안드로겐탈모증의 약물치료
Pharmacological therapeutics in androgenetic alopecia
Article information

Trans Abstract
Androgenetic alopecia (AGA) is the most common type of hair loss and affects both men and women. Male pattern hair loss shows characteristic frontal recession and vertex baldness, whereas female pattern hair loss produces diffuse alopecia over the mid-frontal scalp. AGA is mediated by increased androgen susceptibility in affected scalp hairs. 5α-Reductase converts testosterone into dihydrotestosterone, a potent androgen, in the scalp. Both androgen receptors and 5α-reductase have higher expression levels in the balding scalp than in non-affected regions. Increased androgen susceptibility induces hair follicle miniaturization, which leads to the progressive loss of thicker terminal hairs in the balding scalp. Currently, topical minoxidil and oral 5α-reductase inhibitors, such as finasteride and dutasteride, are approved options for the pharmacological treatment of AGA. Topical minoxidil remains the mainstay of therapy for mild to moderate AGA in both men and women. The daily intake of 1-mg finasteride or 0.5-mg dutasteride shows better efficacy than topical minoxidil in regard to hair regrowth in male AGA. Anti-androgens can be used in female AGA wit clinical and biochemical evidence of hyperandrogenism. Patients may be overwhelmed and confused by the variety of treatment options for AGA management, including over-the-count drugs with low evidence quality. Therefore, physicians must be aware of the current guidelines for the management of AGA based on evidence-based approaches to select better options for patients.
서론
안드로겐탈모증은 남성형탈모와 여성형탈모를 통칭하며, 남성호르몬에 대한 모낭의 병적 민감성으로 모낭의 소형화가 나타나 탈모가 진행하는 질환이다. 두피 모낭의 남성호르몬에 대한 민감성은 유전적 소인에 기인하고 후천적으로 다양한 인자가 질환의 발생과 진행에 영향을 주는 것으로 이해된다[1-3]. 따라서 현재까지는 피부 내 활성화된 남성호르몬의 작용을 억제하는 치료제를 주로 사용하게 된다. 이 종설에서는 안드로겐탈모증의 발생기전과 현재 많이 활용되는 약물치료에 대해 논의하고자 한다.
안드로겐탈모증의 병인
체내에는 다양한 형태의 안드로겐이 존재하며, 대표적인 것이 테스토스테론(testosterone)이다. 테스토스테론과 디하이드로테스토스테론(dihydrotestosterone, DHT)은 역가가 강한 안드로겐으로 구분되며, dehydroepiandrosterone, dehydroepiandrosterone sulfate나 androstenedione 등은 비교적 약한 안드로겐으로 작용한다[4]. 피부는 안드로겐을 자체적으로 합성하는 말초기관으로, 이러한 안드로겐들은 여러 효소에 의해 상호전환이 가능하다[3]. 특히 테스토스테론과 DHT 그리고 5α-reductase (5AR)는 남성형탈모 병인에 가장 중요한 역할을 한다. 테스토스테론은 5AR에 의해 DHT로 전환되며, DHT는 테스토스테론보다 안드로겐수용체에 대해 더 강한 친화력을 보인다[3,4]. 현재까지 세 가지 5AR 동종이형체가 확인되었다. 1형과 3형은 신체 전반적으로 분포하고 있으며, 1형의 경우 모발피지선 단위 내에서는 피지샘에 주로 분포한다. 2형은 전립선, 부고환, 모낭을 비롯한 안드로겐 표적 조직에 주로 분포하고 있으며 피부에서는 주로 바깥뿌리집, 속뿌리집 및 모유두에서 높게 발현된다[5,6].
