정신건강의학과 입원 청소년에서 자해와 관련된 임상 및 정신사회 특성: 후향적 의무기록 연구
Clinical and psychosocial characteristics related to self-harm in adolescent admitted to psychiatric wards in Korea: a retrospective chart review
Article information
 , Yoo-Sook Joung, MD, Byoung-Uk Kim, MD, Hyerin Lee, MD, Jung Yoon Cha, MD, Chang Won Jang, MD, Bo Mi Ahn, PhD
, 정유숙, 김병욱, 이혜린, 차정윤, 장창원, 안보미
, Yoo-Sook Joung, MD, Byoung-Uk Kim, MD, Hyerin Lee, MD, Jung Yoon Cha, MD, Chang Won Jang, MD, Bo Mi Ahn, PhD
, 정유숙, 김병욱, 이혜린, 차정윤, 장창원, 안보미
Trans Abstract
Background
Self-harm is an important public health problem with increasing incidences among adolescents for over a decade. This study aimed to identify factors associated with self-harm in adolescent psychiatric inpatients in Korea. We also investigated clinical characteristics associated with nonsuicidal self-injury disorder (NSSI-D) and suicidal behavior disorder (SBD) according to the Diagnostic and Statistical Manual of Mental Disorders 5 criteria.
Methods
This retrospective study included 215 adolescents aged between 12 to 18 years, who were admitted to the psychiatric ward of Samsung Medical Center, Seoul, Korea, from January 2014 to February 2021. Participants were divided into three groups according to NSSI-D and SBD diagnostic criteria. Collected data were analyzed using chi-square test and analysis of variance test.
Results
Overall, 57.7% of the participants (n=124) reported self-harm at least once in their lives. Patients with self-harm were more likely to have experienced parental conflict, parent-child relational problems, and verbal, physical, or sexual abuse. Among the three groups divided according to NSSI-D and SBD diagnostic criteria, patients with both NSSI-D and SBD were more likely to have experienced parent-child relational problems than those with either NSSI-D only or SBD only.
Conclusion
This study shows that parent-child relational problem is associated with high incidences of selfharm. Especially, the parent-child relational problem seemed to be a risk factor for SBD among patients with NSSI-D. These are important findings that provide an understanding of the self-harm characteristics and therefore improve prevention and treatment strategies in psychiatric adolescent patients.
Introduction
With the growing scientific interest in self-harm, studies have been conducted to identify risk factors for self-harm. Childhood adverse experiences, such as sexual and physical abuse, emotional neglect, and unstable attachment, were associated with selfharm in later life [1,2]. Community-based study also reported that poor family function mediates the association between childhood adversity and nonsuicidal self-injury (NSSI) in adolescence [3]. In a study of hospitalized adolescents, negative life events were associated with increased chances of NSSI occurrence [4], and a meta-analysis of 21 studies reported that there was a significant correlation between life stress and NSSI [5]. Furthermore, a study of adolescents in ten European countries showed an association between bullying and self-harm [6], and a significant association between NSSI and bullying was reported by a metaanalysis of nine studies [7].
Many studies have focused on the relationship between self-harm and suicide. Suicidal thoughts and behaviors are more likely to follow self-injurious thoughts and behaviors [8,9]. Self-harm is a major risk factor for suicide, and researchers have found that suicide rates are significantly high in the first year after self-harm occurs [10]. More than half of those who died by suicide had a history of self-harm [11], and NSSI before the age of 18 has been associated with a higher likelihood of future suicide attempts (SAs) [12,13]. Suicidal risk has been shown to increase with the presence of comorbid mental illness or repetitive self-harm [14], and frequent self-harm has been associated with the presence of mental illness [15].
In a previous study on community populations in Korea [16], 13.8% of middle and high school students reported having injured themselves in the past year, which is comparable to the 12-month incidence in Europe and the United States [17]. Another research on the middle school students in Korea found that 12.4% of the students had self-harmed at least once and that the self-harm group had significantly higher levels of academic stress, alexithymia, depression, and difficult relationships with parents and peers [18]. In a study of risk factors for NSSI in adolescent depressed patients, researchers found that the self-harm group had significantly higher levels of anxiety, suicidal ideation, and emotional and physical abuse [19].
