약물유발 사이질폐질환의 진단과 치료
Diagnosis and treatment of drug-induced interstitial lung disease
Article information

Trans Abstract
Drug-induced interstitial lung disease (DILD) is a group of adverse drug reactions that is rare but fatally toxic. Pulmonary toxicity causes inflammation and subsequent interstitial fibrosis. As novel drugs with a variety of purposes are introduced into the medical field, the number of culprit medications that are suspected to cause lung complications is accordingly increasing. In this review, DILD will be discussed from several aspects such as causality by numerous drugs, check points for a timely diagnosis, alongside some contemporary treatment options. The exact mechanism of DILD has not been elucidated, and a useful clinical, radiological, or pathological confirmation process is still lacking. Common drugs which casue DILD include bleomycin, amiodarone, epidermal growth factor receptor-targeted agents, and immune checkpoint inhibitors. Diagnosis is based on a suspicious drug administration history, somewhat inconsistent clinical symptoms and signs, radiological hints, and histopathological assistance, together with the exclusion of other lung-injuring etiologies. Cessation of the suspected drug, meticulous corticosteroid usage, and ancillary supportive management are the mainstay therapeutic strategy for DILD. Most cases of DILD respond to these countermeasures and reductions, but in some cases the fibrotic process worsens, leading to irreversible sequelae on the affected lung.
서론
인체에게 사용하는 약물은 다양한 목적이 있어 이를 만족하기 위한 적절한 용량, 투여경로, 투여방법 등이 제시되어 있으며, 약물 투여 후 효과나 부작용 등을 평가하여 보완함으로써 약물의 사용목적을 극대화하고 있다. 이때 예기치 못한 부작용이 발생하는 경우 최초의 투여목적에 반하는 효과가 초래되어 환자에게 치명적인 결과를 낳을 수 있다. 특히 약물에 의한 심각한 부작용은 임상가들이 발생과정, 임상양상, 치료 및 예방 방법을 숙지하여 환자의 생명과 건강상태를 해치지 않도록 유의해야 한다.
약물의 다양한 부작용은 인체의 각 장기에서 나타날 수 있으며, 이 중 폐는 고유한 특성이 있다. 폐는 접촉면적이 매우 넓어 다양한 약물 독성의 표적이 될 수 있다. 어떤 약물의 특정 성분은 폐에서 대사되어 독성을 얻기도 한다. 의도하지 않은 독성작용이 폐조직 고유의 기능과 연관되어 나타날 수도 있으며, 반대로 전신적 부작용의 한 양상으로 폐조직이 손상되기도 한다[1]. 폐를 구성하는 조직은 기도, 폐사이질, 종격, 흉막, 폐혈관, 신경·근육 등이 있으며 이들 모두 약물에 의한 폐손상을 입을 수 있다. 폐의 실질에 이환되는 각종 질환을 통틀어 사이질폐질환(interstitial lung diseases, ILD)이라 부르며, ILD의 다양한 원인 중 약물은 드물지만 중요한 유발요인이다. 인체에 투여된 약물에 의해 발생하는 약물유발 사이질폐질환(drug-induced interstitial lung diseases, DILD)은 약물에 의한 폐손상 중에서 가장 흔한 질환이다[1]. DILD는 다양한 질환에 대한 약물 투여 후에 발생하며, 발생기전과 임상양상이 일정치 않고 진단과 치료에 있어 어려움이 따른다. 특히 폐실질의 염증이 해소되지 않는 경우 비가역적인 섬유화로 진행되며 심각한 후유증을 남길 수 있다. 또한 다른 합병증의 발생으로 목숨을 잃는 경우도 있어 더욱 주의가 필요하다.
이 논문에서는 최신 문헌을 토대로 임상적 특징을 중심으로 전형적인 사례를 간단히 서술하면서 DILD의 역학, 위험인자, 진단 및 치료 등을 소개하여, 임상에서 DILD가 의심되는 상황을 접했을 때 효율적으로 대처하는 데 있어 도움이 되는 최신 지식을 공유하고자 한다.