안드로겐탈모증 환자의 탈모부 두피에는 후두부와 같이 탈모가 일어나지 않는 부위에 비해 5AR 활성이 높게 발현된다[7-9]. 따라서 탈모부 모낭에서는 테스토스테론에서 DHT로의 전환이 활발히 일어나고, 세포 내 DHT는 안드로겐수용체와 결합하여, 핵내 androgen response element에 결합 후, 안드로겐 표적 유전자의 전사를 증가시킨다(Figure 1) [3]. 진피유두에서는 이러한 경로로 DHT가 작용하면, 안드로겐탈모증 환자에서는 주로 transforming growth factor β와 같은 성장저해인자의 전사가 증가되어 인접한 모기질의 각질형성세포의 증식을 억제하므로 모낭이 가늘어지는 주요 기전이 된다[3,10,11]. 반대로, 다른 안드로겐 의존 부위인 겨드랑이이나 턱수염 모낭에서는 안드로겐 수용체의 활성화에 의해 진피유두에서 각질형성세포의 분화와 증식을 촉진하는 insulin-like growth factor-1 등을 증가시켜 털을 굵고 길게 만든다. 이러한 안드로겐탈모증이 발생하는 두피에서 역설적으로 성장억제 신호가 관찰되는 것은 발생학적 기원의 차이에 의한 변화로 이해되나, 아직 해부학적 부위에 따른 안드로겐의 작용이 다른 원인은 명확히 밝혀져 있지 않다[3,11,12].
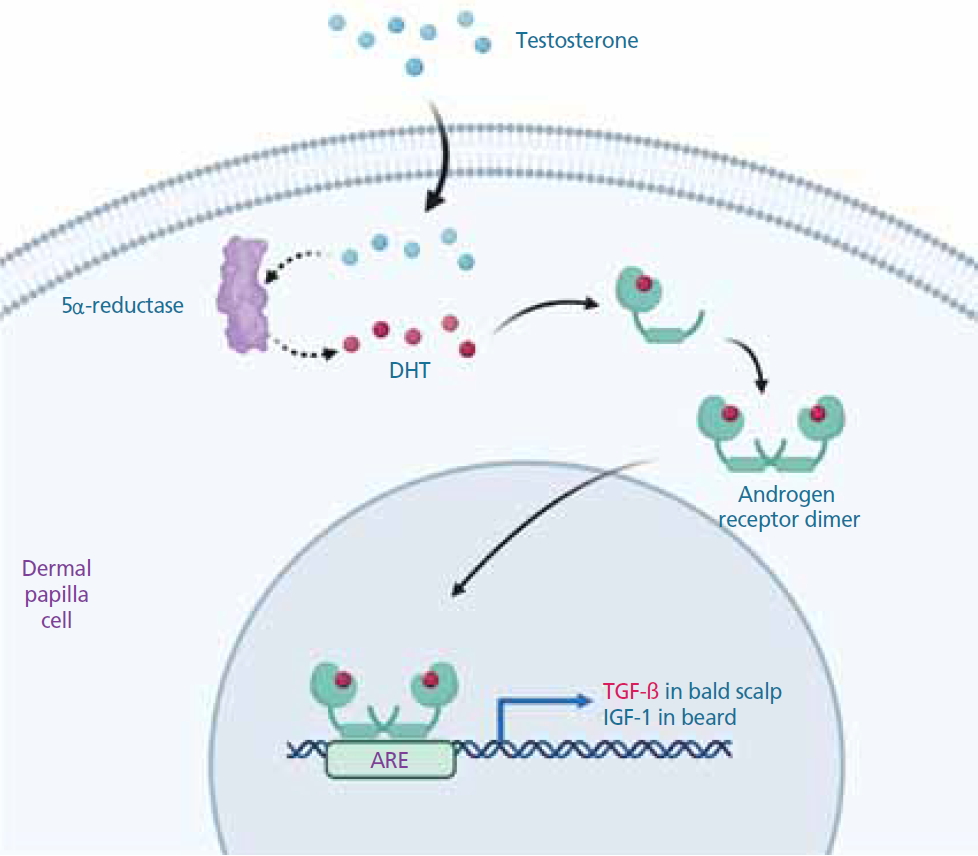
Role of androgens in androgenetic alopecia. Testosterone from the bloodstream enters dermal papilla cells and is converted into dihydrotestosterone (DHT), a more potent androgen, by 5α-reductase. DHT has a higher affinity to androgen receptors, which form dimeric complexes after binding with DHT. Androgenbound androgen receptors translocate into the nucleus and bind to androgen receptor elements (AREs). Subsequently, the transcription of target genes occurs. In the balding scalp, dermal papilla cells paradoxically produce growth factors that negatively regulate the proliferation of the hair matrix, such as transforming growth factor β (TGF-β). The paracrine secretion of TGF-β causes the miniaturization of hair follicles in androgenetic alopecia. IGF-1, insulin-like growth factor-1. Illustrated by the authors.
