






 |
 |
| J Korean Med Assoc > Volume 48(8); 2005 > Article |
Abstract
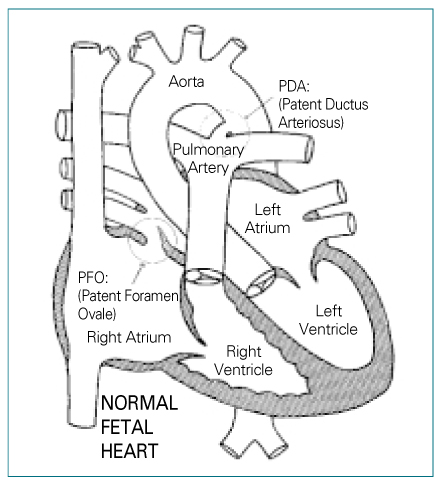
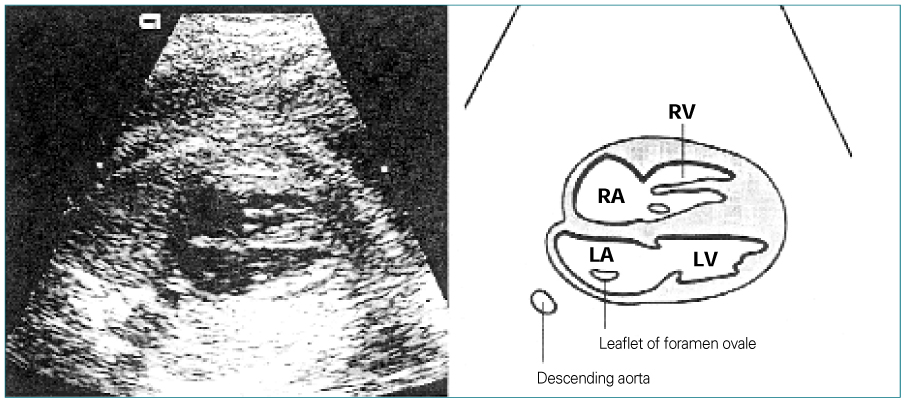
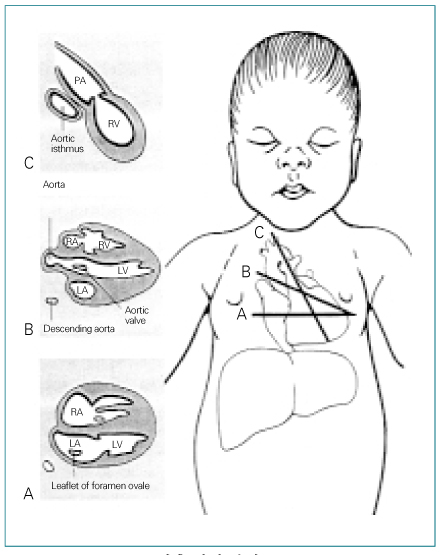
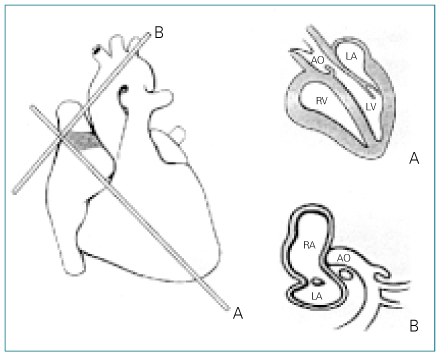
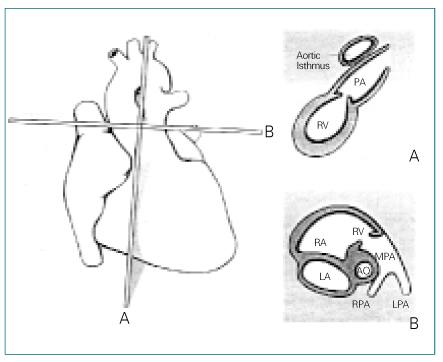
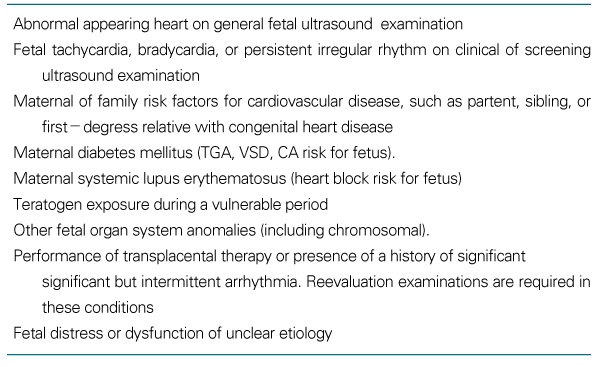
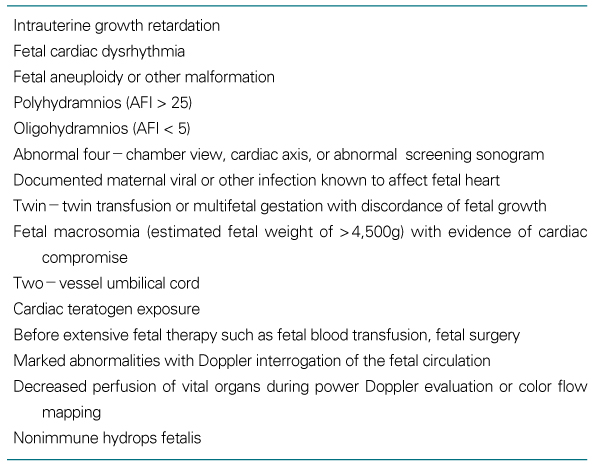
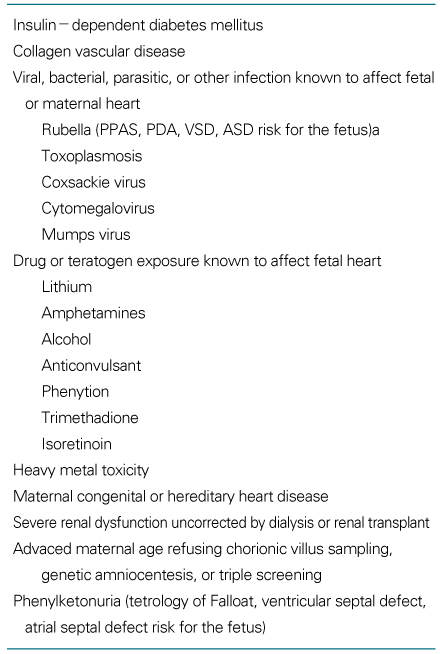
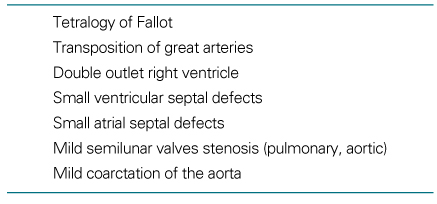
Congenital heart disease(CHD) is the most common congenital abnormality in human fetus, accounting for more than half of deaths from congenital abnormalities in childhood. Fetal echocardiography has been shown to be able to identify the majority of structural cardiac abnormalities, and it has traditionally been reserved for pregnancies at high risk for CHD. Most neonates with CHD, however, have no identifiable risk factors. When a sonogram is performed during pregnancy for defined clinical reasons, a four-chamber view of the fetal heart is routinely performed. However, a four-chamber view of the fetal heart does not reliably detect the most common CHD such as ventricular septal defect, coarctation of the aorta, transposition of the great arteries, and tetralogy of Fallot. Therefore, the vast majority of cases of CHD are left undetected even in those women who have undergone an obstetric ultrasound. A high level of suspicion of the presence of CHD and attention to anatomic details should be part of every ultrasound examination, especially when involving low-risk pregnancies, and it is currently recommended that only those fetuses with significant risk factors be referred for a targeted sonogram and fetal echocardiogram.
