



 |
 |
| J Korean Med Assoc > Volume 47(11); 2004 > Article |
Abstract
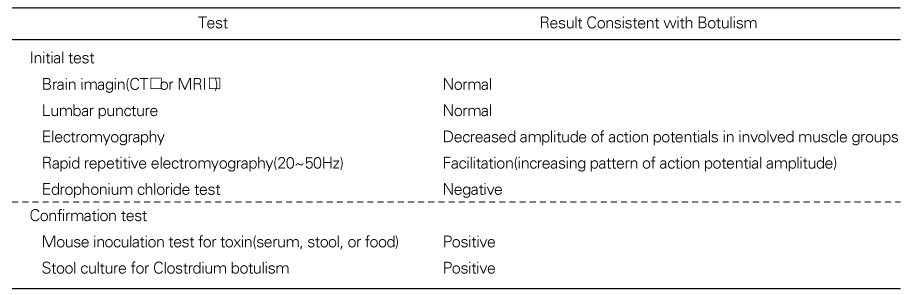
Botulism is a life threatening disorder caused by a neurotoxin produced from the anaerobic, spore-forming bacterium Clostridium botulinum. There are seven antigenically distinct types of botulinum neurotoxins (types A through G), and the human botulism is primarily caused by toxin types A, B, and E. Four clinical forms of botulism occur in humans: foodborne botulism, wound botulism, infant botulism, and adult infectious botulism. Botulism is characterized by symmetric, descending, flaccid paralysis of motor and autonomic nerves, usually beginning with the cranial nerves. Dry mouth, blurred vision, and diplopia are usually the earliest neurologic symptoms. Botulism should be suspected in a patient with an acute onset of gastrointestinal, autonomic, and cranial nerve dysfunction. Confirmation of the diagnosis of botulism depends on the detection of the toxin or the organism in the patient. The most reliable method for the detection of the toxin is the mouse inoculation test. The mainstay of treatment for severe botulism is supportive therapy with mechanical ventilation. The administration of antitoxin is the only specific pharmacologic treatment available for botulism. Botulism is a rare but potentially fatal illness, so timely recognition of the clinical symptoms plays an important role in decreasing the mortality rate.
References
1. van Ermengem E. Classics in infectious disease. A new anaerobic bacillus and its relation to botulism. Rev Infect Dis 1979;1:701-719. [Reprint of van Ermengem's original article, first published in 1897] (Cited from Reference 7).
3. Lund BM. Foodborne disease due to Bacillus and Clostridium species. Lancet 1990;336:982-986.
4. Simpson LL. Molecular pharmacology of botulinum toxin and tetanus toxin. Ann Rev Pharmacol Toxicol 1986;26:427-453.
5. Lamana C. The most poisonous poison. Science 1959;130:763-772.
6. Eitzen LT, Caudle MA. Medical Management of Biological Casualties 1993;Fort Detrick, MD: U.S. Army Medical Research Institute of Infectious Disease. Publication no. 20170-5011.
7. Shapiro RL, Hatheway C, Swerdlow DL. Botulism in the United States:A clinical and epidermiologic review. Ann Intern Med 1998;129:221-228.
9. Woodruff BA, Griffin PM, McCroskey LM, Smart JF, Wainwright RB, Bryant RG, et al. Clinical and laboratory comparison of botulism from toxin types A, B, and E in the United States, 1975-1988. J Infect Dis 1992;166:1281-1286.
10. Hughes JM, Blumenthal JR, Merson MH, Lombard GL, Dowell VR Jr, Gangarosa EJ. Clinical features of types A and B food-borne botulism. Ann Intern Med 1981;95:442-445.
11. Merson MH, Dowell VR Jr. Epidemiologic, clinical and laboratory aspects of wound botulism. N Engl J Med 1973;289:1005-1010.
12. Wilson R, Morris JG Jr, Snyder JD, Feldman RA. Clinical characteristics of infant botulism in the United States: A study of the non-Califonia cases. Pediatr Infect Dis 1982;1:148-150.
13. St Louis ME. In: Evans AS, brachman PS, editor. Botulism. Bacerial Infections of Humans:Epidemiology and Control 1991;2nd ed. New York: Plenum Medical. 115.
14. Hatheway CL. In: Balows A, Hausler WH, Lennette EH, editor. Botulism. Laboratory diagnosis of infectious disease:Principles and Practice 1988;vol 1:New York: Springer-Verlag. 111.
15. Wictome M, Newton K, Jameson K, Hallis B, Dunnigan P, Shone C, et al. Development of an in vitro bioassay for Clostridium botulinum type B neurotoxin in foods that is more sensitive than the mouse bioassay. Appl Environ Microbiol 1999;65:3787-3792.
16. Fach P, Perelle S, Dilasser F, Grout J, Dargaignaratz C, Broussolle V, et al. Detection by PCR-enzyme-linked immunosorbent assay of Clostridium botulinum in fish and environmental samples from a coatal area in northern France. Appl Environ Microbiol 2002;68:5870-5876.
17. Hatheway CL, Snyder JD, Seals JE, Edell TA, Lewis GE Jr. Antitoxin levels in botulism patients treated with trivalent equine botulism antitoxin to toxin types A, B, and E. J Infect Dis 1984;150:407-412.
18. Tacket CO, Shandera WX, Mann JM, Hargrett NT, Blake PA. Equine antitoxin use and other factors that predict outcome in type A foodborne botulism. Am J Med 1984;76:794-798.
- TOOLS
-
- Share :
-





-
METRICS

-
- 0 Crossref
- Scopus
- 1,182 View
- 3 Download
-

-
Related articles in
J Korean Med Assoc
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