증례
57세 남성 환자가 발열을 주소로 의뢰되었다. 3년 전 직장암이 진단되어 저위전방절제술(low anterior resection)을 실시하고 경과 관찰 중, 혈중 암배아항원(carcinoembryonic antigen)이 상승하고 흉부방사선검사 및 흉부 컴퓨터단층촬영(computed tomography, CT)에서 다발성의 전이성 폐결절을 의심케 하는 소견이 관찰되어 FOLFOX 항암화학요법을 개시하였다. Oxaliplatin 85 mg/m2을 정주 투여한 뒤, 5-fluorouracil 400 mg/m2 1회 정주에 이어 5-fluorouracil 600 mg/m2을 22시간 동안 투여하였으며 이를 2주마다 반복하였다. 4차 투여 때부터 oxaliplatin 투여 도중 발열 소견이 나타났으나 자연소실되어 나머지 약물로 치료를 마쳤다. 비슷한 과정을 반복하던 중 9차 투여에서는 발열 소견 및 추적검사한 고해상도CT (high resolution CT, HRCT)에서 새로운 이상 소견이 나타났다. 환자는 고혈압, 당뇨병 등의 기저질환은 없었고 열감 및 경미한 호흡곤란을 호소하였고, 체온은 38.6℃, 흉부 청진에서 양폐야에 거친 호흡음과 악설음이 들렸다. 흉부 CT에서 다발성의 흉막하 폐경화, 결절성의 간유리음영(ground glass opacity)이 새로이 관찰되었다(Figure 1A) [2]. 급성폐렴 혹은 DILD를 의심하여, 기관지내시경검사 및 비디오보조흉강경수술로 조직 진단을 시도하였다. 기관지 폐포 세척액 검사에서 특별한 이상 소견은 없었으며, 폐 우중엽 및 우하엽에서 얻은 조직에서 세기관지 및 폐포를 메우고 있는 기질화마개(organizing plug)가 관찰되어, 기질화폐렴(organizing pneumonia)의 병리진단이 확인되었다(Figure 1B) [2]. 이상의 소견을 종합하여 oxaliplatin에 의해 유발된 DILD를 진단하였다. 진단 후 진행 중이던 항암화학요법을 중단하였으며 코티코스테로이드 치료(prednisolone, 1 mg/kg/day)를 시작하였고, 추적관찰 흉부 CT에서 양측 폐의 흉막하 및 주변부에 보였던 간유리음영이 호전되었음을 확인하였다.
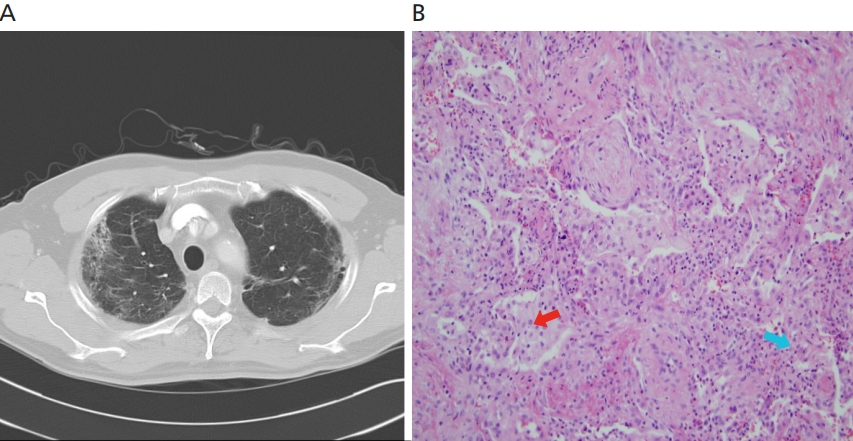
Oxaliplatin-induced interstitial lung disease. Bilateral, patchy consolidations along peripheral lungs was noticed on chest computed tomography scan (A) and histologic finding showed intraluminal organizing fibrous plugs suggestive of organizing pneumonia pattern (B, H&E stain, ×400). Reproduced from Lee EJ, et al. Med Princ Pract 2012;21:89-92, with permission of S. Karger AG, Basel [2].
역학
DILD를 포함하여 약물에 의한 각종 폐질환의 정확한 발병률은 아직 명확하지 않다. 약물유발 폐질환은 전 세계적으로 과소 진단된 것으로 평가받고 있다[1]. 미국에서 약물에 의한 폐질환의 보고 사례는 실제 증례의 5%도 안되는 것으로 추측되고 있다[3]. 이 중 DILD는 흔치 않은 사례와 까다로운 진단과정, 보고체계 내에서의 오류 등으로 역학자료가 부정확한 것으로 보인다. 최근 다수의 연구논문을 분석한 발표에 따르면 각 유발 약물에 의한 DILD의 발병률은 1% 미만에서 60%까지 그 폭이 매우 넓었다. 이는 취합하여 분석한 논문들이 일으키는 오류에 의한 것으로 보인다[4].