References
1. Hofman JI, Christian R. Congenital heart disease in a cohort of 19,502 births with long term follow-up. Am J Cardiol 1978;42:641-647.
2. Lian ZH, Zach MM, Erickson JD. Paternal age and occurrence of birth defects. Am J Hum Genet 1986;39:648-660.
3. Mitchell SC, Korones SB, Berendes HW. Congenital heart disease in 56,109 births. Circulation 1971;43:323-332.
4. Ewigman BG, Crane JP, Frigoletto FD, LeFevre ML, Bain RP, McNellis D. RADIUS Study Group. Effect of prenatal ultrasound screening on perinatal outcome. N Engl J Med 1993;329:821-821.
5. Cullen S, Sharland GK, Allan LD, Sullivan ID. Potential impact of population screening for prenatal diagnosis of congenital heart disease. Arch Dis Child 1992;67:775-778.
6. Chitlin MD, Alpert JS, Armstrong WF, Aurigemma GP, Beller GA, Ryan TJ, et al. ACC/AHA guidelines for the clinical application of echocardiography: Executive summary. J Am Coll Cardiol 1997;29:862-879.
7. Hess DB, Flaker G, Aggarwal KB, Buchheit LC, Hess LW. In: Hess DB, Hess LW, editor. Fetal cardiac imaging. Fetal echocardiography 1999;Stamford: Appleton & Lange. 149-194.
8. Yagel S, Weissman A, Rotstein Z, manor M, Hegesh J, Achiron R, et al. Congenital heart defects: natural course and in utero development. Circulation 1997;96:550-555.
9. Abuhamad A. A practical guide to fetal echocardiography 1997;Philadelphia: Lippincott-Raven.
10. Comstock CH. Normal fetal heart axis and position. Obstet Gynecol 1987;70:255-259.
11. Shipp TD, Bromely B, Hornberger LK, Nadel A, Benacerraf BR. Levorotation of the fetal cardiac axis: a clue for the presence of congenital heart disease. Obstet Gynecol 1995;85:97-102.
12. Truesdell SC. In: Jaffe R, Bui TH, editor. Fetal cardiography. Textbook of fetal ultrasound 1999;New York: Parthenon Publishing Group. 153-173.
13. Friedman AH, Copel JA, Kleinman CS. Fetal echocardiography and fetal cardiology: Indications, diagnosis and managment. Seminars in perinatology 1993;17:76-88.
Table 4
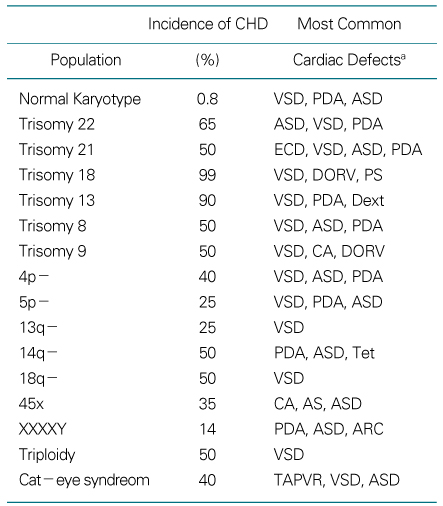
aVSD, ventricular septal defect; PDA, patent ductus arteriosus; ASD, atrial septal defect; TAPVR, total anomalous pulmonary venous returm; Dext, dextrocardia; DORV, double-outlet right ventricle; PS, pulmonary valve stenosis; ECD, endocardial cushion defect; CA, coarctation of the aorta; AS, aortic valve stenosis; ARC, anomalous right coronary artery; Tet, tetralogy of Fallot
- TOOLS
-
- Share :
-





-
METRICS

-
- 0 Crossref
- Scopus
- 1,041 View
- 4 Download
-

-
Related articles in
J Korean Med Assoc
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