Although several investigations have identified clinical characteristics associated with self-harm, the previous studies have limitations in that they targeted the community populations or adolescents with specific psychiatric diseases. Moreover, most of the studies used the dichotomous definition of self-harm behavior as NSSI or SA. Therefore, it is necessary to investigate clinical factors associated with the broad concept of self-harm regardless of suicidal intent and whether the clinical factors are different between NSSI and suicidal behavior in Diagnostic and Statistical Manual of Mental Disorders (DSM)-5, in the clinical population.
Therefore, the purpose of this study was to compare the clinical and psychosocial characteristics of psychiatric adolescent inpatients at Samsung Medical Center, a university hospital based on the presence of self-harm and to examine the factors that predict selfharm. Furthermore, we investigated whether clinical factors were significantly different when divided into NSSI and suicidal behavior disorder (SBD) in DSM-5.
Methods
1. Ethics statement
The study was based on a retrospective chart review and received ethical approval from the Samsung Medical Center Institutional Review Board (IRB No. SMC 2021-07-114). Obtainment of the informed consent was exempted.
2. Study design
It is a retrospective chart review. It was described according to strengthening the reporting of observational studies in epidemiology (STROBE) statement (https://www.strobe-statement.org/).
3. Participants
The medical records of 294 adolescents aged between 12 and 18 years who were admitted in the inpatient psychiatric unit from January 2014 to February 2021 were retrospectively reviewed by two psychiatrists using electronic medical records. All the participants were admitted and assessed at the Department of Psychiatry, Samsung Medical Center in Seoul, Korea. Exclusion criteria were intelligence quotient (IQ) scores lower than 80 and acute psychotic symptoms. Since suspected intellectual disability could bias the results of the selfharm characteristics, it was excluded from the scope of this study [20,21].
4. Definition for grouping
The participants were divided into a group with or without self-harm behavior. Factors related to selfharm (e.g., presence of self-harm behavior, methods of self-harm, and age of onset) were examined by psychiatrists through a retrospective review of medical records. In this study, regardless of suicidal intent or motive of self-harm, intentional self-injury such as cutting or hitting, self-poisoning, and hanging or jumping gestures were included in self-harm behavior. Among participants with self-harm, those who met either NSSI-disorder (NSSI-D) or SBD were divided into three groups: (1) patients who met the criteria for both NSSI-D and SBD, (2) patients who met criteria for only NSSI-D, (3) patients who met criteria for only SBD according to DSM-5. Among participants with a history of NSSI or suicidal attempts, those who did not meet the diagnostic criteria for NSSI-D or SBD were excluded from the subgroup analysis. An overview of the participants is shown in Figure 1.
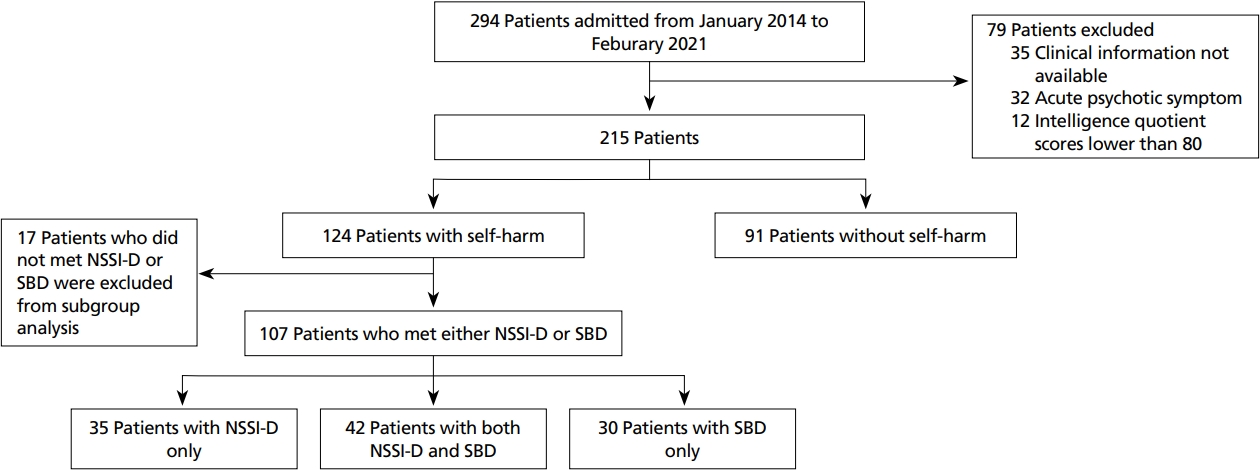
Inclusion criteria of the study participants. NSSI-D, nonsuicidal self-injury disorder; SBD, suicidal behavior disorder.