유병률의 경우 몇 개의 ILD 코호트를 분석한 결과 2.6%에서 5%인 것으로 나타났다[5]. 연구논문의 특정 국가 편중도 있어, 국가 차원의 DILD 사례 수집 및 등록 사업이 활발한 일본의 유병률이 구미의 것보다 높은 것으로 분석되었다[6]. 따라서 이는 인종 차이에 의한 것이라기 보다는 얼마나 적극적으로 보고하느냐에 따른 것으로 보인다[4].
현재까지 350여 종의 약물들이 DILD를 일으키는 것으로 알려져 있으며 대표적인 약물들을 Table 1에 정리하였다.

Some etiologic drugs inducing drug-induced interstitial lung disease
위험인자
다양한 약동학을 이용하며 광범위한 목적 및 질환에 대해 투여하는 약물들의 DILD에 대한 위험인자 역시 다양하다. 이 중 몇몇 인자들은 공통적으로 관찰되는 경향이 있어 이에 대한 이해가 필요하다.
고령일수록 DILD의 위험이 증가하는 약물들이 있다. Bleomycin, gemcitabine, 상피세포성장인자수용체(epidermal growth factor receptor, EGFR) 표적치료제, methotrexate, amiodarone, nitrofurantoin, leflunomide 등이 대표적이다. 나이가 어린 청소년기도 위험인자이나, 그보다는 고령의 환자가 더 취약하며 이는 신장 및 간의 기능저하 및 전반적인 대사기능의 변화에서 비롯되는 것으로 보인다[1]. 성별에 따른 차이는 크지 않은 것으로 알려져 있다. 인종 간의 차이가 있다는 보고들이 있었으나[7], 대상 약물인 gefitinib, leflunomide, tacrolimus 등의 약물들의 부작용이 특정 국가(일본)에서 유독 보고사례가 많았던 것으로 보아 질병 등록 상의 문제나 부작용 사례의 자율적인 보고 등이 영향을 미쳤을 것으로 보이며, 인종 간의 차이는 크지 않을 것으로 보인다.
용량에 따라 그 부작용이 더 심하게 나타나는 약물들이 있다. 투여한 누적 용량에 따라 부작용이 심해지는 약물로는 amiodarone, bleomycin, bis-chloroethylnitrosourea 등이 있다. Bleomycin의 경우 cisplatin이나 gemcitabine 등의 약물과 병합 투여했을 때 bleomycin에 의해 유발되는 DILD가 더욱 심한 임상양상을 보인다. DILD 발생 이전에 항암화학 요법 약물을 투여한 과거력이 폐암 환자에서 gemcitabine에 의한 DILD 발생에 위험인자로 작용하기도 하나[8], 반대로 gemcitabine과 같은 계열 혹은 동일한 약물로 항암화학요법을 실시하면 DILD가 오히려 덜 발생하기도 한다는 보고도 있다[9]. DILD 발생 이전에 방사선요법을 시행 받은 폐암 환자는 DILD 발생이 잦다[10].
DILD가 발생한 환자에게 기존의 폐질환은 위험인자의 하나로 작용할 수 있다. ILD는 다양한 약물에 있어 DILD의 중요한 위험인자이다[11,12]. 몇몇 암은 ILD가 기저질환으로 있는 경우 항암화학요법에 의한 DILD의 발병률이 높을 것으로 추정된다[13,14]. 당뇨병, 과도한 음주, 신장기능 이상 등이 잠재적인 위험인자로 거론된다[10,15]. 그 밖에 cytochrome P450 CYP enzyme polymorphism, 특정 HLA allele의 변이 등도 DILD 발생의 위험을 높인다[4].
