슬개대퇴 관절 질환
Patellofemoral joint disorders
Article information

Trans Abstract
Background
Patellofemoral joint problems refer to a spectrum of conditions affecting the patellofemoral joint, which is the joint between the patella and femur. These conditions can cause pain and instability in the knee and affect an individual’s ability to perform daily activities. Patellofemoral joint problems commonly cause knee pain, particularly among young athletes and physically active individuals. This review article discusses current patellofemoral joint problems, including their epidemiology, pathophysiology, diagnosis, and management.
Current Concepts
Patellofemoral joint problems are presented as clinical symptoms of pain and instability. Dividing the diagnostic criteria into anterior knee pain, patella instability, and patellofemoral arthritis is useful. Anterior knee pain is diagnosed after excluding possible causes. Patellar instability is classified into recurrent dislocation, habitual dislocation (extension and flexion types), and permanent dislocation. Moreover, patellar instability can progress to the final stage of patellofemoral arthritis. Thus, patellar instability should be treated according to the Dejour criterion, and patellofemoral arthritis treatment requires artificial joint replacement surgery.
Discussion and Conclusion
The pathological mechanism of patellofemoral joint problems still needs to be properly established, and multifactorial causes make it difficult to treat patellofemoral joint problems. Accurate diagnosis is considered an essential factor for successful treatment.
서론
슬개대퇴 관절은 하지의 움직임을 조절하는 중요한 구조물 중 하나로, 다양한 원인으로 인해 문제가 발생할 수 있다. 슬개대퇴 관절의 문제에 대한 이해는 치료 및 예방 전략을 개발하는 데 중요한 역할을 할 수 있기에, 이 논문에서는 과거부터 최신에 이르는 연구결과를 재고하여, 슬개대퇴 관절에 발생하는 문제에 대해 이해를 넓히고, 임상적인 의사 결정과 치료 계획 수립에 도움을 주고자 한다. 슬개대퇴 관절의 증상은 2가지로 대별할 수 있는데 통증과 불안정성이 다. 두 가지 증상이 혼합되어 있는 경우가 대부분이지만 진단과 치료를 고려할 때, 환자 적용 시 나누어 접근하는 것이 도움이 된다.
슬개대퇴 관절의 문제로 인해 나타나는 임상적 현상은 통증과 불안정성으로 대별할 수 있지만 임상적 접근의 편의를 위해서 (1) 전방 슬관절 통증(anterior knee pain, AKP), (2) 슬개골 불안정성(patellar instability), (3) 슬개대퇴 관절염으로 나누어 기술하고자 한다. AKP와 슬개대퇴 관절염의 범주가 통증을 일으키는 주원인이 될 것이고, 슬개골 불안정성 범주는 불안정성에 대한 내용을 주로 포함할 것이다.
전방 슬관절 통증
AKP는 진단명이 아니고 가능한 진단이 배제된 후에 남는 환자군에 대한 기술이라고 이해되고, 정확한 원인도 모르고, 그로 인해 치료도 할 수 없는 상태로 향후 실체 규명을 위한 연구가 필요한 상태이다.
AKP 원인 규명을 위한 역사적 연구를 보면, 1960년대까지 연골연화증(chondromalacia)을 AKP의 원인으로 간주하고 상호 연관성을 찾으려 노력했지만, 현재로는 연관성이 없는 것으로 생각된다[1,2]. 1970년대 연구에서는 AKP가 슬개대퇴 부정정렬(patellofemoral malalignment, PFM)과 관련이 있다고 생각되었다[3,4]. PFM은 슬개골의 비정상 활주(maltracking), 외측 전위(lateral displacement) 및 외측 경사(lateral tilting)로 나타나게 된다. 슬개외측과압력증후군(excessive lateral pressure syndrome)으로 불리는 질환도 이의 한 유형으로 볼 수 있다[5]. 1970년대 말에는 하지의 부정정렬이 AKP를 유발할 수 있다고 생각하고, 치료로 이에 대한 교정을 시도하였다[6]. 1990년대에는 tissue homeostasis theory [1,7]로 AKP를 설명하려는 시도가 있었으며, 관절을 기계적 구조물이 아니라 신진대사가 이루어지는 활성화된 구조물로 보고, 관절에 영향을 주는 부하 강도와 빈도가 증가하게 되면, 관절의 조직 항상성에 이상을 초래하게 되고, 결과로 통증이 유발된다는 가설이다. 그 외에 신경 모델(hyperinnervation into the lateral retinaculum) [8], 혈관 모델(ischemia) [9] 등을 들 수 있다.
