경흉부 바늘생검을 이용한 폐암의 진단
Transthoracic needle biopsy for diagnosis of lung cancer
Article information

Trans Abstract
Background
Lung cancer is the most common cause of cancer deaths worldwide and accounts for approximately 2 million deaths annually. Despite advances in lung biopsy methods using bronchoscopy, a transthoracic needle biopsy continues to be used widely owing to its excellent accessibility and cost-effectiveness.
Current Concepts
Various guidance methods are used during a transthoracic needle biopsy to guide the biopsy needle toward the target lesion. Commonly used modalities include conventional computed tomography, computed tomography fluoroscopy, cone beam computed tomography, and ultrasonography. Complications of a transthoracic needle biopsy include pneumothorax (20.0%), hemorrhage or hemoptysis (11.0%), delayed pneumothorax (1.4%–4.5%), air embolism (0.02%–1.8%), and tumor seeding (0.12%–0.061%).
Discussion and Conclusion
Careful selection of the guidance method and needle type, based on the risk factors, the patient’s condition, and location of the lesion is important to achieve high accuracy and low complication rates during a transthoracic needle biopsy. If possible, the bronchoscopic approach should initially be attempted in high-risk groups.
서론
폐암은 전 세계적으로 매년 200만명이 진단받고 170만 명이 사망하여 암 사망률 부동의 1위를 차지하고 있으며, 우리나라에서도 매년 2만 명 가까이 폐암으로 인한 사망이 보고되고 있다[1,2].
미국에서 진행된 국가 폐암 검진 연구(National Lung Screening Trial) 결과, 폐암 고위험군에서 저선량 흉부 컴퓨터단층촬영(low-dose computed tomography, LDCT)을 이용한 검진이 폐암으로 인한 사망률을 20% 정도 낮출 수 있는 것으로 밝혀졌다. 이후 LDCT를 이용한 검진이 활발해지면서 폐암 의심 병변의 발견도 증가하고 있다[3].
의심 병변의 확진을 위해서는 조직검사가 필요하다. 폐조직검사 방법에는 수술적인 방법인 비디오 흉강경 수술(video-assisted thoracoscopic surgery)과 비수술적인 방법이 있다. 비수술적인 방법은 크게 접근 방법에 따라 기관지내시경을 이용한 방법과 경흉부 바늘생검(transthoracic needle biopsy 또는 percutaneous needle biopsy)으로 나눌 수 있다.
기관지내시경을 이용한 방법은 경기관지 폐생검(tranbronchial lung biopsy)이라고 하며, 과거에는 병변과의 연결이 예상되는 기관지에 포셉이나 바늘을 삽입하여 조직을 얻는 방법으로 말초 폐병변에 대한 정확도가 50% 정도에 불과하였으나, 최근에는 방사형 초음파(radial probe endobronchial ultrasound), 전자기유도 내비게이션 기관지내시경(electromagnetic navigation bronchoscopy)등을 이용하여 진단 수득률(diagnostic yield)이 70-80%로 상승하였다[4-7]. 하지만 기관지를 통한 접근 방법의 특성 상 기관지와 병변의 관계(bronchus sign)에 따라 접근성과 정확도가 좌우되는 한계와 검사 비용이 비싼 단점이 있다[8].
따라서 아직도 경흉부 바늘생검이 폐암의 조직진단에 널리 이용되고 있다. 경흉부 바늘생검은 민감도와 특이도가 각각 90%, 95% 정도로 우수하며, 검사 비용이 상대적으로 저렴한 장점이 있다[9]. 반면에 흉벽과 흉막, 폐실질을 천자하여 병변에 접근하는 검사 방법의 특성 상 기관지내시경을 이용한 폐생검에 비해 기흉 등 합병증 발생이 증가한다. 경흉부 바늘생검은 조직검사 바늘을 병변의 위치로 유도하기 위해 여러가지 유도방법을 사용하게 된다[10]. 이 논문에서는 대표적인 경흉부 바늘생검의 유도방법에 대하여 기술하고 검사의 정확도와 합병증에 영향을 미치는 인자들에 대하여 알아보고자 한다.
