서론
백반증은 멜라닌세포가 소실되어 피부에 흰 반점이 발생하는 흔한 탈색 피부질환으로, 특별한 자각증세는 없지만 환자의 삶에 심각한 영향을 미치고 있다. 백반증의 치료는 엑시머레이저와 전신 자외선요법 등 비수술적 치료가 주를 이룬다. 하지만, 긴 치료기간에도 불구하고 모든 환자에서 만족스러운 효과를 보이는 것은 아니며, 이 경우 수술적 치료가 중요한 대안이 될 수 있다[1].
수술적 치료는 정상 피부의 멜라닌세포를 백반증 병변에 이식하여 색소재침착(repigmentation)을 유도하는 것으로, 이식편의 종류에 따라 크게 조직이식술(tissue grafting)과 세포이식술(cellular grafting)로 나뉜다(Table 1). 조직이식술에는 부분층 피부이식술(split-thickness skin grafting), 으깬조직이식술(smashed skin grafting), 흡입물집이식술(suction blister grafting), 펀치이식술(punch grafting)과 미세펀치이식술(micro-punch grafting), 모낭이식술(hair follicle transplantation) 등이 있고, 세포이식에는 비배양 표피세포이식술(noncultured epidermal cell suspension transplantation), 비배양 모낭세포이식술(noncultured follicular cell suspension transplantation), 배양 표피세포이식술(cultured epidermal cell suspension transplantation) 등이 있다. 이중 흡입물집이식술, 펀치이식술, 비배양 표피세포이식술이 기존 치료에 반응이 없는 불응성 백반증의 수술적 치료로 현재 널리 시행되고 있다.
조직이식술
1. 부분층 피부이식술
부분층 피부이식술은 백반증의 치료에 1947년 처음 보고되었다[2]. 부분층 피부이식술은 정상 피부에서 표피와 진피층의 일부를 채취하여 피부 결손 부위에 봉합하는 수술법으로, 본래 일차 봉합으로 회복되지 않는 피부의 결손을 치료하기 위해 발달하였다. 주로 엉덩이나 허벅지를 공여부로 선택하며, 피부절제기(dermatome)를 이용하여 0.125-0.275 mm 두께의 피부이식편을 채취한다. 백반증 부위의 표피를 제거한 후 이식편을 부착하고 1주가량 단단히 고정한다. 하지만, 수술 후 공여부에 영구적인 색소침착과 흉터가 남고, 이식편이 수축하여 수여부의 표면과 피부색이 이질적인 경우가 많아 백반증의 치료를 위해서는 거의 시행되지 않는다.
2. 으깬조직이식술
으깬조직이식술은 부분층 피부이식술의 변형으로 피부이식편을 가위 혹은 면도날로 잘게 썰거나 으깨어 수여부에 넓게 도포한 뒤 고정하는 수술법이다[3]. 같은 크기의 조직으로 좀 더 넓은 병변을 치료할 수 있지만 공여부에 흉터와 색소침착이 남고, 이식 후 피부색이 균일하지 못한 단점이 있다.
3. 흡입물집이식술
흡입물집이식술은 정상 피부에서 흡입기를 통해 흡입물집을 만들어 이를 백반증 병변에 이식하는 수술법이다(Figure 1) [4]. 이는 음압에 의해 표피와 진피의 경계 부위가 정확히 분리되고 멜라닌세포가 물집 쪽(표피)에 위치하는 것에 착안한 방법이다. 주로 아랫배, 허벅지 안쪽, 둔부의 정상 피부를 공여부로 선택하며, 20 mL 주사기의 뒷면을 공여부 피부의 표면에 위치시키고 흡입기를 이용하여 300 mmHg의 음압을 2시간가량 유지시켜 물집을 만든다. 백반증 부위는 냉동요법, 레이저 박피 등으로 표피를 제거한 뒤 흡입물집을 부착하고 5-7일간 고정한다.