5. Variables
A broad definition of self-harm is used in this study, which is defined as intentional injury to one’s own behavior without regard for the degree of suicide intention. The self-harm history (if the patient had self-harmed at any time) and variables associated with self-harm (parental conflict, parent-child relational problem, verbal or physical abuse, bullying and academic stress) were all dichotomous according to presence or absence. The control variables in this study included age, gender, psychiatric diagnosis.
Demographic and psychosocial information was obtained from the electronic medical records. The subjects were assessed by a multidisciplinary team consisting of child psychiatrist, clinical psychologist, social worker, speech therapist, and occupational therapist during hospitalization. Psychosocial factors related to self-harm (parental conflict, parent-child relational problem, verbal, physical, or sexual abuse, bullying, and academic stress) were categorized as presence or absence based on documented family evaluation assessed by the multidisciplinary team.
6. Data sources/measurement
The psychiatric diagnosis was evaluated through clinical observation by psychiatrists and Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADSPL) conducted by a trained clinical psychologist. The reliability and validity of the Korean version of the K-SADS-PL were previously determined in the diagnosis of adolescent psychopathology [22] and its usefulness as a diagnostic tool was verified [23].
The participants completed the Korean version of the Beck depression inventory-II (BDI-II) [24], Beck anxiety inventory (BAI) [25], Beck hopelessness scale (BHS) [26], and children’s depression inventory (CDI) [27]. The reliability and validity of the Korean version of the BDI-II [28], BAI [29], BHS [30], and CDI [31] were previously determined.
To compare cognitive functioning according to self-harm behavior, participants under the age of 16 had received the Korean Weschler Intelligence Scale for Children-Fourth Edition (K-WISC-IV) and participants over the age of 16 had received the Korea Wechsler Adult Intelligence Scale-Fourth Edition (K-WAIS-IV) by a trained clinical psychologist. K-WISC-IV and K-WAIS-IV had previously proven reliability and validity [32]. Full-scale IQ (FSIQ) and four index scores, consisting of verbal comprehension (VC), perceptual reasoning (PR), working memory, and processing speed, were compared according to each group. To objectively measure the attention problem of participants, Conners continuous performance tests were performed [33,34].
7. Bias
Due to the retrospective nature of this study, we addressed the bias by having two psychiatrists review the medical charts. We were able to reduce recall bias because all adolescents admitted to the ward were evaluated for self-harm initially in their hospitalization, regardless of whether there was self-harm. Furthermore, because the control group in this study was selected from hospitalized patients, psychiatric symptom scores were also considered, which could characterize the control group.
8. Study size
Based on the literature, exposure rates for various risk factors in control group ranged between 10% to 30%. We assumed exposure rate in control as 10.0% in this study. With a power of 0.8 and significance level of 0.05, the sample size was calculated to be 97 patients per group.
9. Statistical analysis
An independent t-test was performed for continuous variables and a chi-square test, or fisher’s exact test was performed to compare demographic and psychosocial factors between the group with or without self-harm. Logistic regression analysis was conducted to examine the association of psychological variables and other clinical characteristics with the presence of self-harm. Analysis of variance (ANOVA) and post-hoc Bonferroni correction were performed to compare variables among the three diagnostic groups with NSSI-D or SBD. All analyses were performed using R Statistical Software ver. 4.1.2 (Foundation for Statistical Computing, Vienna, Austria), and the P-value under 0.05 was considered statistically significant.