발병기전
DILD의 발병기전은 크게 네 가지로 분류되는데, 산화제 손상(예: nitrofurantoin의 장기 투여), 직접적인 세포독성 효과, phospholipid의 세포 내 축적(예: amiodarone), 면역 매개 손상(예: 약물유발 루푸스)으로 구분된다[16]. 특정 약물들이 인체의 다른 장기에 비해 폐에 특별히 독성을 보이는 이유는 어떤 약물은 다른 장기보다는 폐에서 높은 세포 또는 조직 농도에 도달하기도 하며, 폐에서 특정한 수준 또는 양상으로 생활성(bioactivation)이 일어나거나, 그러한 생활성의 결과가 폐에서만 발생하기 때문이기도 하다[17].
그럼에도 DILD의 정확한 발생기전은 여전히 명확하지 않다. 가능성이 있는 기전은 폐포에의 직접적인 약물 독성, 그리고 원인 약물에 대한 면역학적 반응 등이 거론되고 있다[12]. 폐독성의 시작은 약물에 의한 폐손상에서 비롯되어 폐포염과 부종이 일어나며, 이어서 폐실질의 손상을 복구하고 더 이상의 염증을 차단하려는 반응이 이어진다. 급성손상은 만성염증으로 진행하기도 하며, 결국 섬유화에 이르러 폐조직 고유의 기능인 가스교환능력이 손상되기도 한다. 또한 기관지 폐포 세척 검사 검체분석에서 림프구 증가증이 있어, 면역학적 기전도 DILD 발병에 관여할 것으로 추정하고 있다.
DILD를 일으키는 약물
1. Bleomycin
생식세포종, 호지킨림프종(Hodgkin’s tumor) 등의 치료에 쓰이는 약물로, ILD의 동물 실험에서 인위적으로 ILD를 유도하는 약물로도 흔하게 사용하고 있다[18,19]. 이 약물은 표적 암세포에 진입해서 DNA에 결합하여 약효를 발휘하는데, 이 과정에 산소라디칼(oxygen radical)이 관여하는 것으로 알려져 있으며 고농도 산소 투여나 방사선치료가 bleomycin의 독성을 증가시키는 것으로도 추정된다[20]. 사이질폐렴 및 섬유화가 가장 흔한 병리적 특징이며, 이는 HRCT에서 간유리음영, 국소적인 폐경화 및 폐 하단부에 주로 분포하는 불규칙한 선상의 망상 음영이 주로 관찰된다[21]. 드물게 과민반응으로 양측성의 간유리음영과 경계가 불분명한 중심소엽성 결절이 HRCT에서 보이기도 한다(Figure 2) [19].

Bleomycin-induced interstitial lung disease. Compared to control group(A and C), hyperplasia of cuboidal-shaped club cells and alveolar epithelial cells, septal thickening, enlarged alveoli (open arrows), influx of inflammatory cells (solid arrow) and extensive fibrosis were observed in the bleomycin-treated lung (B and D). TB, terminal bronchiole; AD, alveolar duct. (A,B) H&E,×400. (C,D) Masson’s trichrome staining,×400. Reproduced from Lee SH, et al. Exp Lung Res 2014;40:117-125, with permission of Taylor & Francis [19].
치료는 bleomycin의 투여 중단과 선택적인 코티코스테로이드 투여이며, 특히 고농도의 산소요법이나 동시적 방사선 요법은 상태를 더욱 악화시킬 수 있어 주의해야 한다. 또한이 약물은 신장으로 배설되므로 치료 중 신장기능의 저하에 유의해야 한다.
2. Amiodarone
부정맥을 치료하는데 사용하는 amiodarone은 여러 가지 부작용이 있으나 ILD가 가장 심각한 부작용이며, 그 중 6%의 환자에게는 치명적이다[16]. 약물의 독성이 누적 용량에 비례하는 독특한 특성도 있다.
HRCT에서 관찰되는 소견은 만성사이질폐렴, 기질화폐렴, 급성호흡곤란증후군, 폐결절 등으로 다양한 편으로 특징적인 병리 소견은 Figure 3에 제시하였다[20]. 증상, 폐기능검사, 병리검사 등으로 확정 진단하기는 쉽지 않으며 배제 진단으로 질환을 파악할 수 있다. 치료는 amiodarone의 투여 중단 및 코티코스테로이드 치료이다. 이러한 치료전략에 환자는 일정치 않은 반응을 보이는데, 코티코스테로이드의 투여를 6개월 이상 지속해야 하는 경우도 있다.
