서론
류마티스관절염은 관절 주위를 둘러싸고 있는 활막의 염증으로 인해 발생하는 전신성 만성염증질환으로 통증, 기형, 장애, 삶의 질 저하를 일으키고 드물지만 폐, 심장까지 침범할 수 있다. 따라서 류마티스관절염은 고혈압이나 당뇨병처럼 만성적으로 조절해야 하는 질환으로 환자의 순응도가 중요하다. 1990년대 후반부터 메토트렉세이트(methotrexate)는 류마티스관절염의 질병조절 항류마티스약물 (disease-modifying antirheumatic drugs, DMARDs) 중 가장 중요한 약으로 인식되어 사용되었다[1]. 류마티스관절염의 병태생리학적 기전이 새롭게 밝혀짐에 따라 생물학적 DMARDs와 같은 새로운 약물이 도입되었다. 종양괴사인자억제제, CD20세포의 B세포 억제제, interleukin (IL)-6 억제제 등의 새로운 약제들이 여기에 속한다[2]. 그러나 생물학적 DMARDs는 지속적으로 반복해서 주사로 투여받아야 하는 단점이 있었다. 이 논문에서 기술하는 최신 약물인 야누스인산화효소(Janus kinase, JAK) 억제제는, 난치성 류마티스관절염에 치료제의 혁신을 일으킨 새로운 종류의 경구치료제이다[3].
류마티스관절염의 새로운 치료제: JAK 억제제
JAK 계열은 JAK1, JAK2, JAK3, tyrosine kinase 2로 구성되어 있다. 많은 사이토카인 수용체(IL-4, IL-6, IL-10, IL-12, IL-23, granulocyte-macrophage colony-stimulating factor 등)가 본질적인 인산화효소 활성이 결여되어 JAK와 같은 tyrosine kinase에 의존하여 세포 외 환경에서 핵으로 신호를 전송하게 된다[2,4]. 즉, 사이토카인이 세포표면수용체와 결합하면 수용체 관련 JAK가 근접, 활성화되어 인산화된다. 활성화된 JAK는 STAT(signal transducers and activators of transcription)를 활성화할 수 있으며 면역세포의 분열, 생존, 활성화에 관련된 유전자의 전사를 허용한다[5]. 이들은 두 개의 kinase domain을 가지는데 진정한 kinase와 pseudo-kinase로 구성되어 로마의 신인 야누스로부터 이름이 유래되었다. 다양한 JAK 조합을 통한 신호전달의 생물학적 중요성을 Table 1에 기술하였다[4]. 현재 다양한 JAK 억제제들이 상용되고 Table 2는 우리나라, 미국, 유럽, 그리고 일본에서 승인된 시기이다[2].
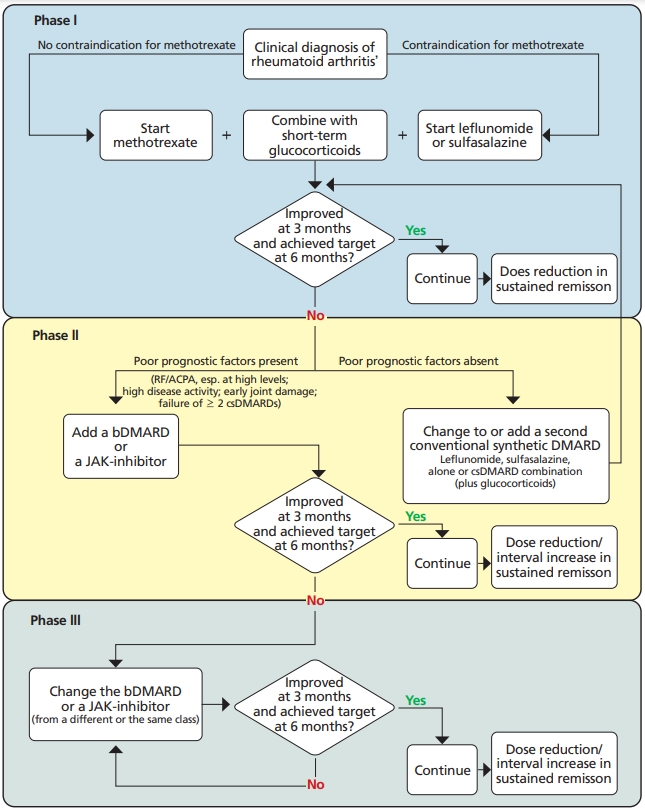
JAK 억제제가 메토트렉세이트에 반응하지 않은 류마티스관절염 환자에서 상당히 높은 반응률을 보여주는 연구결과를 보였고, 이에 따라 2019년 갱신된 EULAR (European Alliance of Associations for Rheumatology) 가이드라인에서 이를 반영하여 메토트렉세이트 및 스테로이드, 합성 항류마티스제제 치료에도 불구하고 3개월 후 호전이 없거나 6개월 후 치료목표에 도달하지 않는 환자군에서 나쁜 예후 인자가 있을 경우 생물학적 항류마티스제제 또는 표적치료제로서 JAK 억제제를 이차 치료제로 사용하도록 권고하고 있다(Figure 1) [6].
류마티스관절염 환자에서 JAK 억제제 치료로 가장 자주 보고되는 부작용은 감염이다. 호흡기, 하기도 및 요로 감염과 같은 일반적인 감염의 발생률은 일반 인구에 비해 높지만, 종양괴사인자 억제제, 리툭시맙 및 토실리주맙 같은 생물학적 항류마티스제제를 사용할 때 발생률과 비교 시 심각한 감염의 위험도는 비슷한 것으로 보고되었다[7,8]. 이 외에도 대상포진, 혈구감소증, 정맥혈전증 등이 부작용으로 나타날 수 있다[2]. 종양괴사인자 억제제를 사용하기 전 잠복성결핵 감염에 대한 검사 및 치료를 하는 것처럼 JAK 억제제도 사용하기 전 스크리닝 및 치료전략이 권장된다[9].