안드로겐의 활성과 연관된 변화 이외에도 안드로겐탈모증 환자의 두피 내에는 프로스타글란딘(prostaglandin)의 활성 변화도 나타나는 것으로 알려져 있다. 프로스타글란딘은 염증과 통증의 매개, 안압 조절 및 성호르몬의 대사 등 다양한 기능을 하는데, 모낭에서 프로스타글란딘 D2는 주로 모발의 성장을 억제하고 프로스타글란딘 E2와 프로스타글란딘 F2α는 모발 성장을 촉진하는 작용을 하는 것으로 알려져 있다. 특히 안드로겐탈모증의 두피 내에는 프로스타글란딘 D2 발현이 증가되어 있고, 이는 모낭줄기세포에서 전이 증폭세포로의 정상적인 분화가 일어나지 않는 것과 연관된 것으로 이해되고 있다[13,14]. 프로스타글란딘 조절을 표적으로 한 새로운 약제 개발의 임상연구는 진행중에 있다[15].
임상양상과 진단
모낭의 성장 주기는 퇴행기(catagen)로 시작되어 모발의 성장이 중단되는 휴지기(telogen)로 이어지고 그 다음 새로운 주기의 생장기(anagen)가 시작된다. 정상적으로 머리카락의 경우 약 90%가 생장기에 해당하며 10% 이내가 휴지기에 해당한다. 개개의 머리카락 생장기 기간은 3-6년으로 생각되며, 이 생장기의 길이가 모발의 굵기와 길이를 결정하게 된다. 안드로겐탈모증 환자의 두피에서 앞에서 서술된 안드로겐 작용에 의해 모유두의 성장억제신호가 발현되게 되면 이러한 생장기의 주기가 수개월로 짧아지게 된다. 따라서 모낭이 길어지지 않고 짧고 가는털 상태로 있다가 휴지기를 거쳐 탈락이 된다. 이러한 점진적인 모낭의 소형화에 의해 안드로겐탈모증의 전형적인 임상양상을 나타내게 된다.
안드로겐탈모증은 20대 중반부터 탈모가 시작되는 경우가 많으며, 연령이 증가함에 따라 발생빈도가 점점 증가한다. 탈모는 급격히 일어나는 것이 아니라 여러 단계를 걸쳐 서서히 진행된다. 남성형탈모증에서는 앞머리 모발이 먼저 가늘어지고 모발선이 M자형으로 변하면서 뒤로 후퇴하는 양상이 초기에 나타나며, 정수리 모발도 점점 가늘어져 탈모에 이르는 진행과정을 거친다. 이러한 앞머리와 정수리 탈모의 정도와 모양에 따라 type I-VII 로 구분한 것이 Hamilton-Norwood scale이다. 여성에서는 남성과 달리 앞머리선은 유지되면서 정수리를 포함한 머리 위쪽이 전체적으로 모발이 가늘어지면서 광범위한 침범 소견을 보이게 된다. 따라서 여성형탈모증에는 Ludwig 분류법이 주로 사용되며 중등도에 따라 1-3단계로 구분된다[16]. 다만, 이러한 임상적변화는 성별에 따라 이분법적으로 나뉘지는 않고, 남성에서도 여성형탈모증의 형태로 탈모가 진행될 수 있다. 최근 대한모발학회를 중심으로 발표된 BASP분류법(basic and specific classification)은 남성형탈모 및 여성형탈모 모든 환자의 임상양상과 탈모의 중등도를 쉽게 표현할 수 있어 현재 우리나라에서는 가장 널리 활용되고 있다[17].
안드로겐탈모증은 남성에서 일정한 패턴을 보이면서 탈모가 진행되기 때문에 육안적인 관찰로도 정확한 진단을 내리기가 쉬운 편이다. 그러나 탈모 초기에 내원한 경우나 다른 탈모 질환이 동반되어 있는 경우, 그리고 여성에서는 일정한 패턴이 명확하지 않을 수 있어, 보다 정확한 진단을 위해 육안적 진단 외에 모발확대경 검사 등을 포함한 추가적인 검사를 시행할 수 있다.