Results
1. Demographic and clinical characteristics
The subject comprised 215 adolescent patients, with a mean age of 15.6 years (standard deviation, 1.62) and 124 (57.7%) of the study population reported a history of selfharm including SAs. Demographic and psychosocial characteristics are shown in Table 1. There were significant differences in gender ratio between patients with self-harm and those without. Adolescents with self-harm showed a higher ratio of females than those without (χ²=32.6, P<0.001). Patients with self-harm reported significantly more parental conflicts (χ²=4.40, P=0.036), parent-child relational problems (χ²=14.1, P<0.001), and verbal, physical, or sexual abuse (χ²=6.30, P=0.012) than patients without self-harm. The self-harm group reported significantly more suicidal ideation (χ²=67.7, P<0.001). In addition, the self-harm group was significantly more likely to be diagnosed with depressive disorder (P=0.015). Most common diagnosis in self-harm group was depressive disorder (n=64, 51.6%), followed by bipolar and related disorder (n=58, 46.8%), anxiety disorder (n=18, 14.5%), and attentiondeficit hyperactivity disorder (n=17, 13.7%). Nonself-harm group was significantly more likely to be diagnosed with attention-deficit hyperactivity disorder (P=0.019) and oppositional defiant disorder or conduct disorder (P=0.009).
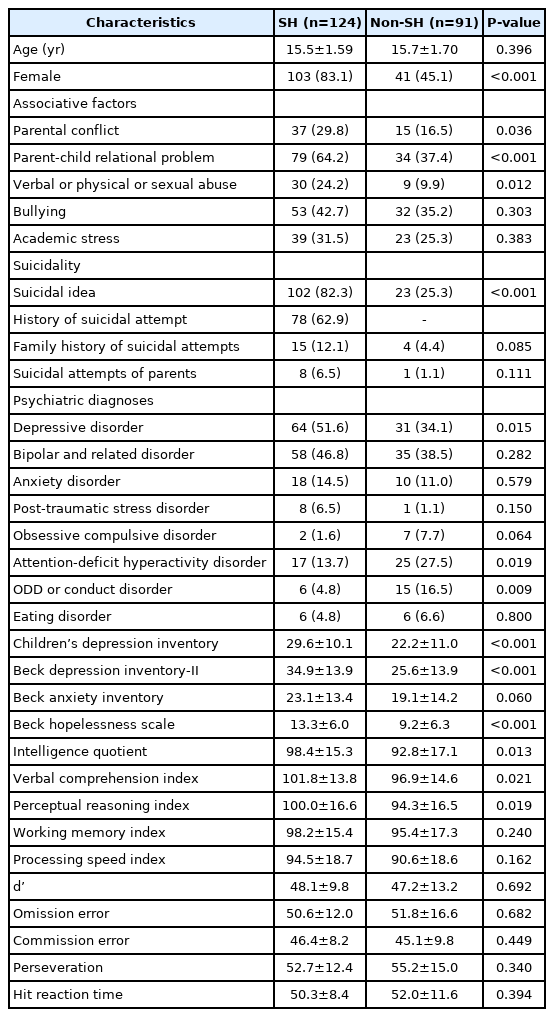
Baseline characteristics of subjects with or without self-harm
Psychological assessment was conducted to investigate differences in clinical characteristics between patients with or without self-harm. Clinical characteristics are shown in Table 1. Self-harm group showed significantly higher levels of CDI (t=3.89, P<0.001), BDI-II (t=4.29, P<0.001), and BHS (t=4.21, P<0.001) scores. BAI score in the self-harm group was higher than in the non-self-harm group, although the difference between the two was insignificant (t=4.21, P=0.060).
There was a significant difference in FSIQ scores between patients with and without self-harm. Patients with self-harm showed a significantly higher level of FSIQ scores than those without (P=0.013). Among the index score, verbal comprehension index score (t=2.33, P=0.021) and perceptual reasoning index score (t=2.37, P=0.019) were significantly higher in patients with selfharm than those without. There were no significant differences in all Conners continuous performance test parameters between groups with or without self-harm.
In multivariate logistic regression, variables included were age, gender, suicidal idea, adverse experiences associated with self-harm, diagnosis, and psychological distress (BDI, BAI, and BHS). Female (odds ratio [OR], 6.59, P<0.001), suicidal idea (OR, 9.73; P<0.001), depressive disorder (OR, 17.36; P=0.009), bipolar disorder (OR, 11.39; P=0.024), and verbal, physical or sexual abuse (OR, 4.56; P=0.034) were significantly associated with self-harm.
2. Characteristics of self-harm
The most common method of self-harm was cutting (n=97, 78.2%), followed by self-poisoning (n=38, 30.6%), jumping (n=30, 24.2%), and hanging (n=25, 20.2%). The average age of onset of self-harm in the self-harm group was 14.0 years (standard deviation, 1.96). 72.6% (n=90) of the patients with self-harm reported a history of NSSI, while 62.9% (n=78) of the patients with self-harm reported a history of SAs. 5 (13.2%) of those who had a history of self-poisoning reported no suicidal intent.