흡입물집이식술은 국내외적으로 오랫동안 시행되어온 전통적인 수술법 중 하나로 외래에서 간편히 시행할 수 있으며 흉터 발생의 위험이 적고 일정한 치료효과를 기대할 수 있는 장점이 있다. 하지만, 이식 부위에 색소재침착이 과하게 올라오거나 이식편 주변으로 저색소 테두리(perilesional halo)가 남을 수 있으며, 넓은 병변을 치료하는 경우 면적에 비례하여 많은 수의 흡입물집이 필요한 어려움이 있다.
4. 펀치이식술
펀치이식술이란 1-2 mm 직경의 펀치기구로 공여부에서 원주형의 이식편을 채취하여 백반증 부위로 옮겨 심는 수술법으로 1972년 처음 보고되었다. 하지만 공여부에 흉터가 남고, 이식편이 밀려나와 울퉁불퉁해지는 자갈밭모양(cobblestone appearance) 흉터가 남을 수 있고, 수술면적에 비례하여 수술시간이 길어지기 때문에 그동안 널리 시행되지 못했다.
5. 미세펀치이식술
최근 전동 핸드피스를 이용한 0.8 mm 미세펀치이식술이 개발되어 수술시간을 대폭 줄이고 보다 균일한 치료효과를 얻을 수 있게 되었다. 저자들은 2015년 1월부터 2017년 8월까지 미세펀치이식술로 치료한 불응성 백반증 230례를 분석한 결과, 총 181례(78.7%)에서 성공적인 결과를 확인하였다(Figure 2) [5]. 특히 얼굴과 목의 백반증, 젊은 환자, 분절형 백반증에서 좋은 효과를 보였다. 수술 시간은 병변의 크기에 따라 차이가 있었지만 대체로 30분에서 2시간 이내였으며, 일상생활이 바로 가능했다. 자갈밭모양의 변형은 수술 후 6개월까지 23.4%에서 관찰되었으나, 1년 뒤에는 11.4%로 감소하였다.
미세펀치이식술은 백반증의 수술적 치료 중 외래에서 가장 간단하게 시행할 수 있는 방법으로 어린이나 굴곡진 부위 등 다른 수술법을 적용하기 까다로운 경우에도 시도해볼 수 있다. 또한, 0.5 mm 미세펀치이식술을 활용하면 공여부의 수술 흔적이 거의 남지 않고 수여부의 자갈밭모양 흉터 발생의 위험도 크게 줄어 보다 안전한 시술이 가능하다[6]. 하지만, 노동집약적인 방법의 특성상 넓은 면적을 치료하기에는 어려움이 있으며, 입 주위, 목, 관절 부위와 같이 움직임이 많은 부위는 이식편이 잘 고정되지 않아 자갈밭모양 흉터의 발생위험이 높아 주의를 요한다.
6. 모낭이식술
모낭이식술은 두피나 모발이 많은 부위에서 펀치기구로 모낭단위를 채취하여 백반증 부위에 이식하는 수술법으로 이식된 모낭으로부터 멜라닌세포가 이주하여 색소침착을 유도한다[7]. 특히, 모낭이식술은 공여부의 흉터가 감춰지는 장점이 있으며 모발이 많은 부위의 백반증이나 백모증이 동반된 부위에 시도해 볼 수 있다. 하지만 수술시간이 길고, 모발이 없는 부위의 치료에는 적절치 않다.
세포이식술
1. 비배양 표피세포이식술
세포이식술은 정상 피부에서 분리한 멜라닌세포와 각질형성세포를 세포현탁액의 형태로 백반증 병변에 이식하는 수술법으로 세포배양 여부에 따라 비배양법과 배양법으로 나뉜다. 배양 세포이식술은 아직 시험적으로 시도되고 있는 단계인 반면, 비배양 표피세포이식술은 1992년 처음 보고된 이래 발전을 거듭하여 현재 세계 각지에서 보편적으로 시행되고 있다[8].