약물치료
현재 미국 식품의약국(Food and Drug Administration, FDA)에서 안드로겐탈모증의 치료제로 승인된 약물은 국소 미녹시딜(minoxidil)과 경구 5AR억제제뿐이다[18-20]. 이러한 약물적 치료에 의해 호전되지 않거나, 내원 시부터 진행된 탈모를 보이는 경우는 모발이식과 같은 수술적 접근이 추천된다(Figure 2) [21]. 이외 치료효과와 안정성에서 충분한 근거가 정립되지 않았지만 몇몇 약물이 실제 임상에서 활용되고 있어, 이들을 중심으로 정리해보고자 한다.
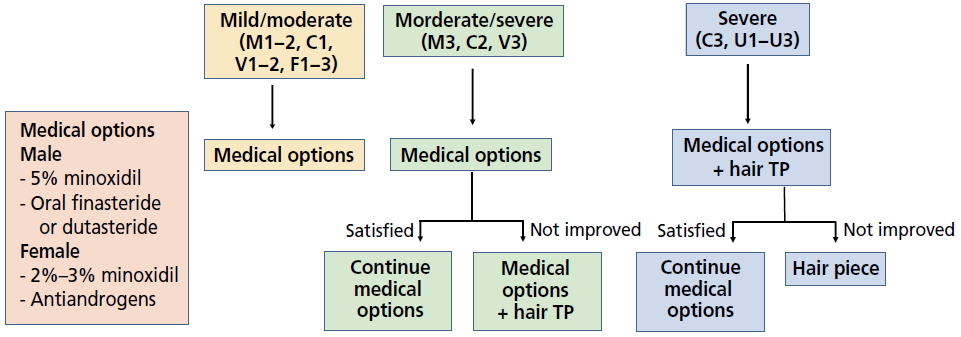
Clinical guideline for the management of androgenetic alopecia. The therapeutic strategy was stratified based on a severity scoring system assessed by the BASP (basic and specific) classification. TP, transplantation. Reproduced from Lee WS, et al. J Eur Acad Dermatol Venereol 2013;27:1026-1034, with permission from John Wiley & Sons, Inc. [21].
1. 국소치료
미녹시딜은 항고혈압 약물로 개발되었다가 다모증이 흔한 부작용으로 확인되어 국소 발모제로 개발되었고, 1988년 안드로겐탈모증의 치료제로 FDA 승인을 받았다. 액상 제형은 2-3% 농도로 여성형탈모에서, 5% 농도는 남성형탈모에 사용되며, 최근 개발된 폼(foam) 제형은 5% 단일 농도로 개발되어 여성 및 남성에서 모두 사용 가능하다. 아직까지 발모의 기전은 명확하지 않으나, 모낭에서 adenosine triphosphate sensitive potassium channel을 활성화시키거나 혈관내피성장인자와 그 수용체의 발현을 증가시켜 혈관생성을 통해 모발의 생장기를 촉진하는 것으로 생각된다.
미녹시딜을 도포하면 6-8주 내에 효과가 나타나기 시작하며, 40세 이하, 유병기간이 10년 이하, 탈모 부위의 직경이 10 cm 이하, 길이 1 cm 이상의 소형화된 모발이 남아 있는 경우 더 좋은 효과를 나타낸다[22,23]. 발모의 최대 효과는 치료 6-12개월에 나타나고, 그 이상 장기치료 시에는 점차 치료효과가 감소한다. 미녹시딜 도포를 중단하면 빠르게 탈모가 진행되어 4-6개월 후에는 모발이 치료 이전 상태로 돌아가게 된다. 남성형탈모증의 경우 5% 미녹시딜이 2% 미녹시딜보다 더 나은 효과를 보였고, 여성에서도 고농도를 도포하는 경우 효과는 우수하였으나 부작용 발현빈도가 유의하게 높아 액상의 경우 저농도를 권고한다[24,25]. 다만 최근연구에서 5% 폼 제형을 사용하는 경우에 환자 편의성이 개선되고 두피 자극 등 부작용이 적어 여성에서도 5% 미녹시딜 폼 사용은 권고된다[26,27].