유도방법과 조직검사 바늘
1. 컴퓨터단층촬영 유도방법
환자의 특성과 병변의 위치에 따라 적절한 유도방법을 선택하는 것이 정확도를 향상시키고 합병증을 최소화하는데 영향을 미칠 수 있다. 1980년대부터 사용된 고식적인 CT 유도방법(conventional CT guidance)은 잘 정립된 방법으로 최근에 발표된 연구들에서 96.1-96.7%의 매우 우수한 진단 정확도를 보여주고 있다[11-13]. 또한, 1 cm 미만의 작은 병변에 대하여도 90% 이상의 진단 정확도를 나타내 가장 널리 사용되는 유도방법이다[10].
그러나 실시간으로 병변과 조직검사 바늘의 움직임을 확인할 수 없기 때문에 호흡 협조가 되지 않거나 의식이 명료하지 않는 환자에서는 적절한 조직을 얻는 것이 어려울 수 있다. 특히, 크기가 작은 병변에서 검사 도중 기흉이 발생하였을 경우에는 병변의 추적과 바늘 위치 조정이 어려워 검사가 실패할 수 있다. 호흡에 따른 움직임이 큰 하엽에 위치한 병변의 경우 이러한 상황에서 단점으로 부각되므로 기흉 발생의 고위험군이면서 하엽에 위치한 병변의 경우 실시간 추적이 가능한 유도방법을 사용하는 경흉부 바늘생검이나 기관지내시경을 이용한 경기관지 폐생검을 우선해서 고려해 볼 수 있다[5].
실시간 유도방법에는 CT투시 유도방법(computed tomography fluoroscopy guidance), 콘빔CT (cone beam computed tomography) 유도방법, 초음파 유도방법이 있다. CT투시 유도방법은 1990년대 도입되었으며, 생검 바늘의 위치를 실시간으로 확인하면서 표적 병변에 접근할 수 있기 때문에 호흡에 따른 움직임이 큰 위치나 호흡 조절이 잘 안되는 환자에서도 시행이 가능하다. 전향적 임상시험에서는 고식적인 CT 유도방법에 비해 시술시간과 흉막 천자 횟수에서 의미 있는 감소를 보였다. 하지만 진단 정확도의 차이는 없었다[12]. 또한, CT투시 유도방법은 검사 중 시술자가 방사선에 노출되며 CT 장치의 갠트리(gantry)의 공간적인 제약으로 인해 환자의 자세나 병변의 위치, 조직검사 바늘의 진입 지점에 따라 검사가 어려울 수 있다.
콘빔CT는 가장 최근에 도입된 유도방법으로 콘빔 X선 영상시스템을 이용하여 3차원 영상을 획득하는 동시에 형광투시(fluoroscopy) 영상을 이용하여 실시간으로 병변을 확인할 수 있다. 또한, 전용 소프트웨어를 이용하면 투시영상에서 직접 관찰되지 않는 간유리음영 결절(ground glass opacity nodule)이나 작은 결절을 표시하는 가상의 영상(integrated virtual guidance image on fluoroscopic view, Bull’s eye view)을 유도에 사용할 수 있다[14]. 그러나 이러한 영상을 이용하더라도 형광투시영상의 한계로 인하여 형광 투시에서 직접 관찰되지 않는 병변의 진단 정확도는 관찰되는 병변에 비해 낮다(76.7% 대 89.1%, P=0.042) [15]. 이러한 병변들에서는 오히려 실시간으로 CT 영상을 얻을 수 있는 CT투시 유도방법이 유리할 가능성이 있다[15,16]. CT투시와 콘빔 CT 유도방법을 비교한 후향적인 분석 연구에서 각각의 진단 정확도는 94%, 96%로 의미 있는 차이가 없었다(P=0.330) [17]. 형광 투시에서 관찰되지 않는 간유리 음영 결절이나 작은 크기의 결절의 조직검사에 어떠한 유도방법이 더 우수한지는 추가적인 연구가 필요하다.
