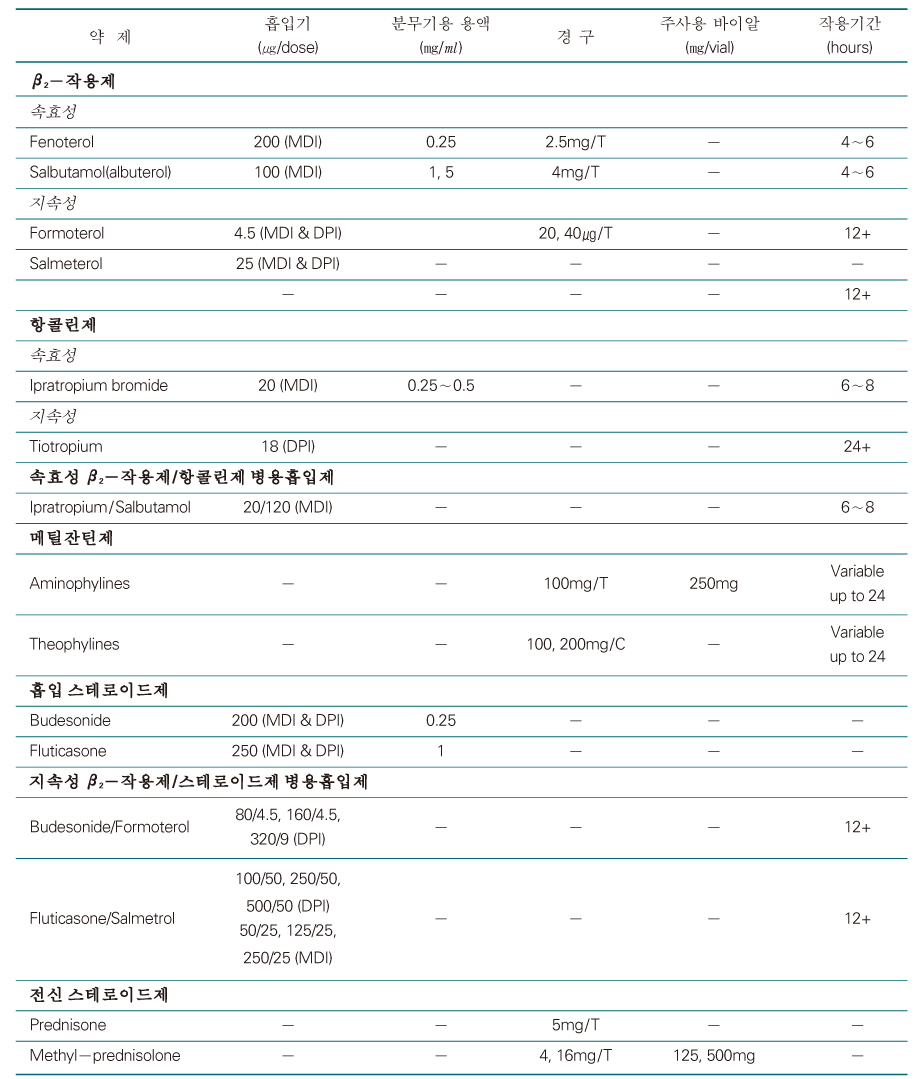
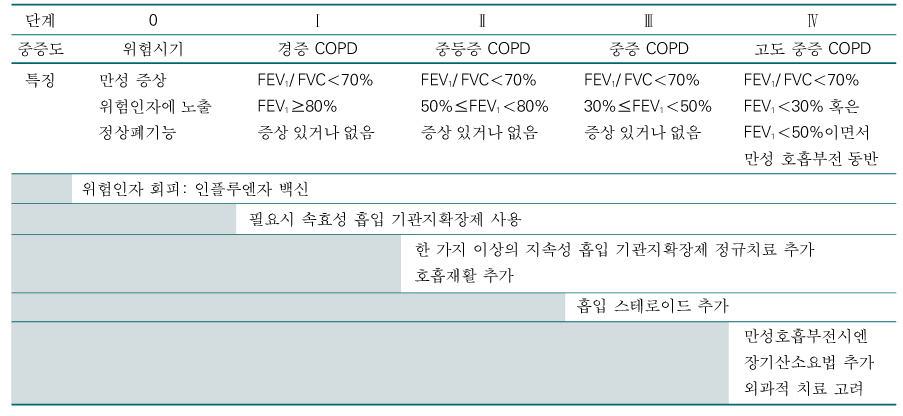
The general approach to manage stable COPD is characterized by a stepwise increase in treatment, depending on the severity of the disease. None of the existing medications for COPD have been shown to modify the long-term decline in lung function that is the hallmark of the disease. Therefore, pharmacotherapy in COPD is used to decrease symptoms and/or complications. Bronchodilator medications are central to the symptomatic management of COPD. They are given on an as-needed basis or on a regular basis to prevent or reduce symptoms. The principal bronchodilator treatments are β2-agonists, anticholinergics, theophylline, and a combination of these drugs. Regular treatment with long-acting bronchodilators is more effective and convenient than treatment with short-acting bronchodilators, but more expensive. The addition of regular treatment with inhaled steroids to bronchodilator treatment is appropriate for symptomatic COPD patients with an FEV1<50% predicted (Stage III: Severe COPD and Stage IV: Very Severe COPD) or repeated exacerbations (for example, more than 3 times during the last 3 years). Chronic treatment with systemic steroids should be avoided, if possible.
References
1. Global Strategy for The Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. 2004 Updated Global Initiative for Chronic Obstructive Lung Disease www.goldcopd.org
3. van Noord JA, Bantje TA, Eland ME, Korducki L, Cornelissen PJ. The Dutch Tiotropium Study Group. A randomised controlled comparison of tiotropium and ipratropium in the treatment of chronic obstructive pulmonary disease. Thorax 2000;55:289-294.
4. Kim SJ, Kim MS, Lee SH, Kim YK, Moon HS, Park SH, et al. A comparison of tiotropium 18µg, once daily and ipratropium 40µg, 4 times daily in a double-blind, double-dummy, efficacy and safety study in adults with chronic obstructive pulmonary disease. Tuberc Respir Dis 2005;58:498-506.
5. Murciano D, Auclair MH, Pariente R, Aubier M. A randomized, controlled trial of theophylline in patients with severe chronic obstructive pulmonary disease. N Engl J Med 1989;320:1521-1525.