미녹시딜 도포 후에는 심혈관계 등에 대한 부작용이 일부 보고되었으나 드물고 경미하다. 국소 부작용은 비교적 흔하게 나타나며 두피의 건조감, 가려움, 홍반 등의 자극반응이 흔하다. 또한 이마나 뺨의 솜털이 굵어지는 다모증이 여성에서는 흔히 발생할 수 있다. 미녹시딜 도포 1-2개월 이내 일시적으로 모발의 갑자기 많이 빠지는 현상이 있을 수 있는데, 이는 탈모의 악화가 아니라 휴지기 모발을 조기에 탈락시켜 새로운 모발이 나오는 것을 촉진시키는 현상이므로 치료를 중단할 필요는 없다.
여성의 안드로겐탈모증에 허가된 약물로 0.025% 알파트라디올(alfatradiol) 용액이 사용될 수 있으나 현재 치료 효과에 대한 일관된 연구결과는 부족하다[28]. 녹내장 치료제로 허가되어 사용된 라타노프로스트(latanoprost)나 비마토프로스트(bimatoprost)와 같은 국소 프로스타글란딘 F2α 작용제는 눈썹발모제로 활용될 수 있으나, 현재까지 안드로겐탈모증을 대상으로 한 연구에서는 임상적 유효성이 입증되지 않았다[29,30]. 국외에서는 피나스테리드 또는 두타스테리드를 국소도포제로 개발하여 안드로겐탈모증 치료에 적용한 사례가 보고되고 있으나 아직 장기 안정성과 유효성에 대한 근거는 불충분하다[31].
2. 전신약물치료
1) 5AR억제제
현재 두 가지 5AR억제제가 시판되고 있다(Table 1). 피나스테리드는 2형 5AR을, 두타스테리드는 1형과 2형 5AR 모두를 억제하여 DHT를 낮추어 탈모를 억제하고 개선한다. 피나스테리드는 미국 FDA에서 1997년, 국내에서 2000년에 안드로겐탈모증에 사용승인을 받고 시판중인 약물이며, 남성 안드로겐탈모증에 하루 1 mg 매일 복용으로 사용된다. 임상 승인을 위한 대규모 3상연구로 1,553명의 남성 안드로겐탈모증 환자를 대상으로 위약 포함 무작위배정연구가 진행되었고, 탈모 진행의 억제와 모발확대경 및 연구자 평가지표에서 모두 유의한 모발 수의 증가 효과가 확인되었다[32]. 피나스테리드 복용 시작 후, 약제의 효과는 대개 2-3개월 후부터 나타나며, 6개월 경부터 객관적인 발모의 증가가 보이며, 대개 1년까지 모발이 증가하고 그 이후에는 조금 감소하는 경향을 보이나 위약군과 비교하였을 때, 지속적으로 유의한 탈모예방 효과를 보인다[32]. 젊은 환자의 경우 모발증가 효과가 2년까지 지속되기도 한다[32,33]. 따라서 환자에게 약물의 효과를 설명할 때는 객관적인 발모증가는 약물복용 초기에 관찰되나 장기적으로 투약하는 경우 위약 대비 탈모예방을 통해 치료효과를 극대화할 수 있음을 주지시켜, 환자의 순응도를 높이는 것이 중요하다. 단기간 약제를 사용하고 중단한 경우에는 이러한 개선효과가 빠르게 없어지는 것을 예상할 수 있다[32].

Comparison of commercially available 5α-reductase inhibitors
두피 부위별로는 정수리, 앞머리 및 옆머리 모두에서 치료 후 모발성장의 효과가 있다. 젊은 환자의 경우 모든 두피 부위에서 우수한 효과를 보이나, 고령의 경우 앞머리 모발선 부위와 옆머리에서의 효과는 조금 떨어지는 것으로 알려져 있다[32,34].