2. 초음파 유도방법
초음파유도 경흉부 바늘생검은 흉막과 붙어 있어 초음파로 관찰되는 폐병변에서 사용해 볼 수 있다. 초음파유도 생검의 진단 정확도와 악성병변에 대한 민감도(sensitivity for malignancy)는 각각 88.7%, 91.5%로 보고되었으며, 가장 흔한 합병증인 기흉은 4.4%로, 기타 유도방법의 20%에 비해 우월했다[10,18]. 초음파의 특성 상 흉벽과 병변 사이에 공기가 포함되어 있는 폐실질이 있으면 이용이 불가능한 단점이 있으나 병변과 조직검사 바늘을 실시간으로 관찰할 수 있으며, 환자와 검사자에 방사선 노출이 없는 장점이 있다. 또한, 검사 직후 초음파를 이용하여 기흉, 혈흉과 같은 합병증 발생 여부를 확인할 수 있다[19].
3. 조직검사 바늘
세침흡인검사(fine needle aspiration)는 세포병리검사 검체를 얻는 반면에 중심부바늘생검(core needle biopsy)은 직경이 더 큰 조직검사 바늘의 절단면을 이용하여 조직의 형태가 보존되어 있는 조직병리검사 검체를 얻게 된다[2,3]. 중심부바늘생검은 세침흡인검사에 비해 진단 정확도(93%), 민감도(89%) 및 특이도(97%)가 약간 더 높은 것으로 보고되었다 [20]. 하지만 rapid on-site evaluation을 이용하면 진단 정확도에 차이가 없다[20]. 다만, 유전자검사(molecular test)에 이용할 경우에는 중심부바늘생검으로 얻는 formalin-fixed paraffin-embedded 조직이 더 적합한 것으로 나타났다[21]. 또한, 괴사성 육아종(necrotizing granulomas)과 같은 특정 병리학적 소견의 확인이 필요한 양성 병변이나 림프종과 같이 명확한 진단 및 아형 분류를 위해 구조의 확인이 필요한 악성 병변에서는 중심부바늘생검이 선호된다[22,23].
중심부바늘생검은 단일바늘 방법(single needle technique) 이나 이중구조 유도바늘 방법(coaxial needle technique) 을 이용할 수 있는데. 이중구조 유도바늘 방법은 이중구조 유도바늘을 병변까지 삽입 후 속이 빈 외피(outer sheath)를 거치한 상태로 반복하여 조직병리검사 검체를 얻는 방법이다[24]. 반면에 단일바늘 방법은 조직을 얻을 때마다 반복적으로 흉벽과 흉막을 천자해야 한다. 최근 발표된 후향적 분석에 따르면 병변의 크기가 1.5 cm 미만이고 바늘의 통과 길이(needle path length)가 4 cm 이상인 경우 이중구조 유도바늘 방법이 더 높은 진단적정확도(95.5% 대 72.7%, P=0.023)와 낮은 기흉 발생률을 보여주었다[25].
합병증
1. 기흉
경흉부 바늘생검의 합병증에는 기흉, 출혈(객혈), 지연성 기흉, 공기 색전증, 종양 파종(tumor seeding) 등이 있다(Table 1) [26-28].

Complications of transthoracic needle biopsy
그 중 기흉은 경흉부 바늘생검의 가장 흔한 합병증으로 발생률은 약 20%이다[10]. 기흉의 위험인자는 2 cm 이하의 작은 병변, 폐기종의 존재, 폐기종의 양, 중심부바늘생검, 바늘 삽입 깊이, 0.1-2 cm의 병변 깊이, 하엽, 반복적인 흉막 천자 등이 있다(Table 2) [26,29-31]. 합병증 발생을 줄이기 위해서는 적절한 유도방법을 선택하는 것도 중요한데, 앞부분에서 기술한 바와 같이 초음파 유도방법의 기흉 발생률은 약 4%로 보고되어 있어 흉막 접촉이 있는 병변일 경우 고려할 수 있다. 그 밖에 조직 획득 10초 이내에 천자 부위를 아래로 환자 자세를 변경하거나(rapid needle-out patientrollover technique), 조직 획득 후 조직검사 바늘을 제거함과 동시에 자가혈액(autologous blood patch) 또는 생리식염수를 주입함으로써 기흉 발생률 및 흉관 삽입 빈도를 감소시킬 수 있다[32-38].