3. NSSI-D and SBD according to DSM-5
Among the patients, 77 (35.8%) met the criteria for NSSI-D and 72 (33.5%) met the criteria for SBD. Patients meeting the criteria for either NSSI-D or SBD were divided into three groups: met the criteria for (1) both NSSI-D and SBD (n=42), (2) NSSI-D only (n=35), (3) SBD only (n=30). 54.5% of the patients who met the criteria for NSSI-D met with SBD, whereas 58.3% of patients who met the criteria for SBD met with NSSI-D.
Analyses were conducted among the three diagnostic groups and the results are shown in Table 2. There were significant differences in gender ratio among the groups. Patients who met both NSSI-D and SBD and met NSSI-D only showed a higher ratio of females than those who met SBD only. With regards to associative factors, both NSSI-D and SBD groups reported significantly more parent-child relational problems (P=0.044) than those who met either NSSI-D or SBD. There were no differences in other adverse experiences among the groups. Both NSSI-D and SBD groups (97.6%) and SBD-only groups (93.3%) showed a higher ratio of suicidal ideas than the NSSI-D only group (65.7%). Regarding psychiatric diagnosis, NSSI-D only group and SBD-only groups were more likely to be diagnosed with depressive disorder, while both NSSI-D and SBD group was diagnosed with bipolar and related disorder (59.5%). Psychological assessments results were compared among the three groups and there are no significant differences among the groups.

Demographics in association with NSSI-D and SBD according to Diagnostic and Statistical Manual of Mental Disorders 5
Characteristics and function of self-harm were compared among the three groups and the results are shown in Table 3. There were no significant differences in age of onset of self-harm among the groups. Patients with both NSSI-D and SBD and patients with NSSI-D only were more likely to use cutting (95.2%, 94.3%) for self-harm than SBD only groups (31.0%). Patients with both NSSI-D and SBD, and patients with SBD only were more likely to use self-poisoning (42.9%, 62.1%) for self-harm than NSSI-D only group (5.7%). There were significantly higher rates of jumping and hanging, in both NSSI-D and SBD groups and SBD-only group. Patients with both NSSI-D and SBD showed a higher ratio of doing self-harm for feeling generation (33.3%) than the NSSI-D only group (17.1%), however, there were no significant differences.
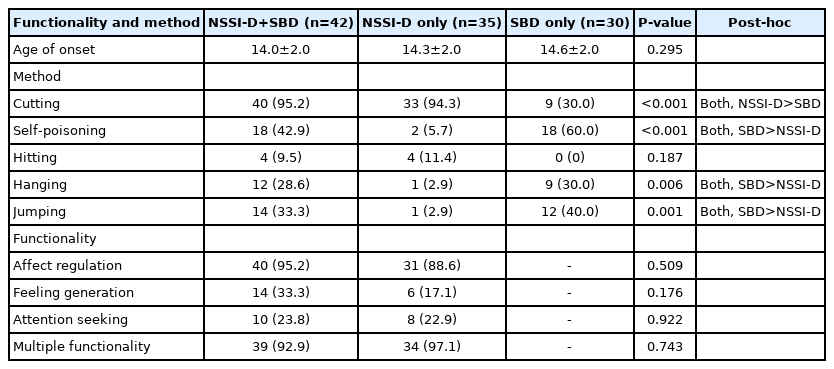
Functionality and method of self-harm in association with NSSI-D and SBD according to Diagnostic and Statistical Manual of Mental Disorders 5
Discussion
In the analysis of self-harm groups based on DSM-5 criteria, adolescents with SBD only had a significantly lower proportion of females than the other two groups similar to a previous study on Korean adolescents [35]. In the current study, the prevalence rate that met the diagnostic criteria for NSSI-D and SBD were 32.8% for NSSI-D and 33.5% for SBD; the prevalence was comparable with the study based on DSM-5 criteria [20].