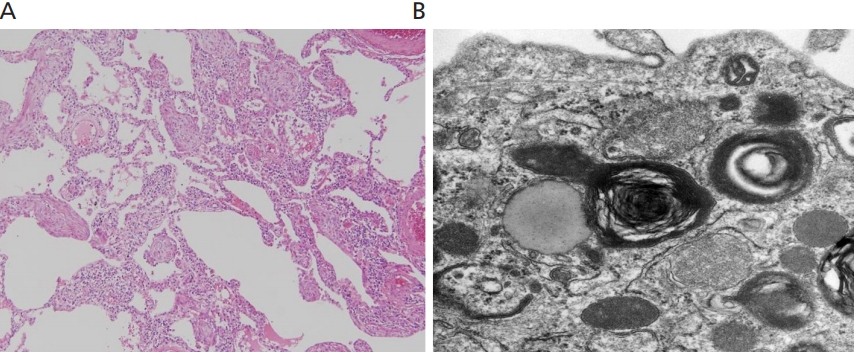
Amiodarone-induced interstitial lung disease. Video-assisted thoracoscopic surgical biopsy showed an intraluminal organizing fibrous plug in the alveoli, consistent with an organizing pneumonia pattern (A, H&E stain, ×40). Electron microscopic examination reveals macrophage with lamellated cytoplasmic inclusions suggestive of amiodarone-induced endogenous lipid pneumonia(B). Informed consent for publication of the clinical images was obtained from the patient.
3. EGFR-targeted agents: gefitinib, erlotinib, osimertinib, cetuximab, panitumumab
EGFR의 타이로신인산화효소(tyrosine kinase)를 선택적으로 억제하는 gefitinib, erlotinib, osimertinib 등은 진행된 비소세포폐암, 유방암, 대장암 등에 쓰인다. 급성사이질폐렴이 약 1% 내외로 발생하며 사망률은 22.8%에 이르고 있다[22]. 최근 연구에 따르면 두 약물은 DILD 유발 약물의 투여와 발생 사이의 기간이 4주 미만으로 상대적으로 짧은 것으로 알려져 있어, 약물 투여 후에 주의 깊은 관찰이 필요하다[23]. CT에서 광범위한 간유리음영과 다발성 경화 소견이 관찰되며, 병리조직검사는 폐포의 손상, 사이질염증, 기질화폐렴 등의 소견이 보일 수 있다.
Cetuximab과 panitumumab은 EGFR을 차단함으로써 항암효과를 발휘하는 단일클론항체(monoclonal antibody) 약물들로, 흔치 않게 DILD를 일으킨다. 일본의 후향적 연구에 따르면 발병률은 각각 1.2% [24]와 1.3% [25]로 나타났다. 때로는 치명적일 수 있어 의심되는 경우 약물을 끊고 코티코스테로이드 투여를 고려해야 한다.
Figure 4는 비소세포폐암의 치료제로 최근에 미국 식품의약청에서 사용이 승인된 osimertinib에 의한 DILD 환자의 흉부방사선검사 소견으로, 원인 약물 중단 및 코티코스테로이드 투여로 호전되는 것을 확인할 수 있다.
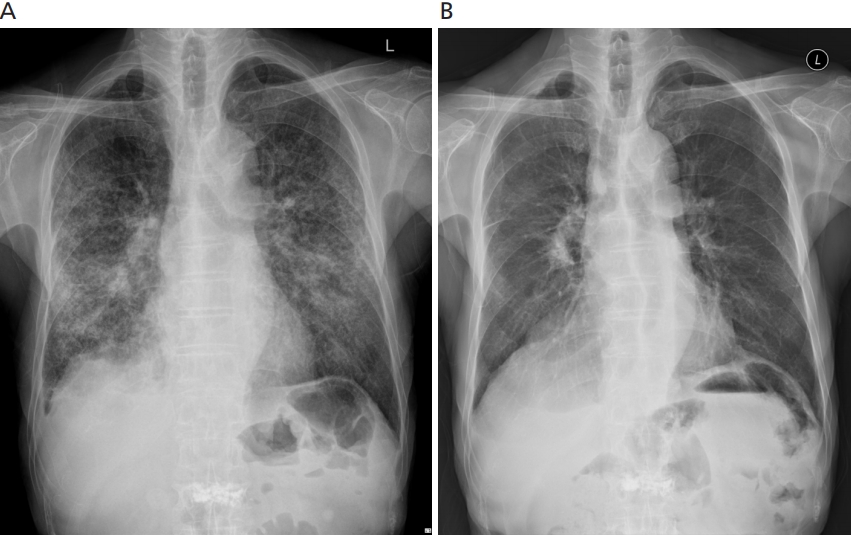
Osimertinib-induced interstitial lung disease. Chest X-ray on Osimertinib showed bilateral increased opacity(Left). After corticosteroid treatment along with Osimertinib discontinuation, chest X-ray showed improvement(Right). Informed consent for publication of the clinical images was obtained from the patient.