여러 가지 가설이 있다는 것은 한가지 원인이 아니라 여러 원인이 작용하여 증상을 나타낼 수 있다고 결론지어지며, 슬개대퇴 관절에 가해지는 과부하와, 불안정성이 연골 손상과 관절염을 일으키고, 통증으로 이어지는 기전으로 요악할 수 있다(Figure 1). 여러 요소를 감안하면 진단과 치료에 도움을 받을 수 있을 것으로 생각된다.
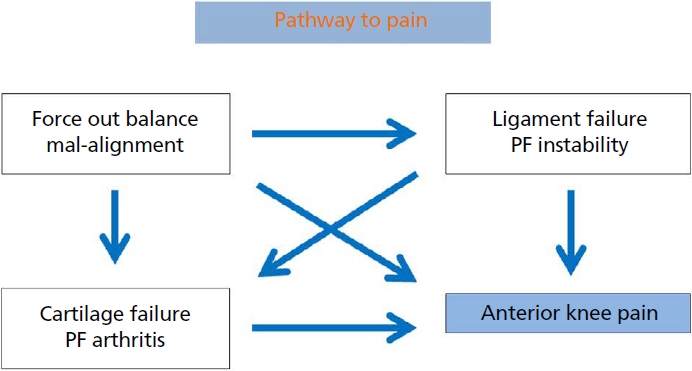
Pathways to anterior knee pain in patellofemoral joint problems. PF, patellofemoral. Illustrated by the authors.
슬개골 불안정성
슬개골 불안정성은 슬개대퇴 관절의 접촉면이 소실되는 완전 탈구(dislocation)가 일어나는 경우와 주관적으로 슬개골을 외측으로 전위 유발 시 불안감을 느끼는(apprehension test 양성) 경우이지만 임상적 탈구의 발생은 없었던 경우로 나눌 수 있다. 후자의 경우는 다른 탈구 위험인자를 1-2개 가지고 있지만 탈구 과거력은 없는 경우이다[10-12].
슬개골 탈구(patellar dislocation)는 3가지 임상 양상을 나타낸다. (1) 재발성 탈구(recurrent dislocation or episodic patellar dislocation), (2) 습관성 탈구(habitual dislocation), (3) 영구적 탈구(permanent dislocation )이다. 재발성 탈구는 간헐적으로 탈구가 일어나는 경우이고, 습관성 탈구는 무릎 관절 운동 시마다 탈구가 일어나는 경우로, 신전 시 탈구가 일어나는 경우와 굴곡 시 탈구가 일어 나는 경우 두 가지 경우가 있다. 일반적으로 슬개골 탈구 시 보이는 J 징후(J sign)는 신전 시 외측 슬개골 탈구가 일어나고 굴곡 시 정복되는 경우이고, 슬개골 궤적이 J 모양을 뒤집어 놓은 형상을 보인다(Figure 2) [13]. 운동학적 역동 컴퓨터단층촬영(kinematic and dynamic computed tomography)을 이용하면, 슬개골 궤적을 이미지화할 수 있는데 신전 형 외측 탈구(Figure 3A)와 다르게 굴곡 형 외측 슬개골 탈구의 경우는 굴곡이 진행하면서 외측으로 탈구가 진행되고, 신전 시 정복이 관찰된다(Figure 3B) [14].

Illustration showing the J sign. The arrow line delineates the inverted ‘J’ path the patella takes. Illustrated by the authors.
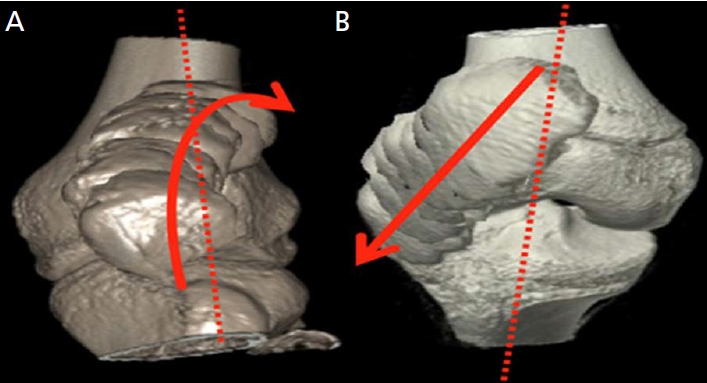
Dynamic kinematic computed tomography of right knee. (A) The arrow shows inverted ‘J’ path of the patella (J sign) in extension type. (B) In flexion type, lateral dislocation progresses as flexion progresses, and reduction is observed during extension. Adapted from Tanaka MJ et al. Blog: the evaluation of patellar maltracking 2017, according to the Creative Commons license [14].