There was a higher proportion of female patients in the self-harm group than the without self-harm group. This is consistent with results showing females had a greater rate of NSSI and that gender differences are more obvious among clinical patients [36]. However, it should be noted that our study included a higher total number of female adolescents. A previous study on the inpatients sample showed 65% to 71% of the adolescents were female and is close to the gender ratio in our study, which makes sense in the context of clinical reality [36-39].
With respect to suicidal ideas, there was a significant number of adolescents with self-harm who reported suicidal ideation than those without self-harm. In this study, broader definition of self-harm was used, and self-harm group included patients with SA. Notably, self-harm group in our sample showed more suicidal ideation than previous studies with NSSI [40]. In this study, even in the NSSI-D only group, in which suicidal behavior was not observed, the percentage of suicidal ideation was 65.7%, indicating a high rate. Therefore, a sample of our study of patients with self-harm including NSSI-D only group appeared to have high rate of suicidal ideation. In logistic regression, suicidal ideation was significantly associated with self-harm. Although NSSI is not associated with conscious suicidal intent, it is the strong predictor of suicidal ideation and suicidal attempt [41,42].
As in a previous study performed in the United States [1], the rate of physical or sexual abuse was also high in the self-harm group in this study. In addition, sexual, physical, emotional abuse, and emotional neglect, have been associated with self-harm in studies conducted in several other countries [43,44]. Thus, regardless of race or geographical location, childhood abuse appears to increase the risk of self-harm. Verbal abuse was considered as an abuse in this study, which is a concept that has been considered as an emotional abuse in previous studies. Therefore, since this study did not divide and compare the abuse types, we did not find which types of abuse have a greater effect on self-harm behavior. However, in future, if we employ objective methods according to each abuse, we will have a better understanding of the link between abuse and self-harm.
Addition to verbal, physical, or sexual abuse, patients with self-harm reported significantly more parental conflict and parent-child relational problems than patients without self-harm. These results are in line with those of a previous study that found that stressful life events were associated with self-harm [45]. Stressful life events include parental separation, divorce, and witnessing domestic violence, in addition to abuse and neglect [46,47], and it seems that adolescents are more exposed to these childhood adversities when they have parent-child relational problems or parental conflict. Bullying was more common in the self-harm group than in the control group, but there was no statistically significant difference. However, given that prior studies were done on a wide scale [6,7], it is probable that the difference did not occur owing to the limited number of participants in this study. Among the negative life events related to self-harm, the parent-child relationship problem was significantly high only in adolescents with both NSSI-D and SBD. Our findings suggest that the parent-child relationship is an important risk factor for suicide in adolescents with NSSI-D only. In a previous research study, individuals with NSSI only reported fewer negative events than those with NSSI and SA [48]. Emotional abuse and neglect in childhood have been linked to suicidal ideation and attempts in adolescents, especially severe SAs [49]. In the neurobiological developmental model of NSSI, adolescents with NSSI showed altered hypothalamic-pituitary axis and autonomic nervous system function, contributing to stress vulnerability [50]. In this context, it can be assumed that traumatic and persistent childhood adversity reduces the ability to cope with stress and appears as a more severe form of behavior on a continuum between NSSI and SA. Future research is needed on whether stress vulnerability differs according to the type of childhood adversity and biological factors that mediate the degree of serious self-harm.
There were no significant differences in psychological assessment in the analysis of the self-harm group divided into three subgroups. Regardless of suicidal intentions, it means that the difference in clinical scale is not significant in groups with self-harm. These results are in line with those of a previous study examining adolescents with NSSI and SAs in which there were no significant differences in clinical scores representing psychological symptoms [35].
With respect to psychiatric diagnosis, patients with self-harm were distributed a wide spectrum of diagnoses. The proportion of the disease group is close to that of a recent study with a Korean adolescent clinical sample, where 61.5% of the adolescent with NSSI were diagnosed with depressive disorder and 34.6% were diagnosed with bipolar disorder [21]. In the analysis that divided the self-harm group into three groups, the NSSI-D only and SBD only groups showed a significantly higher proportion of depressive disorder than both NSSI-D and SBD groups. In addition, the proportion of bipolar disorder was higher in both NSSI-D and SBD than in the other two groups, even though there was no statistically significant difference. For depression and bipolar disorder, the group with NSSI-D only and the group with SBD only showed similar disease distribution. This suggests that SAs in patients with NSSI have different characteristics from those without NSSI in terms of psychiatric diagnosis. In addition, the NSSI-D group with SBD showed different diagnostic profiles from the NSSI-D group without SBD. This seems to be an important implication for potential suicidal behavior in adolescents with NSSI-D.