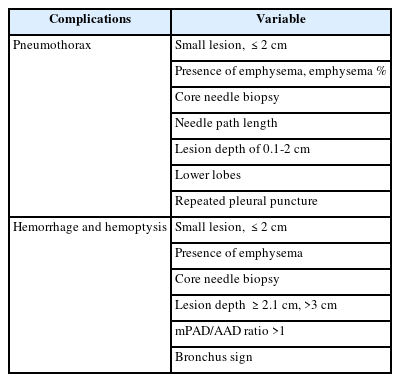
Risk factors for pneumothorax and hemorrhage (hemoptysis)
시술 3시간 이후에 발견된 기흉을 지연성기흉(delayed pneumothorax)이라고 하는데 최대 4.5%까지 발생률이 보고된다. 원인은 불분명하나 시술 후 바늘이 제거된 위치에 있던 혈괴(blood clot)가 탈락되면서 발생한다는 기전이 제시되었다[27]. 대부분의 국내 의료기관들은 경흉부 바늘생검을 입원 상태에서 시행하는 경우가 많아 크게 문제가 되지 않으나 외래에서 시행할 경우 응급실 방문 등 문제의 소지가 될 수 있다. 최근 소규모 전향적인 연구에서 시술 후 폐초음파가 임상적으로 의미가 있는 지연성기흉의 발생을 100% 민감도로 발견할 수 있다는 보고가 있어 당일 퇴원하는 고위험군에서 적용해볼 수 있겠다[39].
2. 출혈(객혈)
출혈(객혈)은 2번째로 흔한 합병증으로 발생 빈도는 약 11%로 보고되고 있다[10]. 잘 알려진 위험인자로는 2 cm 이하의 작은 병변, 폐기종의 존재, 중심부바늘생검, 병변의 깊이 2.1 cm 이상, 병변의 깊이 3 cm 초과, 주 폐동맥과 상행대동맥 직경의 비가 1 초과(main pulmonary artery diameter/ascending aorta diameter ratio >1), 열린 기관지 징후(open bronchus sign) 등이 있다(Table 2) [26,29-31,40,41].
기관지 징후가 있을 경우 기관지내시경을 이용한 조직검사의 정확도가 상승하는 반면에 경흉부 바늘생검에서 객혈의 발생률은 증가하므로 기관지 징후 양성일 경우 가능하면 경기관지 폐생검을 먼저 고려하는 것이 좋다[8,41].
결론
기관지내시경을 이용한 폐조직검사 방법들의 발전에도 불구하고 접근성과 비용 측면에서 우수한 경흉부 바늘생검은 여전히 널리 이용되고 있다. 최선의 검사 정확도를 얻기 위해서는 유도방법과 바늘의 종류 등 검사에 관련된 모든 요소들을 환자의 상태와 병변의 위치에 따라 세심하게 선택하는 것이 중요하다. 합병증을 최소화하기 위해서는 위험인자를 파악하고 고위험군일 경우 가능하면 기관지내시경을 이용한 접근을 먼저 시도해보는 것이 좋겠다.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
References
Peer Reviewers’ Commentary
이 논문은 폐암 진단에 있어 전통적으로 널리 이용되고 있는 비수술적 조직검사 방법인 경흉부 바늘생검에 대해 최신 문헌을 토대로 정리한 논문이다. 최근 고령화와 함께 국가 폐암 검진사업의 도입에 따라, 폐암의 발생률이 꾸준히 증가하고 있으며, 주로 중심부보다는 말초 폐 부위에서 더 많은 폐암과 폐결절이 진단되고 있다. 이러한 상황에서 경흉부 바늘생검은 말초 부위 폐병변과 폐암을 진단하기 위한 매우 중요한 진단 기법이다. 특히 이 논문에서는 경흉부 바늘생검의 시행 방법과 그에 따른 진단율, 발생 가능한 합병증에 대하여 자세하고 체계적으로 설명하고 있어, 폐암을 진료하는 임상 현장에 많은 도움이 될 것으로 판단된다.
[정리: 편집위원회]