슬개골 불안정성의 분류로는 Chotel 등[15]이 제안한 방법을 사용하는 것이 이해가 쉽고 치료에 적용하기가 용이하다. 소아 환자에 주로 적용이 되지만, 성인에서도 적용할 수 있다. 5개의 군으로 나누어 볼 때, 상부로 갈수록 병변이 중하고 사두근 구축이 심한 반면, 하방으로 내려 갈수록 병변의 고착 정도가 경하여 좋은 예후가 기대된다(Figure 4).
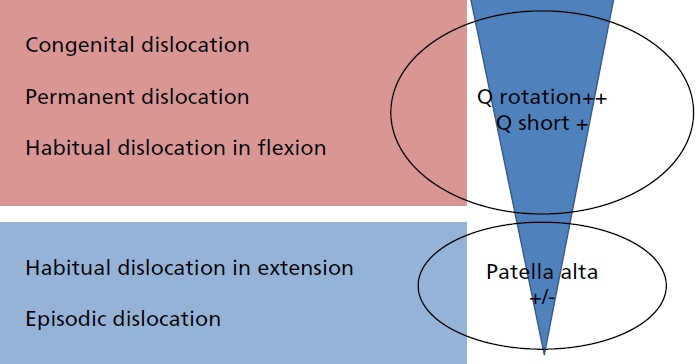
Chotel’s classification of clinical patterns of patellar instability in children and adolescents. Severe dislocation with shortness of the quadriceps (dark frame) is distinguished from minor instability occurring near full extension. Illustrated by the authors.
슬개골 불안정성을 유발하는 원인에 대해 Dejour의 4가지 분류가 치료를 결정하는 데 도움이 된다[16]. 활차 이형성증(trochlear dysplasia), 슬개 경사(patellar tilt), 슬개 고위증(patellar alta), TT-TG 거리 이상(tibial tuberosity-trochlear groove distance)에 따라 활차 성형술(trochleoplasty), 외측 지대 유리술(lateral retinacular release), 경골 결절 원위 전이술(tibial tuberosity distal transfer), 경골 결절 내측 전이술(tibial tuberosity medial transfer)을 고려할 수 있다(Figure 5) [17].

An algorithmic approach to the recurrent patellar instability. TT-TG, tibial tuberosity-trochlear groove distance; TT, tibial tuberosity. Illustrated by the authors.
외상성 슬개골 탈구의 주원인인 내측 슬개대퇴 인대(medial patellofemoral ligament) 손상 시 내측 슬개대퇴 인대 재건술(medial patellofemoral ligament reconstruction)을 시행하는 것이 기본 치료이고, 내측 중첩술(medial reefing)도 선택적 치료가 될 수 있다.
슬개대퇴 관절염
슬개대퇴 관절염(patellofemoral osteoarthritis, PFOA)은 슬관절 내측 및 외측에 국한된 관절염에 비해 빈도는 적으나 55세 이상의 연령에서 남자는 11%, 여자는 24%의 유병률을 보인다[18]. 증상 유무에 따라 분석한 결과, 20세 이상 연령군의 무증상군에서는 유병률 25%를 보인 반면, 30세 이상의 유증상 연령군에서는 39%의 유병률을 보여[19], 증상이 없이 발생하는 경우도 흔하다는 것을 알 수 있다. 발명 원인에 대해서는 논란이 많고, 대부분은 특발성(49%, idiopathic)이지만, 동반 병변으로 객관적 슬개골 불안정(33%), 후외상성 병변(9%), 연골석회화증(8%, chondrocalcinosis)이 관찰된다[20].
PFOA 자연 경과(natural history)에 대한 연구는 문헌 보고가 적어, 결론적 근거를 찾기가 어렵다. 다만 경대퇴 관절염(tibiofemoral osteoarthritis, TFOA)과의 상호 연관성은 보고되고 있으며, TFOA를 가지고 있는 환자에서 3년 내 PFOA로의 발생 및 진행되는 위험요소로 작용할 수 있다. PFOA가 TFOA의 위험요소로 작용한다는 근거도 방사선 연구를 통해 보고되고 있다[21,22]. 수술적 치료에 대해서는 2개의 범주로 나누어 생각할 수 있는데, (1) 정상 해부학적 슬개대퇴 관절의 구조를 갖는 PFOA, (2) 비정상적 해부학적 구조를 갖는 PFOA로 활차 혹은 슬개골의 이형성증(dysplasia)이나 슬개대퇴 관절의 부정정렬이 동반된 경우이다. 전자의 경우는 보존적 치료에도 증상 호전이 없을 때 인공관절 부분 치환수술(patellofemoral arthroplasty) 혹은 고령에서 인공관절 전치환수술(total knee arthroplasty)을 시행할 수 있다. 해부학적 이상을 동반한 두 번째 경우는 인공관절 치환수술과 함께 비정상적 요소를 교정할 수 있는지의 판단이 중요할 것 같다.