4. Immune checkpoint inhibitors: nivolumab, pembrolizumab, atezolizumab, durvalumab
면역관문억제제(immune checkpoint inhibitor)는 암세포와 T세포의 결합 부위에 결합, 암세포가 T세포의 면역 공격을 회피하지 못하도록 함으로써 항암효과를 발휘한다. 전이된 흑색종, 비소세포폐암, 호지킨림프종 등에서 효과를 보고 있으며, programmed cell death-1 (PD-1)에 대한 단일클론항체인 nivolumab, pembrolizumab 등과 programmed cell death-ligand 1 (PD-L1)에 대한 단일클론항체인 atezolizumab, avelumab, durvalumab 등이 이에 속한다. DILD의 발병률은 PD-1 억제제는 3.6%, PD-L1 억제제는 1.1%로 보고되고 있다[9,26]. 일반적으로 PD-1 억제제인 nivolumab, pembrolizumab들이 PD-L1 억제제보다 발병률, 심각성, 치명률 등이 높아 DILD 관련 치명률이 8%에 이른다[4]. 암세포의 표면에 있는 면역관문 분자들을 억제함으로써 암세포에 대한 면역반응 및 암세포의 사멸을 유도하는 약물의 항암기전을 고려했을 때, 면역관문억제제에 의한 DILD는 면역세포의 활성화에 따른 면역계 부작용으로 추정하고 있다[27]. 이에 코티코스테로이드의 시의 적절한 투여가 면역관문억제제에 의한 DILD의 치료에 중요할 것으로 보인다.
병리학적 소견
전술한 것과 같이 DILD는 ILD 질환군의 범주에 포함되는 하부 집단이므로, 본질적으로는 ILD에서 볼 수 있는 병리 소견과 대체로 일치하는 편이다. ILD는 2002년에 미국흉부학회/유럽호흡기학회(American Thoracic Society/European Respiratory Society, ATS/ERS)에서 공동으로 정립한 분류체계에 의거, 조직병리에서 관찰되는 패턴을 바탕으로 임상-영상의학-병리학적 진단으로 정의하여 적용하고 있는데[28], ATS/ERS 분류체계 하에서 DILD 환자에서 볼 수 있는 대표적인 병리 소견들을 소개하고자 한다.
기질화폐렴 패턴은 폐포관과 폐포 내의 기질화가 특징이며, 이때 세기관지도 기질화가 동반될 수 있다. 이러한 병리 소견은 군데군데 분포하는 것이 일반적이며 폐조직 구조 자체는 보존되어 있다.
비특이적 사이질폐렴(non-specific interstitial pneumonia, NSIP) 패턴은 폐포벽 염증 또는 섬유화가 기본 소견이며 기질화폐렴 패턴에서 보이는 폐포 내 기질화는 흔하지 않다. 병리 소견은 전체 폐에 균일하게 분포하고 있으며 폐사이질에는 만성염증 반응이 관찰된다.
광범위폐포손상(diffuse alveolar damage, DAD) 패턴은 ILD 중에서 급격한 결과를 거치는 급성사이질폐렴이나 급성호흡곤란증후군에서 관찰할 수 있는 소견이다. 광범위한 범위에 걸쳐 일어나며 부종, 유리질막(hyaline membrane), 폐사이질의 급성 염증 소견들이 시간이 점차 지나면서 폐포격벽(alveolar septum)의 섬유화 및 과립허파꽈리세포(type II pneumocyte)의 증식으로 발전한다.
통상간질성폐렴(usual interstitial pneumonia) 패턴은 폐조직 구조의 붕괴 소견, 벌집 모양(honeycombing)이 동반된 섬유화, 섬유아세포가 변연부를 주로 침범하는 특징 등이 있다.