10년간 장기투약 연구결과에서도 이러한 치료효과는 유지되는 것으로 알려져 있고, 10년 치료 결과, 86%에서 진행억제 및 탈모개선의 유익한 효과를 유지하였다[35]. 18-40세 126명의 남성을 대상으로 한 국내 장기 관찰연구에서는 5년 후 탈모 개선이 85.7%, 진행억제가 98.4%로 보고되어 기존 장기 효용성 연구와 유사한 결과를 보였다[34].
두타스테리드는 1형 및 2형 5AR을 모두 억제하며 특히 2형 5AR 억제효과가 피나스테리드보다 더 강력한 것으로 알려져 있다[36]. 용량 비교 임상연구에서는 하루 0.1 mg 이상 용량에서 유의한 치료효과를 보였고 혈중 테스토스테론과 DHT에 대한 영향을 고려하여 최종적으로는 양성전립선비대증의 치료용량과 동일한 0.5 mg가 사용되고 있다. 허가를 위한 다기관 3상 임상연구는 국내에서 처음 시행되었고, 안드로겐탈모증에서의 효과와 안전성이 입증되어 2009년 우리나라 식약처 승인 후 시판 중이다[37]. 0-50세의 917명 환자들을 대상으로 피나스테리드와 두타스테리드의 효과를 비교한 연구에서는 3개월과 6개월 모두 피나스테리드에 비해 모발 개수의 유의한 증가를 보였고, 특히 정수리와 앞머리 모두에서 통계적으로 유의한 모발 개수 증가가 나타났다[38]. 최근 메타분석 연구에서도 적은 수의 비교임상연구들을 대상으로 분석하였으나, 두타스테리드가 피나스테리드 대비 우수한 치료효과를 보이는 것으로 보고하였다 [39]. 치료 후 임상적인 개선효과는 피나스테리드와 비슷한 시기에 나타나지만 장기 유효성에 대한 연구는 많이 진행되지 않아 추후 장기 유효성에 대한 임상 결과가 필요하다. 두 종류의 5AR억제제 병용요법은 허가되지 않았다. 다만 피나스테리드 단독치료 중 효과가 떨어지는 경우, 저용량 또는 주기요법으로 두타스테리드를 병합하는 경우 효과 개선이 보고되어 있으나, 장기적인 안정성 및 유효성에 대한 연구는 더 필요하다[40].
5AR억제제는 중증 부작용은 거의 없이 비교적 안전하게 사용된다. 약동학에서 간기능 혹은 신기능장애가 있는 경우에도 중증의 경우를 제외하면 용량조절 없이 사용 가능하며, 노령에서도 비교적 안전하게 사용되고, 약물 상호작용도 많지 않다[19,33]. 다만, 약물사용과 관련하여 흔히 발생될 수 있는 성기능 관련 부작용, 임신과 관련된 위험도, 전립선암 등 장기 안정성과 관련된 내용은 흔히 임상에서 질의를 받는 부분이어서 약제 안전성에 대한 정보는 숙지할 필요가 있다. 피나스테리나나 두타스테리드 사용 시 가장 흔한 성기능 관련 부작용은 성욕감퇴, 발기부전, 사정장애 등이 있다. 피나스테라이드의 5년 장기 안정성을 관찰한 연구에서는 성기능 관련 부작용의 발생은 투약 후 첫 1년에 가장 높은 것으로 알려져 있고, 약물투약이 길어지는 동안 그 발생률이 증가되지 않는다. 실제 성기능 관련 부작용 중 성욕감퇴의 경우 첫 1년 3.8% 이후 지속적으로 감소하여 5년째는 0.8% 정도로 보고되었다[41]. 일본에서 시행된 피나스테리드 10년 장기 관찰연구에서는 성기능 관련 부작용이 다소 높은 빈도(전체 6.8%, 성욕감퇴 5.6%, 발기부전 3.0%)로 보고되었으나 성기능 관련 부작용으로 약제가 중단된 사례는 없었다[42]. 이러한 성기능 관련 부작용은 ‘nocebo’ 현상으로 설명되기도 한다. 실제로 약물에 의한 부작용이라기보다는 환자가 약물로 인한 가능한 부작용을 알고 있을 때 나타나는 심리적인 영향을 의미한다. 최근 메타분석 결과, 두 종류의 5AR억제제의 성기능과 관련된 부작용의 빈도에 유의한 차이는 관찰되지 않았다[43].
