조현병 진단기준에 대한 정신병리학적 고찰
Psychopathological consideration of the diagnostic criteria for schizophrenia
Article information

Trans Abstract
Background
Considering the conterarguement of the optimistic attitude of psychoanalysis and environmental change, the current diagnostic criteria for schizophrenia (i.e., Diagnostic and Statistical Manual of Mental Disorders, 5th edition-text revised [DSM-5-TR], International Classification of Diseases, 11th revision [ICD-11]) are defined under the substantial influences of symptom-based operationalism. The current diagnostic criteria for schizophrenia are occasionally considered as the incorporated characteristic mixtures of the chronicity, positive symptoms, and negative symptoms of Emil Kraepelin, Kurt Schneider, and Eugen Bleuler, respectively.
Current Concepts
Concerning the diagnostic criteria for schizophrenia, the two remarkable changes from DSM-IV or DSM-IV-TR to DSM-5 or DSM-5-TR are as follows. First, related to diagnosing schizophrenia, the weighting of Kurt Schneider’s first-rank symptoms has been omitted. Second, the defining subtypes (i.e., paranoid, disorganized, undifferentiated, catatonic, and residual) have also been omitted. In addition, catatonia has been newly considered a semi-independent diagnostic entity in DSM-5 or DSM-5-TR. Therefore, from a psychopathological aspect, the operationally defined diagnostic criteria for schizophrenia display several limitations: First, the oblivion of the concept of formal thought disorder, considered as the fundamental symptom of schizophrenia by the greatest psychopathologists, has been deepened. Second, the current diagnostic criteria for schizophrenia have been partly inconsistent with the disease essentialism model.
Discussion and Conclusion
Schizophrenia cases are interconnected with ‘family resemblance’ but not shared by common underlying neurobiological correlates. Herein, in clinical psychiatric practice, with an emphatic approach, phenomenological psychopathology would still be required to evaluate the subjective experiences of an individual with schizophrenia.
서론
조현병을 어떻게 정의할 것인가? 이 논쟁은 정신의학에서 오랫동안 지속되어 왔다. 이러한 질의는 조현병의 진단단위에 국한해서 협의의 수준에서 논의하는 것으로부터 정신의학의 과학적 기초에 대한 보다 근본적인 논쟁을 제시하기까지 광범위하다. 조현병의 증상중심 진단기준은 인식론적으로 불완전하다는 평가를 받고 있다. 그간 생물정신의학 연구가 60년간 집중적이고 지속적으로 이뤄졌음에도, 신경학적으로 구분하는 것은 여전히 그 경계가 불명확하며, 임상적으로도 임의적인 수준에 머물러 있는 수준이다[1,2]. “여전히 최종적인 검사로 조현병을 진단할 수 없고, 조현병 구균(Schizococuss)을 동정하지 못했으며, 질병 유무를 판정할 수 있는 영상검사도 없다”라고 기술하기도 했다[3]. 그렇기에 조작주의 관점을 토대로 한 증상중심 조현병 진단구성은 자연적 종(natural kind)에 해당하는 것이라기보다는 인지적 구성체(cognitive construct)에 상응하는 것이므로[4], 대안적 혹은 보완적 방법론의 고려가 필요한 실정이다. 한편, 조작주의라 함은 개념을 이에 대응하는 조작들(operations)의 집합과 동의어로 정의하는 것을 의미한다[5]. 이 논문에서는 미국정신의학회(American Psychiatric Association)가 공표한 일련의 정신질환의 진단 및 통계 편람(Diagnostic and Statistical Manual of Mental Disorders, DSM)에서 조현병 진단위의 구성체와 그 변화를 고찰하고자 한다.
