성인척추변형 환자의 임상적 및 영상학적 지표
Clinical and radiographic parameters for patients with adult spinal deformity
Article information

Trans Abstract
Background
Improved medical care and increased life expectancy have led to a focus on the impact of adult spinal deformity (ASD) on health-related quality of life (HRQoL) in the field of the spine. Recently, there has been a paradigm shift in the evaluation and management of ASD regarding the important correlation between sagittal imbalance and clinical outcomes.
Current Concepts
Loss of lumbar lordosis is recognized as a key driver of ASD followed by forward-leaning of the trunk, reducing thoracic kyphosis, pelvic retroversion, and knee flexion. Radiological assessment has been critical for evaluating ASD from the anteroposterior and lateral view of the whole spine radiograph. Important parameters include coronal, regional, global, and sagittal spinopelvic parameters. Especially, sagittal spinopelvic parameters significantly correlate with disability and HRQoL in patients with ASD, which can influence the process of decision-making with respect to the choice between conservative treatment and surgery.
Discussion and Conclusion
Sagittal imbalance has been recently emphasized in patients with ASD. Therefore, the decision-making of ASD treatment should be focused on restoring harmonious alignment to prevent catastrophic complications and improvement of HRQoL.
서론
성인척추변형이 있는 환자들은 소아와는 달리 퇴행성 변화가 진행되면서 요통, 하지 방사통 및 파행 등을 수반하여 정상적인 보행이 어려워 일상 생활에 심각한 장애를 초래한다[1-3]. 방사선학적 지표의 관점에서, 척추 부위만의 변형(측만증과 후만증)과 함께 골반, 하지 관절의 형태와 자세에 의한 시상면 및 관상면 불균형을 동반하고 있기 때문에, 척추의 국소적인 문제는 물론 전신적인 불균형 상태에 대해 확인해야 한다[4]. 특히, 최근 연구 결과들은 시상면상의 불균형이 건강 관련 삶의 질(health-related quality of life)과의 연관성을 강조하고 있다[4]. 따라서 이 논문에서는 성인척추 변형에서 고려해야 할 방사선학적 지표로부터 임상학적 지표와의 관련성에 대해 정리하고, 장애와 통증의 관점에서 일차적 진단 계획의 수립에 대해 알아보고자 한다.
성인척추변형의 병태생리와 보상 기전
성인척추변형의 방사선학적 지표를 고려하기 위해서는 병태생리를 이해하는 것이 필수적이며, 이는 기립 자세에서 시상면의 균형을 유지하기 위한 보상 기전(compensatory mechanism)과 밀접한 연관이 있다[4-6]. 성인척추변형은 인대와 관절의 심각한 비후, 골극 형성 및 추체의 비대칭과 같은 원인에 의해 척추 정렬의 구조적 변화가 야기되고, 이는 요추 만곡의 소실을 초래한다[4]. 보상 작용으로서, 가장 경제적인 형태로 균형 기전의 변화가 발생하여 몸이 앞으로 기울어지고, 흉추 후만의 감소, 골반의 후방 경사(pelvic retroversion), 무릎 굴곡으로 진행하게 된다(Figure 1) [1]. 척추 정렬의 불균형이 심화될수록, 기립 자세를 유지하기 위한 하지와 체간의 근육 사용이 늘어나면서 피로와 통증, 장애를 야기하게 된다[7,8]. 이로 인한 장애와 삶의 질의 심각한 저하는 수술적 치료를 요하게 되어 사회적, 경제적으로 막대한 손실을 야기한다[9-11].
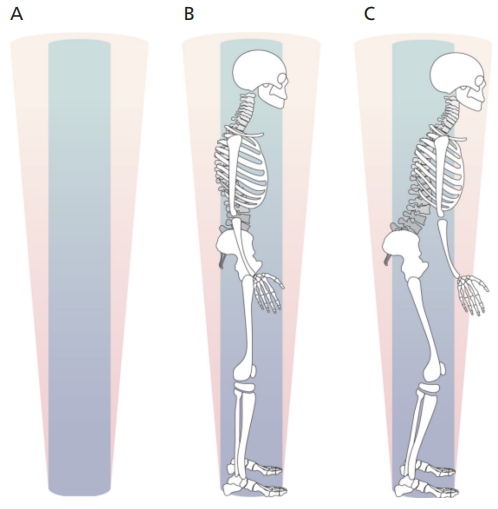
Change of posture in the patient with adult spinal deformity. (A) Conus of economy. (B) The posture for the patient with normal alignment. (C) Degenerative changes in the spine including loss of lordosis and kyphosis can result in postural changes that push the body to the periphery of the cone of economy, which requires more energy to maintain upright posture. Illustrated by the author.
성인척추변형의 방사선학적 평가
성인척추변형의 방사선 촬영은 14×36인치의 필름을 사용하여 척추 전체, 골반, 고관절이 포함되도록 검사하여야 하며, 척추의 균형 상태는 골반, 고관절과 슬관절의 자세에 따라 변하기 때문에 기립, 중립 자세에서 일정하게 촬영하여야 한다[1]. 양발은 어깨 넓이만큼 벌리고, 고관절과 슬관절은 중립 상태에서 똑바로 선 채로, 주관절을 굴곡시켜 손을 쇄골 위에 위치시키는 자세를 취하거나 팔을 뻗어서 지지대를 잡고 촬영한다[4].