남성이 5AR억제제를 복용하는 경우 배우자의 임신 결과에 미치는 영향은 미미하다. 181명의 피나스테리드 복용군을 대상으로 한 연구에서는, 정자 수, 정자의 운동성, 정자의 형태에서 유의한 영향이 관찰되지 않았다[44]. 일부 연구에서는 통계적인 유의성은 없으나 정자 수 등 실험실적 측정값이 감소되는 경향이 보고된 바는 있다. 사정 시 정액을 통해 배우자에게 전달되는 5AR억제제의 노출량도 무시할 정도로 예측된다. 따라서 예외적으로 임신한 배우자가 약물에 직접적으로 노출되지 않는 경우에는 남성의 5AR억제제가 수태능력이나 배우자의 임신 결과에 미치는 영향은 없는 것으로 예상된다. 다만, 남성 요인으로 불임이 지속되거나, 실험실적으로 관찰되는 정자수나 운동능 감소 등이 있는 경우에는 보수적인 접근에서는 약제 중단을 고려해볼 수 있고, 경증의 안드로겐탈모증의 환자가 수개월 내 임신을 계획하는 경우, 5AR억제제 투약의 시작은 성공적인 임신 이후에 시작하도록 권고할 수 있다.
피나스테리드 복용 군에서 장기 전립선암 발생률을 관찰한 연구에서는 악성도가 높은 전립선암의 발생비율이 증가된다는 보고가 있었으나, 이는 피나스테리드 복용 후 전립선 위축에 따른 조직검사 민감도의 변화와 같은 비약물적 요인들이 반영되지 않은 결과로 해석된다[45]. 현재 대규모 빅데이터 연구결과에서는 5AR억제제 장기복용이 전립선암의 발생률을 증가시킨다는 보고는 없다. 다만, 5AR억제제 복용 시에는 전립선특이항원(prostate specific antigen, PSA) 수치가 감소되므로, 건강검진에서 전립선암이나 전립선비대증 발생을 놓칠 수 있다. 약제 복용 6개월 이후부터는 50-60%의 혈청 PSA 감소가 피나스테리드와 두타스테리드에 의해 유발되므로, 이를 보정하여 PSA의 실제 수치를 판단하여야 하며, 중장년층 이상에서는 5AR억제제 투약 전 PSA 수치의 확인이 권고된다.
이 외에 기타 부작용으로 여성형유방이 5AR억제제 사용환자에서 드물게 보고되므로, 약제 투약 후 유방의 종창 또는 압통이 있는 경우 확인 및 투약중단이 필요하다. 피나스테리드증후군은 5AR억제제 투약 후 보고되고 있는 다양한 전신 증상과 우울감, 무기력감 등의 정서 변화를 포함하는 상태로 일반인들에게 알려져 있으나, 아직 약제와의 직접적인 연관성에 대한 학문적 근거는 미약하다[46].
여성에서 발생한 안드로겐탈모증, 즉 여성형탈모에서 5AR억제제 사용은 권고되지 않는다. 다만, 여성형탈모에서 제한적으로 5AR억제제를 사용한 기존 연구결과들에서는 2.5 mg 이상의 피나스테리드나 두타스테리드의 사용이 일부 환자들에게 유의한 발모증가 효과가 보고된 바 있다. 국내에서 112명의 여성형탈모 환자에게 18개월간 2.5 mg의 피나스테리드를 투약한 경우 94.7%에서 호전반응을 보여, 난치성 여성형탈모에서 제한적으로 사용해 볼 수는 있겠으나, 유방암 등의 호르몬 연관 악성종양의 발생 등 장기안전성에 대한 자료는 제한적이어서 환자 선정에 주의를 요하며, 가임기 여성의 경우 피임에 특별히 주의를 요한다[47,48].