슬개대퇴 관절 관련된 최신 보고들
슬개대퇴 관절의 문제 발생 시, 통증과 불안정성이 나타나는데, 증상에 대한 치료 전 후 평가를 위해 환자 보고 결과 측정(patient-reported outcome measures)이 중요 요소로 슬개대퇴 관절에서 발생하는 특이 증상만을 반영할 수 있는 지표가 필요한 데, 이를 만족시키는 평가지표는 개발이 필요한 상태이고[23], knee injury and osteoarthritis outcome score-patellofemoral subscale 점수가 타당성이 높다고 제안되고 있다[24]. 증상 치료는 보존적 치료로 시작되며, 근력 강화의 관점에서 슬관절 근위부의 근력이 강화되었을 때, 슬관절 원위부보다 증상 완화에 효과적이라 보고된다[25-27]. 다양한 위치의 테이핑 치료 효과는 증상 호전을 보고하고 있어[28,29], 치료 방법으로 고려될 수 있다. 스쾃 운동(squat exercise)은 슬개대퇴 관절에 부하를 높이므로 hip thrust 운동이 유리하다고 권장된다[30]. 최근 홈프로그램이 발전하고 있어 이를 이용하면[31,32], 환자 교육에 도움이 될 것으로 생각된다.
보존적 치료에 반응하지 않는 환자에 있어서, 수술적 치료를 고려하게 되는데, 슬개골의 비정상 활주를 교정하는데 주목하게 된다. 주원인은 슬개골 슬개대퇴 인대의 파열 및 약화로, 이에 대한 치료는 내측 슬개대퇴 인대 재건술을 중심 치료로 시행하고, 추가적으로 주위 변형을 교정하는 수술을 병행할지를 추가하는 방향으로 진행되고 있다[13].
결론
슬개대퇴 관절의 문제는 동통과 불안정성의 임상적 증상으로 나타나는데, 이에 대한 진단적 접근은 전방 슬관절 통증, 슬개골 불안정성, 슬개대퇴 관절염으로 나누어 적용하면 도움이 된다. 전방 슬관절 통증은 가능한 원인을 제외한 후 얻어지는 증상 복합적 진단이다. 슬개골 불안정성은 재발성 탈구, 습관성 탈구 (신전형과 굴곡형), 그리고 영구적 탈구로 구분된다. 최종단계는 슬개대퇴 관절염으로 진행하게 된다. 치료는 Dejour 분류에 따라 진행을 하고, 슬개대퇴 관절염은 인공관절 치환수술이 필요하게 된다. 정확한 진단이 최우선이며, 성공적 치료를 얻어낼 수 있는 중요 요소이다.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Acknowledgements
I would like to express my sincere gratitude to Hyung-Jin Yoon for their invaluable assistance in creating the figures for this paper.
References
Peer Reviewers’ Commentary
이 논문은 슬개대퇴 관절의 문제로 인해 무릎 통증과 불안정성을 유발하는 질환들인 전방 슬관절 통증, 슬개골 불안정성, 슬개대퇴 관절염의 3가지에 대하여 최신문헌을 정리하여 기술해주고 있다. 전방슬관절 통증은 통증을 유발할 수 있는 다른 질환들을 배제한 임상적 진단명이며, 원인이 아직 불명확하나, 현재까지 제기된 가설 및 기전을 정리하여 이해하기 쉽게 기술하였다. 슬개골 불안정성의 원인과 이에 따른 치료는 다양한데, 정립된 몇 가지 분류를 통해 치료 방법을 결정할 수 있도록 기술하였다. 슬개대퇴 관절염은 해부학적 이상 여부에 따른 치료를 제시해주었으며, 그 외 슬개대퇴 관절의 증상과 기능을 반영할 수 있는 임상 평가 지표를 소개하고 있다. 이 논문은 무릎 통증 관련 환자를 진료하는 임상 현장에 많은 도움이 될 것으로 판단된다.
[정리: 편집위원회]