6. Pauwels RA, Lofdahl CG, Laitinen LA, Schouten JP, Postma DS, Pride NB, et al. Long-term treatment with inhaled budesonide in persons with mild chronic obstructive pulmonary disease who continue smoking. European Respiratory Society Study on Chronic Obstructive Pulmonary Disease. N Engl J Med 1999;340:1948-1953.
7. Burge PS, Calverley PM, Jones PW, Spencer S, Anderson JA, Maslen TK. Randomised, double blind, placebo controlled study of fluticasone propionate in patients with moderate to severe chronic obstructive pulmonary disease: the ISOLDE trial. BMJ 2000;320:1297-1303.
8. COMBIVENT Inhalation Aerosol Study Group. In chronic obstructive pulmonary disease, a combination of ipratropium and albuterol is more effective than either agent alone. An 85-day multicenter trial. Chest 1994;105:1411-1419.
9. Van Noord JA, de Munck DR, Bantje TA, Hop WC, Akveld ML, Bommer AM. Long-term treatment of chronic obstructive pulmonary disease with salmeterol and the additive effect of ipratropium. Eur Respir J 2000;15:878-885.
10. Mahler DA, Wire P, Horstman D, Chang CN, Yates J, Fischer T, et al. Effectiveness of fluticasone propionate and salmeterol combination delivered via the Diskus device in the treatment of chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2002;166:1084-1091.
11. Calverley P, Pauwels R, Vestbo J, Jones P, Pride N, Gulsvik A, et al. Combined salmeterol and fluticasone in the treatment of chronic obstructive pulmonary disease: a randomised controlled trial. Lancet 2003;361:449-456.
12. Nichol KL, Margolis KL, Wuorenma J, Von Sternberg T. The efficacy and cost effectiveness of vaccination against influenza among elderly persons living in the community. N Engl J Med 1994;331:778-784.
- TOOLS
-
- Share :
-





-
METRICS

-
- 0 Crossref
- Scopus
- 1,013 View
- 1 Download
-

-
Related articles in
J Korean Med Assoc -
Pharmacotherapy for patients with Alzheimer’s disease2024 March;67(3)
Pharmacotherapy for pulmonary embolism: new anticoagulants2022 July;65(7)
Pharmacotherapy for female nocturia2021 June;64(6)
Updated view on the treatment of chronic obstructive pulmonary disease in Korea2021 March;64(3)
Anesthetic management of patients with chronic obstructive pulmonary disease2020 September;63(9)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