척추 전후면 및 시상면 방사선 사진을 기반으로 시상면 정렬과 관상면 정렬(coronal parameter)을 확인한다. 시상면 정렬을 평가하기 위한 지표는 국소형 지표(regional parameter), 전신형 지표(global parameter), 척추-골반 지표(sagittal spinopelvic parameter)로 나눌 수 있다(Figure 2) [4,12].
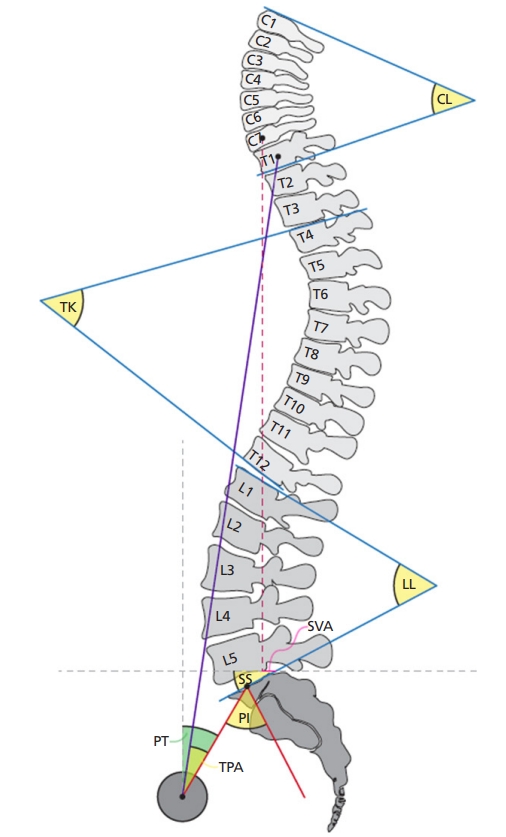
The important sagittal radiological parameters of adult spinal deformity. Reproduced from Kim HJ, et al. Asian Spine J 2020;14:886-897, according to the Creative Commons licence [4]. CL, cervical lordosis; TK, thoracic kyphosis; LL, lumbar lordosis; SVA, sagittal vertical axis; PI, pelvic incidence; PT, pelvic tilt; SS, sacral slope; TPA, T1 pelvic angle.
1. 국소형 지표
국소형 지표는 경추 전만각(cervical lordosis angle), 흉추 후만각(thoracic kyphosis angle), 요추 전만각(lumbar lordosis angle, LL)을 포함한다[4]. 경추 전만각은 제2경추 하연에서 제7경추 하연 사이의 각도를 측정하며, 정상 범위는 30-35도로 생각한다[13]. 흉추 후만각은 제4흉추 상연에서 제12흉추 하연 사이의 각도를 측정하며, 정상 범위는 약 20-40도이다[1]. LL은 제1요추 상연에서 제1천추 상연 사이의 각도를 측정하며, 정상 범위는 약 40-60도이다[1].
2. 전신형 지표
전신형 지표는 시상축(sagittal vertical axis, SVA)과 제1흉추-골반각(T1 pelvic angle)을 포함한다. 시상축은 제7경추 척추체 중앙에서 내린 수직선(C7 plumb line, C7PL)에서 제1천추 척추체 상연의 후방 모서리 사이의 거리이다[4]. C7PL이 제1천추 척추체 상연의 후방 모서리보다 전방에 위치하면 양의 값으로, 후방에 위치하면 음의 값으로 표현한다. 제1흉추-골반각은 제1흉추 척추체 중앙에서 대퇴골두 중심을 잇는 선과 대퇴골두 중심에서 제1천추 상연 모서리의 중간 지점을 잇는 선 사이의 교차하는 각도로 정의한다[4].
3. 척추-골반 지표
척추-골반 지표는 골반 입사각(pelvic incidence, PI), 골반 기울기(pelvic tilt, PT), 천골 경사(sacral slope, SS)를 포함한다[1-3]. PI는 대퇴골두 중심에서 제1천추 상연 모서리의 중간 지점을 잇는 선과 제1천추 상연의 수직으로 그은 선 사이의 교차하는 각도로 정상치는 한국인에서 평균 52.6도로 알려져 있다[1]. PT는 대퇴골두 중심에서 제1천추 상연 모서리의 중간 지점을 잇는 선과 대퇴골두 중심에서 수직으로 그은 선 사이의 교차하는 각도로 정상치는 평균 13도로 알려져 있다. SS는 제1천추 상연 모서리와 제1천추 상연 모서리 후방 끝 지점에서 수평으로 그은 선 사이의 각도로 정의하며 정상치는 평균 39.6도로 알려져 있다[1,4].