영상의학적 소견과 특징
일반 흉부방사선검사에서는 양쪽 혹은 한쪽의 폐침윤 소견이 DILD의 첫 소견일 수 있으나 대부분의 경우 별다른 이상 소견이 없다[29]. HRCT는 ILD를 진단하는데 있어 민감도가 높아 유용한 검사이다. 하지만 DILD를 진단하는데 있어 진단적 가치는 낮다. 즉 원인 약물을 밝히는 데는 비특이적인 한계를 드러내는데, 이는 DILD 환자의 CT에서 관찰되는 폐실질의 변화는 ILD의 소견과 거의 차이가 없기 때문이다. DILD의 경우 CT에서 관찰되는 소견은 조직병리 소견과 항상 일치하지는 않는다. 소규모의 전향적 연구에서 42명의 DILD 환자를 대상으로 기관지경유폐생검(transbronchial lung biopsy) 또는 기관지 폐포 세척액 검사를 실시한 결과 전체 진단 일치율은 67%였다[30]. 따라서 CT에서의 소견만으로 환자의 예후를 예측하는 것 역시 제한이 따른다[31]. 단, DILD 환자에서 DAD가 있는 경우 CT에서 관찰되는 DAD의 소견과 일치도가 매우 높으며[32], 이는 높은 치명률로 이어지는 것으로 확인되었다[33].
DILD의 가장 흔한 CT 소견은 결절성 간유리음영이며, 양폐야의 말단부, 기저부에 양측성으로도 침범하며 폐경화 소견을 동반하기도 한다. ILD의 ATS/ERS 분류에 따르면 DILD의 HRCT 소견은 기질화폐렴을 연상케 하는 사례가 가장 흔했으며, 이어서 NSIP와 과민성폐렴과 유사한 소견을 보이는 증례가 많았다[30,33-35]. 기질화폐렴은 말단부에 띠모양 폐경화(bandlike consolidation) 및 공기기관지조영상(air bronchogram)이 주된 CT 소견이다. NSIP는 하엽에 분포하는 간유리음영 및 심한 견인성 기관지확장증이 CT에서 흔히 관찰된다. 과민성폐렴의 영상의학적 특징을 보이는 DILD 환자의 CT에서는 중심소엽성 결절 및 모자이크형 공기 걸림(mosaic air trapping) 등이 관찰되어 진단에 도움을 얻을 수 있다[32].
CT를 활용한 DILD의 진단은 여러 측면에서 어려움이 따른다. 동일 약물에 의한 DILD는 매우 다양한 것으로 보고되고 있다. 일례로 amiodarone에 의한 DILD의 CT 소견이 NSIP, DAD, 기질화폐렴 패턴 등 여러 가지 양상으로 나타나 진단에 혼선을 준다. 반대로 특정한 CT 소견은 수많은 약물에 의한 DILD들에서 관찰되고 있다[36]. 또한 면역 억제 상태에서 발생하는 각종 비특이적 감염성 폐질환 환자나 결체조직 관련 ILD 환자에 DILD가 합병되었을 때 CT 소견 해석의 어려움은 더욱 크다.
정량적 CT 분석, positron emission tomography 및 자기공명영상(magnetic resonance imaging, MRI) 검사(hyperpolarized 129Xe MRI [37], oxygen-enhanced MRI [38], dynamic contrast-enhanced MRI 등)들이 폐의 구조와 기능을 더욱 특징적으로 묘사할 수 있어 DILD의 진단에 특화하여 이용할 수 있을 것으로 기대되고 있다.
진단
약물에 의한 폐손상은 담당 의사의 주의 깊은 관찰과 의심에서 출발한다. 원인으로 추정되는 약물에의 노출 과거력이 중요하며, 필요시 시행된 조직병리진단을 확인하고 다른 원인으로 인한 폐손상 가능성을 배제해야 한다. 특히 항암화학요법 약물에 의한 DILD는 단일의 질병 특유의 진단검사나 조직병리진단은 없는 것이 현실이다. Lee 등[2]의 연구에서 보듯, 유발 약물의 투여와 DILD의 증상 발현 사이에서 일정한 시차를 수반하는 인과관계를 임상가가 유추할 수 있고, 환자의 자각증상이나 신체활력 징후 혹은 각종 검사에서 ILD가 의심 또는 진단되며, 유발 의심 약물을 중단하여 증상이 호전되고 검사소견이 개선되는 등을 확인함으로써 진단을 굳힐 수 있다. 이에 못지 않게 중요한 것이 급성질환, 특히 감염성질환에 의한 증상 및 징후인지를 감별하는 것으로, 이는 감염질환이 아닌 것으로 오인하고 코티코스테로이드 등의 약물로 치료를 시도했을 때 오히려 환자상태의 급격한 악화를 초래할 수 있다는 점에서 주의가 필요하다.
