Diagnostic Approach and Prognostic Factors of Cancers
Article information
Abstract
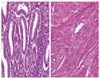
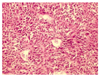
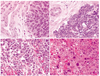
When one follows a systematic approach to make a diagnosis of pathologic lesions, it is relatively easy to render a cancer diagnosis in almost all cases in routine daily practice. The first step is to recognize whether or not the specimen contains a lesion and then to determine whether the lesion is neoplastic or non-neoplastic. Since neoplasm is clonal proliferation, neoplastic conditions are usually composed of a single cell type, whereas non-neoplastic conditions consist of multiple different cell types. After a neoplastic condition has been documented, the next step is to decide whether the neoplasm is of an epithelial origin or mesenchymal origin. The main differences between epithelial tumors and mesenchymal tumors include : 1) the tumor cells in epithelial tumors are oval, round to polygonal, while those in mesenchymal tumors are in general spindle-shaped : 2) epithelial tumors generally form tumor cell nests, while mesenchymal tumors arrange diffusely without forming tumor cell nests : 3) in epithelial tumors, desmoplastic stroma is well formed in between tumor cell nests, while in mesenchymal tumors there is no desmoplastic stroma ; and lastly, 4) feeding vessels open in the stroma in epithelial tumors, while they open between tumor cells in mesenchymal tumors. After this one should decide whether the tumor is benign or malignant. The differences between benign and malignant tumors include : 1) differentiation ; 2) growth rate ; 3) growth pattern ; and 4) metastasis. The benign tumor is well differentiated, grows slowly, shows an expansile growth pattern with encapsulation, and does not metastasize. On the other hand, the malignant tumor is in general poorly differentiated, grows rapidly with frequent mitoses, shows an invasive growth pattern without capsular formation, and frequently metastasizes. In general malignant tumors show a high cellularity, tumor necrosis, and nuclear alterations, which include nuclear enlargement with a high nuclear/cytoplasmic ratio, hyperchromatism, pleomorphism, prominent nucleolus, and frequent mitoses. The final step is to classify the type of tumor based on the cellular differentiation and gross and microscopic growth patterns based on the light microscopic examination of H & E stained slides. For the correct identification of the tumor, immunostaining, electron microscopic evaluation, and molecular diagnostic tools may be required. After establishment of a diagnosis of malignancy, one should think about the prognostic factors. The two well-known prognostic factors (category I) applicable in almost all tumors include stage and grade. Therefore, information about the stage and grade should also be included in the pathology report.