With respect to functionality, there were no significant differences in the functionality of self-harm. Affect regulation was the most common reason for self-harm in both the NSSI-D and SBD and NSSI-D only groups, which is consistent with previous studies [41,51]. The urge to escape from an intolerable state of mind is a prominent motivation for self-harm, as supported by empirical [52] and theoretical research [53]. In consistence with this idea, previous research found that NSSI for affect regulation was significantly related to a history of SAs [51]. Our result showed that the motivation for affect regulation was not significantly different between the NSSI-D only group and both NSSI-D and SBD groups.
Patients with both NSSI-D and SBD and patients with NSSI-D only are more likely to use cutting for self-harm than patients with SBD only. Patients with both NSSI-D and SBD and patients with SBD were more likely to use self-poisoning for self-harm than patients with NSSI-D [54]. Jumping and hanging rates were significantly higher in both the NSSI-D and SBD groups and SBD only group than NSSI-D only group. These findings imply that adolescents with NSSI should be more conscious of the dangers of suicide behavior if they have a history of self-harm through poisoning, hanging, or jumping.
There were several limitations to our analyses. First, as the subjects were limited to one university hospital, variables of referral hospital may have influenced the interpretation of the results. Therefore, the sample size in this study was not an accurate representation of the clinical group or general adolescent population. Second, due to the limitations of retrospective chart review, the possibility that the variables included in the analysis were omitted and underestimated in the recording process cannot be ruled out. Third, since it is a cross-sectional study evaluated based on the time of hospitalization, the factors related to self-harm in the results cannot explain the casual relationship. Fourth, factors related to self-harm, such as parentchild relational problem, were classified according to presence or absence, and the qualitative evaluation was insufficient in this study. Fifth, when comparing the presence or absence of self-harm, self-poisoning was included; however, there was a limitation in that self-poisoning was excluded when in the comparison between the three self-harm groups because of the diagnostic criteria of NSSI.
Despite these limitations, this study is meaningful in that it was able to analyze self-harm-related factors and diagnoses for clinical adolescent groups with various diseases and identify results consistent with previous studies, which were limited to specific patient groups. In addition, we employed a broad self-harm definition to reduce misunderstanding in self-harm research. Meanwhile, in the future, further studies on the prevalence of NSSI and SBD in a wide range of conditions for further study using the DSM-5 criteria are required.
In conclusion, this study analyzed the psychosocial and clinical characteristics of hospitalized adolescents with various psychiatric diseases by dividing them into self-harm and non-self-harm groups. This study showed that female gender, suicidal idea, adverse experience associated with self-harm, and psychiatric diagnosis are associated with self-harm. The most common diagnosis in the self-harm group was depression, followed by bipolar disorder. Also, our results demonstrated that difficulties in relationships with parents and parental conflict were related to selfharm. Furthermore, when the self-harm group was divided into three categorical groups, each of the three groups exhibited different diagnostic profiles; therefore, future research should further develop and confirm initial findings by considering these three categorical groups.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
References
Peer Reviewers’ Commentary
이 논문은 정신건강의학과에 입원한 청소년 환자들의 의무기록을 기반으로 자해 병력 유무에 따른 집단 비교 분석을 시행한 후향적 연구논문이다. 대학병원에 입원한 청소년 환자를 대상으로 자해 행동이 있는 대상자를 자살 의도 유무에 따라 non-suicidal self-injury (NSSI)와 suicidal behavior disorder (SBD)로 나누고, NSSI와 SBD 모두 있는 군과 NSSI만 있는 군, SBD만 있는 군으로 나누어 비교 분석하였다. 최근 청소년들의 자해가 급증하면서 자해와 자살 구분의 어려움이 늘어나고 있다. 이러한 면에서 이 논문은 임상 현장에서 유용하게 적용할 수 있는 연구 결과를 잘 제시하고 설명해 주고 있다. 이 논문의 연구 결과를 토대로 자해 및 자살 청소년을 진료하는 임상 현장에서 탐색, 평가, 개입하기 위한 적적한 목표를 설정하는 데 좋은 정보를 제공할 것으로 판단된다.
[정리: 편집위원회]