PI는 천추가 골반에 연결되어 기울어져 있는 정도를 의미하기 때문에, 성장이 완료되면 거의 변하지 않는 고정값이며, 골반의 해부학적 형태를 반영한다[3]. 척추와 골반이 연결되는 기울기의 정도는 LL과 흉추 후만각에 영향을 끼치기 때문에, 시상면의 불균형에 대해 PI를 고려할 때에는 반드시 LL을 포함하여 생각해야 한다. LL의 소실은 PI와 LL 사이의 부조화(PI/LL mismatch)를 야기하며, 이는 건강-관련 삶의 질과 장애를 예측하는 중요한 지표 중 하나이다[14-16]. 그러나 PT와 SS는 골반의 자세와 위치에 따라 변하며 골반의 방향을 나타낸다. 즉, 낮은 PT는 골반의 전방 경사(anteversion)을 높은 PT는 골반의 후방 경사(retroversion)을 의미한다. SS는 요추에 대한 천추의 상대적 위치를 결정하는 인자로서 낮은 SS는 천추가 수평, 높은 SS는 천추가 상대적으로 수직으로 위치함을 반영한다[4]. 산술적으로 PI는 PT와 SS의 합(PI=PT+SS)을 의미하기 때문에, 골방의 후방 경사(높은 PT)은 천추가 상대적으로 수평으로 위치하게 된다(낮은 SS).
4. 관상면 지표
관상면에서는 Cobb 각도와 척추체의 축성 회전 여부를 확인하며, 이를 기반으로 측만의 정도를 측정한다. 관상면 정렬을 판단하기 위해 관상면 균형(coronal balance)을 조사하는데 이는 C7PL에서 천추체의 중앙에서 내린 수직선(central sacral vertical line, CSVL) 사이의 거리이다. C7PL이 CSVL보다 후방 모서리보다 우측에 위치하면 양의 값으로, 좌측에 위치하면 음의 값으로 표현한다(Figure 3) [4].

The coronal parameters of adult spinal deformity. C7PL, C7 plumb line; CSVL, central sacral vertical line; CB, coronal balance. Illustrated by the author.
임상적 지표와의 연관성
성인척추변형 환자의 방사선학적 불균형은 임상적 지표와 밀접한 연관성이 있다[15]. 다양한 임상적 지표와의 연관성을 기반으로, Schwab 등[16]은 2012년도에 Scoliosis Research Society-Schwab 분류법을 제안했는데, 이 분류는 측정자간 및 측정자 내 신뢰도가 높고 관상면 곡선 유형과 PI와 LL 사이의 부조화, SVA, PT를 시상 변형의 수정 지표로 사용하였다. 시상 변형의 수정 지표들의 값이 증가는 환자의 장애를 나타내는 지수인 요통 기능 장애 척도(Oswestry disability index)와 통증이 증가하는 상관 관계가 있음이 여러 문헌에서 밝혀졌다[16,17].
여러 다기관, 전향 연구들을 통해 척추-골반 지표와 건강 관련 삶의 질과 양의 상관 관계가 있음이 보고되었다. Schwab 등[16]은 PI와 LL 사이의 부조화가 11도 이상, SVA가 47 mm 이상, PT가 22도 이상에서 예측되는 요통 기능 장애 척도가 40 이상으로 될 수 있음을 보고하였다. 또한 Terran 등[17]은 여러 척추 관련 임상적 척도는 시상 변형의 수정 지표에 따라 유의미한 차이가 있다고 보고하였다. 하지만 Scoliosis Research Society-Schwab 분류법은 시상면의 수정 지표들이 임상적 지표와의 연관성을 보여주는 중요한 체계이지만, 수술적 술기 선택의 구체적인 방안을 제안하지는 못했다는 한계점을 지니고 있다[11].
결론
시상면 불균형은 성인척추변형 환자에 있어 장애와 건강 관련 삶의 질과 연관성이 있으며, 이에 따라 최근 그 중요성이 강조되고 있다. 따라서 성인척추변형 환자의 적절한 평가와 올바른 치료는 건강 관련 삶의 질의 개선과 관련된 방사선학적 불균형을 복원하는 데 중점을 두어야 한다.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
References
Peer Reviewers’ Commentary
이 논문은 성인 척추변형 환자의 적절한 평가와 올바른 치료를 위한 임상적 및 방사선학적 지표를 정리하여 소개하고 있다. 성인 척추변형은 정상적인 척추 기능의 불균형을 유발하여 환자들의 삶의 질에 부정적인 영향을 주는 질환이다. 최근 평균 기대 수명 및 기본적인 삶의 질에 대한 관심 증가로 성인 척추변형 환자들을 대상으로 하는 척추 변형 수술 및 치료의 빈도가 늘어나고 있다. 이 논문에서는 척추 정렬의 구조적 변화 및 그로 인한 요추 만곡의 소실을 보이는 성인 척추변형의 병태생리와 척추 및 골반의 보상 작용에 대해 적절하게 설명해 주고 있다. 특히, 여러 지표 중에 시상면 불균형이 성인 척추변형 환자에 있어 장애 및 삶의 질에 가장 큰 영향을 준다는 최신 연구를 잘 소개해 주고 있다. 이 논문은 성인 척추변형 환자들의 진단 및 치료를 시행하는데 좋은 지침을 제공할 것으로 판단된다.
[정리: 편집위원회]