Epilepsy: Diagnosis
Article information
Abstract
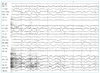
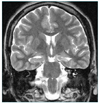
Aphysician faced with a patient who has an episodic disorder should determine whether the episode in question is indeed a seizure in the first place. If so, he or she should characterize its pattern and other characteristics, and finally, should delineate the underlying cause. Epilepsy is primarily a diagnosis based on a history and the initial assessment is based largely on the clinical history, especially on an accurate description of the event in question. The EEG, MRI, and routine blood tests should be included in the initial diagnostic workup. The EEG is undoubtedly the most sensitive, indeed indispensable, tool for the diagnosis of epilepsy, however, it must be used in conjunction with clinical data. A proportion of epileptic patients have a perfectly normal interictal EEG. Furthermore, a small number of healthy persons show paroxysmal EEG abnormalities. MRI is the most important diagnostic tool for the detection of structural abnormalities underlying epilepsy. Some patients may later need protracted video-EEG monitoring for the diagnosis of epilepsy. The conditions most likely to simulate a seizure are syncope and transient ischemic attacks. There is a rise in serum creatine kinase and serum prolactin levels after the seizure, which findings could be used in emergency room to assist in distinguishing seizures from syncope or pseudo-seizures.