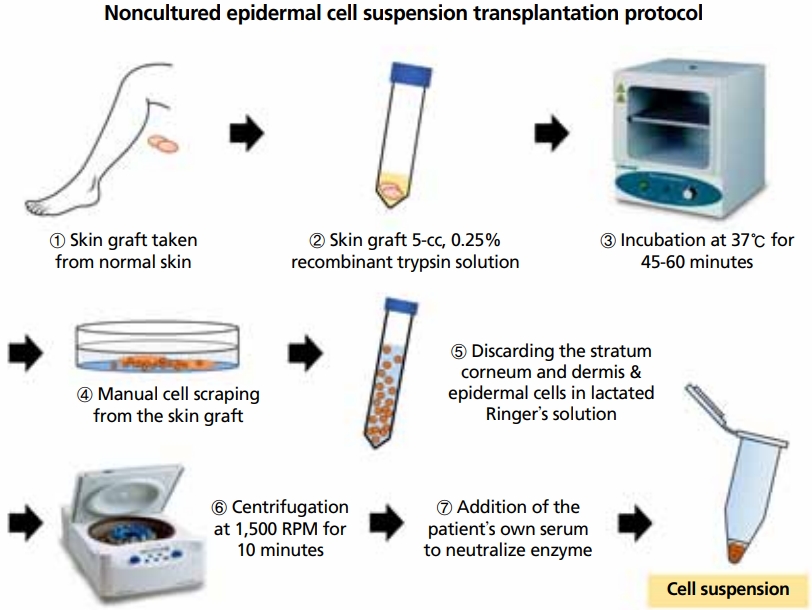
비배양 표피세포이식술은 크게 정상 표피의 채취, 세포 분리, 세포현탁액의 제작, 피부이식의 4단계로 진행된다(Figure 3) [9]. 주로 허벅지 안쪽에서 수술할 면적의 1/5에서 1/10 정도 크기로 공여부를 확보하며 수술용 칼이나 피부절제기 등을 이용하여 표피를 채취한다. 채취한 표피는 트립신(trypsin) 효소를 처리하여 세포 단위로 분리한 뒤 원심분리로 농축하여 세포현탁액을 만든다. 백반증 부위는 레이저 박피 등으로 표피만 얇게 제거한 뒤 세포현탁액을 고르게 도포하고 콜라겐 드레싱 등으로 1주간 밀폐 고정한다.
비배양 표피세포이식술은 4-5시간의 수술시간이 소요되며 원활한 수술을 위해서는 숙련된 팀이 필요하다. 조직이식술이 공여부와 수여부를 1:1로 이식하는데 비해, 비배양 표피세포이식술은 공여부 면적의 5-10배까지 적용할 수 있어 넓은 면적을 한 번에 치료할 수 있는 장점이 있다. 또한, 세포배양 과정을 거치지 않기 때문에 특수한 재료와 설비가 필요하지 않으며 외래에서 당일 시술이 가능하다.
2. 비배양 표피세포이식술의 새로운 시도
비배양 표피세포이식술은 불응성 백반증의 표준수술법으로 수술효과를 개선하기 위해 많은 연구가 이뤄지고 있다. van Geel 등[10]은 세포현탁액의 고정을 위해 점도가 높은 히알루론산(hyaluronic acid)을 첨가하여 치료의 편의성과 수술 결과를 향상시켰다. Esmat 등[11]은 여러 종류의 성장인자를 첨가하여 치료 효과를 높일 수 있음을 보였고, Thakur 등[12]은 진피세포를 추가하였을 때 표피세포 단독보다 멜라닌세포의 생착률이 증가됨을 확인하였다.