2) 항안드로겐 약물 및 기타 전신약물요법
남성에서는 5AR억제제가 일차적으로 선택되고 내약성이 우수하므로 다른 종류의 항안드로겐 약물을 선택할 필요는 없다. 여성에서는 제한적으로 기타 항안드로겐 약물을 사용할 수 있고, 스피로노락톤(spironolactone), 사이프로테론아세테이트(cyproterone acetate), 플루타미드(flutamide) 등이 보고되었다. 다만, 이러한 약물의 장기 안정성과 탈모증에서의 유효성은 대규모 연구를 통해 검증되지 않았고, 플루타미드 등에서 보이는 간독성 등 내약성 등의 문제로 현재 거의 사용되지 않는다. 이 중에서는 비교적 내약성이 좋은 스피로노락톤이 다낭성난소증후군 등 안드로겐 과다증을 보이면서 여성형탈모가 진행된 경우 사용할 수 있고, 하루 50-200 mg 6개월 이상 복용하는 경우 발모 증가를 기대할 수 있다. 다만, 치료효과가 미녹시딜 도포에 비해 우월하지는 않으며, 위장장애, 생리불순, 과칼륨혈증 등의 발생 가능한 부작용을 면밀히 확인할 필요가 있다[18,49].
그 외 일반의약품으로 시판되는 calcium pantothenate, 케라틴, L-시스틴, 약용효모 등을 함유한 약제가 안드로겐탈모증의 치료보조제로 오인되어 처방되는 경우가 있으나, 이러한 약제군은 제한적으로 휴지기탈모증을 가진 여성을 대상으로 한 연구에 그 유효성을 기반으로 하고 있어, 안드로겐탈모증의 치료보조제로 사용하는 것은 과학적 근거가 부족하다[50].
결론
안드로겐탈모증은 유전적 소인을 가진 환자에서 두피 모낭의 안드로겐에 대한 과도한 민감성에 의해 모발의 성장기간(생장기)이 단축되어 발생한 모낭 소형화로 탈모가 진행되는 질환이다. 현재까지 공식적으로 승인된 약물요법은 국소치료제로 미녹시딜과 남성에서는 경구치료제로 피나스테리드와 두타스테리드가 추천된다. 미녹시딜의 작용기전은 잘 알려지지 않았지만 남성과 여성 모두에서 비교적 안전하게 사용될 수 있어 임상형과 무관하게 일차로 추천된다. 피부에서 테스토스테론을 DHT로 전환시키는 효소는 5AR이며, 피나스테리드는 2형 5AR를, 두타스테리드는 1형과 2형 5AR 모두를 억제하여 DHT를 낮추어 탈모를 억제하고 개선한다. 두 약제 모두 효과가 우수하고 안전한 약제이며 치료반응이 나오는데 최소 6개월 이상이 걸리므로 초기 투약 안정성이 확인이 되면 지속적으로 투약할 것을 권고하여야 한다. 이러한 약물적 치료에 저항하는 경우 모발이식 등의 수술적치료가 병행될 수 있다. 현재 안드로겐탈모증에 대한 다양한 중개연구와 임상시험들이 활발히 진행되고 있는 분야이므로 추후 새로운 신약이 출시될 것으로 기대한다.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Acknowledgements
This study was supported by the National Research Foundation of Korea(NRF) grant funded by the Korea government(MSIT) (No. 2020R1C1C1005198)
References
Peer Reviewers’ Commentary
이 논문은 탈모증의 가장 흔한 원인인 안드로겐탈모증의 병인, 임상 양상, 진단 방법과 함께 치료에 사용되는 도포제와 경구제의 사용 방법 및 주의사항에 관한 최신 지식을 정리하여 체계적으로 기술해 주고 있다. 안드로겐탈모증의 치료를 위해서는 6개월~1년 이상 약제를 사용해야 효과를 알 수 있으며, 장기간에 걸쳐 높은 순응도를 유지하기 위해서는 약제에 대한 정확한 정보를 환자에게 알려주어야 한다. 이 논문에서는 안드로겐탈모증 약제를 처방하기 전에 환자에게 반드시 알려주어야 할 사항과 환자가 궁금해 할 사항들을 알기 쉽게 설명해 주고 있다. 또한, 국내 안드로겐탈모증 환자의 연구 결과에 따른 치료 가이드라인도 함께 기술해 주고 있어, 임상 현장에서 탈모증을 치료하는 의사들에게 많은 도움이 될 것으로 판단된다.
[정리: 편집위원회]