치료 및 예후
DILD 환자의 치료목적은 염증반응을 억제하고 조직의 섬유화 진행을 늦추는 것이다[1]. DILD 치료의 첫 걸음은 의심되는 약물을 즉각 중단하는 것이다. 약물 투여의 최초 목적과 효과보다 약물의 부작용이 더 심각할 경우 바로 중단해야한다. 실제로 부정맥을 조절할 수 있는 유일한 약물로 판단되어 amiodarone 투여를 중단하지 못한 채 DILD의 치료를 위한 코티코스테로이드 투여와 함께 계속 복용하게 하는 사례가 많은 실정이다[39].
코티코스테로이드는 DILD의 치료에서 가장 흔히 동원하고 있다. 원인 약물의 투여를 중단했음에도 경과가 악화하는 경우 사용을 고려한다. 그러나 최근까지 보고된 코티코스테로이드의 효능은 연구결과에 따라 상이하다. 저자들의 검색 결과 전향적 임상연구는 아직까지 시행된 바 없으며 후향적 연구 역시 크고 작은 오류가 있는 실정이어서, 실제 임상현장에서는 더 심각한 증례나 HRCT 소견이 불량한 경우에 코티코스테로이드를 더 자주 투여하는 경향을 보이고 있다[4]. 또한 폐섬유화의 정도가 심한 경우 코티코스테로이드의 효과는 없으며, 원인 약물을 끊더라도 질병이 계속 악화할 수 있다[1]. 그 외에 저산소증이 관찰되는 경우 산소를 공급하며 환자의 상태가 악화하는 경우 기계호흡 등을 요하는 호흡부전으로 진행할 수 있다.
DILD의 예후는 초기 임상소견의 심각성이나 기저질환의 중증도보다는 점차 진행할 수 있는 폐섬유화의 정도와 관련이 깊다[1]. 적절한 치료로 DILD는 완전한 회복이 가능한 질환이다. 그러나 경과가 나빠져 호흡부전, 다발성장기손상, 그리고 코티코스테로이드 약물의 부작용 등으로 사망하는 경우도 적지 않다[4]. 각종 암 환자의 DILD 사망률은 14%에서 51.3%였으며 비암성 질환자의 경우 최대 41%까지 사망하였다.
결론
DILD는 다양한 목적으로 투여한 약물에 의해 발생하는 약물유발 폐질환이며, 일반적으로 심각한 양상 및 결과를 초래하는 이상반응이다. 질환의 경과는 다양한 편으로 완치되는 사례도 있으나 섬유화가 진행되어 만성화되는 환자도 있다. 진단은 원인 약물과 이환의 인과관계를 파악하고 확인하는 것이 가장 중요하며, 보조적으로 영상의학적 기법과 조직병리학적 진단이 이용된다. 치료는 원인 약물의 중단과 보존적 치료, 심각한 상황에 처한 경우 코티코스테로이드를 투여한다.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
References
Peer Reviewers’ Commentary
이 논문은 약물 사용 중 경험할 수 있는 합병증의 하나인 약물유발 사이질폐질환의 진단과 치료에 대한 최신 지식을 정리하여 소개하고 있다. 흔히 경험할 수 있는 증례와 역학, 위험인자, 발병기전, 대표적 원인 약물들과 함께, 약물유발 사이질폐질환의 영상소견, 진단 및 치료에 대해 자세히 설명해 주고 있다. 약물유발 사이질폐질환은 약물 사용 중 드물지 않게 경험하고, 원인 약물의 중단 및 스테로이드제 사용으로 호전되기도 하나, 치료에 반응하지 않고 섬유화가 진행되어 치명적인 가능성도 있어 주의가 필요하다. 최근 면역항암제 등 새로 개발된 약물 사용의 증가로 이러한 합병증에 대한 의심과 진단이 중요해졌다. 이 논문은 이러한 환자들을 진료하는 임상 현장에 좋은 지침이 될 것으로 판단된다.
[정리: 편집위원회]