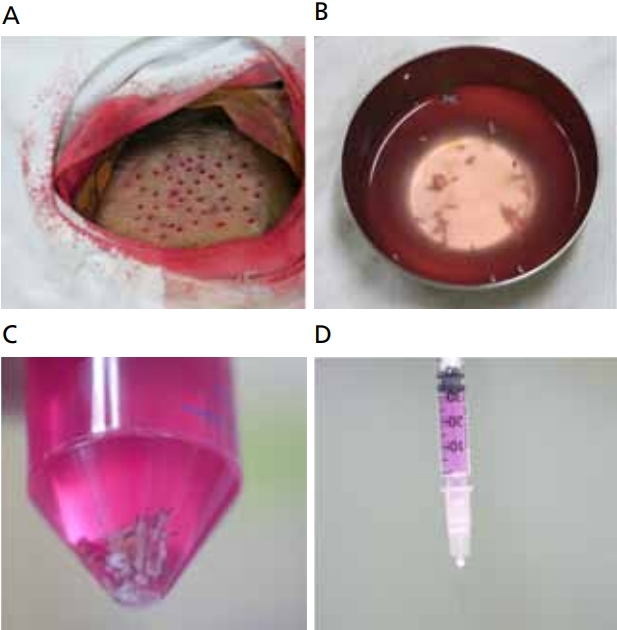
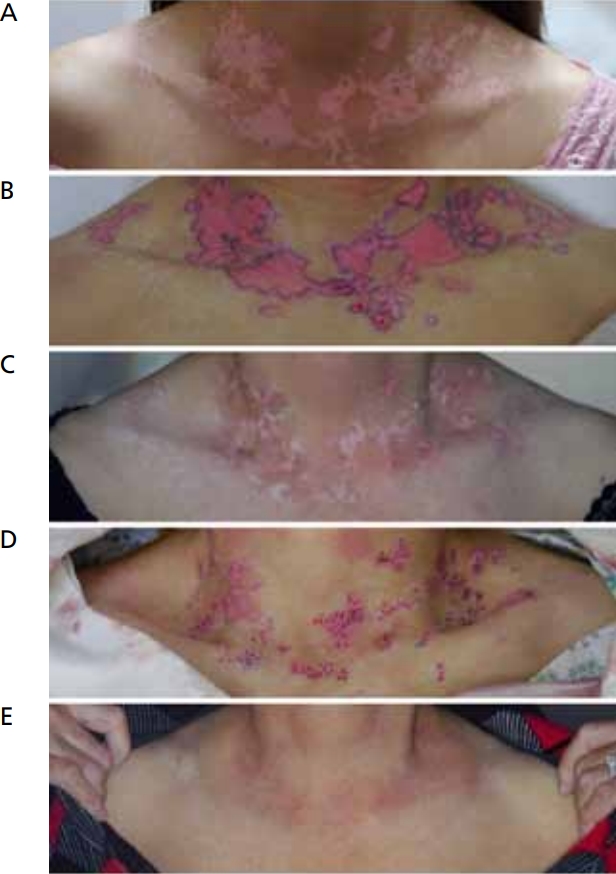
저자들은 비배양 표피세포이식술의 표피 채취 단계에 흡입물집술을 적용하여 공여부 흉터 발생의 위험을 최소화하였다. 흡입물집이식술에서와 같이 음압을 통해 표피를 채취하면 표피와 진피 경계 부위가 정확히 분리되어 진피의 손상을 피할 수 있다[9]. 2015년 7월부터 2020년 8월까지 본원에서 시행한 흡입물집을 이용한 비배양 표피세포이식술 47례를 분석한 결과 37명(78.7%)에서 한번의 시술로 성공적인 결과를 확인하였고 비후성 흉터의 발생은 관찰되지 않았다(Figure 4).
비배양 표피세포이식술은 기존 치료로 호전되지 않는 백반증에 대한 훌륭한 수술적 대안으로 이미 피부과학 교과서에서 백반증의 표준수술법으로 기술되고 있으나, 국내에서는 신의료기술평가에서 불승인되어 환자에게 시행할 수 없는 안타까운 상황이다.
3. 비배양 모낭세포이식술
비배양 모낭세포이식술은 모낭의 겉뿌리싸개(outer root sheath)에 존재하는 멜라닌세포를 분리해 세포현탁액으로 만들어 병변부에 이식하는 방법이다[13]. 겉뿌리싸개에 분포하는 비활동성 멜라닌세포와 멜라닌세포 줄기세포는 정상 상태에서는 멜라닌색소를 합성하지 않지만, 자외선 치료가 이들의 분화와 증식을 유도하여 백반증 병변의 색소재침착을 일으킨다[14].
시술 과정은 모낭단위의 채취, 세포분리, 세포이식의 단계를 거친다. 귀 뒤나 후두부에서 1 mm 펀치기구를 이용하여 모낭단위조직을 채취한 뒤, 트립신 효소를 처리하여 겉뿌리싸개의 멜라닌세포와 줄기세포들을 분리한다. 털줄기(hair shaft) 조직을 제거하고 원심분리를 통해 농축한 세포현탁액을 수여부에 이식한다(Figure 5).
4. 배양 표피세포이식술
보다 넓은 백반증을 치료하기 위해 자가 멜라닌세포와 각질형성세포를 배양하여 이식하는 배양 표피세포이식술이 시도되고 있다. 배양 표피세포이식술은 공여부의 10-40배까지 치료할 수 있으며, 배양된 세포를 보관하여 반복 시술이 가능한 장점이 있다. 배양에는 3주가량의 시간이 필요하며, 실험실적 장비와 기술의 숙련이 필요하다. 현재까지의 보고에 따르면 배양 표피세포이식술은 비배양 표피세포이식술과 유사한 치료효과를 보여주고 있다[17]. 한편, 배양 세포이식술은 세포치료제로 분류되기 때문에 우수 의약품 제조·관리 기준(Good Manufacturing Practice)에 부합하는 설비와 공정을 따라야 한다.
배양된 세포를 생체에 이식하는 경우 가장 큰 문제는 안전성이다. 세포 배양에 사용되는 대표적인 세포 분열 촉진제인 12-tetradecanoylphorbol 13-acetate (TPA)는 발암성에 대한 논란이 있다. 이에 endothelin-1, basic fibroblast growth factor, α-melanocyte-stimulating hormones 등 생체 내 인자들로 TPA를 대체하는 배양법들이 보고되었으며 자가혈청을 이용한 배양법 등 다양한 시도가 이루어지고 있다.[18,19]. 배양 표피세포이식술은 아직 시험적 단계에 있지만 향후 광범위한 난치성 백반증의 환자에 있어 좋은 치료 옵션이 될 것으로 생각된다.
수술적 치료의 고려사항
최근 메타분석에 따르면 한 번의 수술로 치료 성공에 이르는 비율은 수술법의 종류에 관계없이 50-80% 정도였다. 백반증의 수술적 치료법은 어느 것이 더 우월하다고 말할 수는 없으며, 백반증의 부위와 면적, 환자의 나이와 상태, 예상되는 부작용 등을 종합적으로 고려하여 각 환자에게 적합한 수술법을 선택해야 할 것이다. 경우에 따라서는 최상의 결과를 얻기 위해 두 종류 이상의 수술법을 병합하여 시행할 수 있다(Figure 6).
결론
백반증은 오랫동안 치료가 안되는 불치성 혹은 난치성 피부질환으로 여겨져 왔다. 하지만 최근 수술법의 발전으로 치료가 가능한 백반증의 범위가 크게 늘었다. 세계백반증학회의 백반증 치료지침에 따르면 1년 이상의 내과적 치료에도 불구하고 더 이상 호전을 보이지 않는 경우 수술적 치료를 권고하고 있다[21]. 수술적 치료는 더 이상 백반증 치료의 대안이 아니라 표준 치료법의 하나로 자리잡았다.
국내에서는 현재 흡입물집 표피이식술과 미세펀치이식술이 국민건강보험의 혜택을 받고 있으나, 비배양 표피세포이식술은 신의료기술평가의 문턱을 넘지 못하고 있다. 교과서 적으로 표준 수술법으로 간주되는 비배양 표피세포이식술이 국내에서 허용되지 않는 것은 안타까운 일이다. 앞으로 수술이 가능함에도 치료를 포기하는 환자가 없도록 의사와 정부의 적극적인 관심이 필요할 것이다.