조작주의 진단구성
Table 1과 같이 2013년과 2022년에 각각 공표된 DSM-5과 DSM-5-TR은 모두 조현병 진단구성을 다음과 같이 정의하였다[6-11]. 증상에 관한 기준은 (1) 망상, (2) 환각, (3) 와해된 언어, (4) 와해되거나 긴장병적인 행동, (5) 음성증상 등 5가지 증상 중 2가지 이상이 1개월 이상 지속되는 동시에, 망상, 환각, 와해된 언어 등 3가지 증상 중 1가지 이상은 필수적으로 존재해야 함을 제시한다. 또한 사회적 및 직업적 기능손상이 동반되어야 한다. 위의 5가지 증상 중 2가지 이상이 적어도 지속되는 기간이 1개월 이상이면서 전구증상 및 잔여증상을 포함하는 기간이 6개월 이상이어야 한다. 마지막으로, 조현정동장애, 기분장애, 물질사용장애, 발달장애 등을 감별하여 진단하기 위한 항목이 있다[10,11]. DSM-5과 DSM-5-TR의 조현병 진단기준이 DSM-IV과 DSM-IV-TR으로부터 개정된 사항은 다음과 같다. 첫째, 증상중심 기준에서 망상이 기이하거나 환각이 개인의 행동이나 생각에 대해 지속적으로 논평하는 목소리이거나 서로 대화하는 두 명 이상 목소리일 때는 단지 1가지 증상만 있어도 된다는 쿠르트 슈나이더(Kurt Schneider)의 일급증상(first-rank symptoms)에 대한 가중치 조항을 삭제한 것이다[12,13]. 일급증상에 대한 가중치 조항은 그 이전 DSM-III 및 DSM-III-R의 공표 당시 조현병 진단기준 내에 처음으로 직접적으로 포함되었다[14]. 쿠르트 슈나이더는 가청사고(audible thought), 대화환청(voice discussing) 혹은 논쟁환청(voice arguing), 논평환청(voice commenting), 신체피동체험(somatic passivity experiences), 사고탈취(thought withdrawal), 사고주입(thought insertion), 사고전파(thought broadcasting), 망상적 지각(delusional perceptions), 조종망상(delusion of being controlled) 등을 일급증상으로 정의하면서, 이 중에서 단지 한 가지라도 있으면 조현병으로 진단할 수 있다고 역설하였다. 일급증상은 자신의 사고, 감정, 신체를 피동적으로 지각하는 것을 공통적인 속성으로 하는데, 증상의 유무로 양분화하여 평가한다[15]. 코크란 데이터베이스 체계적 문헌고찰 결과를 살펴보면, 일급증상으로 75% 이상 조현병 환자에 대해서는 적절하게 진단할 수 있었지만, 20% 미만으로 다른 정신질환 환자에 대해서 조현병으로 잘못 진단했다고 보고하였다. 한편, 일급증상의 조현병 진단에 대한 민감도는 60% 정도로 산출되었다. 이에 일급증상을 이용한 조현병의 진단은 전문가에 의한 감정이입을 통한 접근이 필수적이라고 결론을 내렸다[16]. DSM-5-TR 등 현재 보편적으로 사용되고 있는 조현병 진단기준에서 일급증상에 대해 더 이상 가중치를 부여하지 않는 것은 이러한 경향을 반영한 것이라고 볼 수 있다. 하지만 DSM이 일급증상의 숫자와 성격에 대한 개정이 진단의 민감도 전반에 부정적인 영향을 미쳤을 가능성이 있으며, 애초에 원래 슈나이더가 역설했던 개념을 그대로 적용한다면 그 결과가 달라졌을 것이라는 반론도 있다[17]. 둘째, 편집형, 와해형, 긴장형, 미분화형, 잔류형 등 유형(subtype)의 구분에 대한 항목을 삭제하고, 그 중에서 긴장증(catatonia)을 준독립적인 진단단위로 개별화하여 정의하였다[12,13]. 조현병 진단구조는 이미 한 세기 이전에 확립된 것으로, 그 이래로 유형이라는 개념을 상정하여 조현병의 이질성을 질병분류학적으로 설명하고자 했다. 하지만 DSM-IV의 임상실제 적용에서, 유형은 그 신뢰도가 빈약하고 시간경과에 따른 안정성이 낮으며 예후를 시사하는 가치가 그다지 높지 않다고 알려졌다. 조현병 유형을 질병분류학적으로 식별하기 위해 시도한 군집분석 결과는 일관되게 DSM의 유형과 부합하지 않았다[12,13]. 유형을 분류하는 조항의 삭제는 조현병 개념에서 파과증(hebephrenia) 등과 같은 비편집형 조현병(nonparanoid schizophrenia)의 하위 범주는 점진적으로 사라지게 하고 현상학적 전체상(phenomenological Gestalt)은 잊혀지게 하여, 오직 만성적인 망상-환각 증후군(chronic delusional-hallucinatory syndrome)만을 남게 하여 그 진단단위를 협소화한다는 비판도 있다[17].

DSM-III의 증상중심 조작주의 진단체계의 시작은 DSM-I 및 DSM-II이 견지했던 정신분석학적 태도 및 환경 개선을 통한 낙관주의 관점에 대한 반성으로부터 출발했다고 해도 과언은 아니다. 그 결과, DSM-III는 조현병이 아닌 ‘조현병적 장애(schizophrenic disorder)’라고 명명하였는데, 이러한 반성의 태도를 반영한 것으로 여겨진다[18]. Table 2와 같이 1952년에 공표되었던 DSM-I [19]은 진단단위를 조현병이 아닌 ‘조현병적 반응(schizophrenic reaction)’으로 명명하였고 다음과 같이 정의하였다.

이 용어는 이전에 사용된 조발성 치매(dementia praecox)라는 용어와 동의어이다. 이는 다양한 정도 및 혼합을 나타내는 정동, 행동, 및 지적장애와 함께 현실관계 및 개념 형성의 근본적인 장애를 특징으로 하는 일련의 정신병적 반응을 의미한다. 이 장애는 현실로부터 후퇴하려는 강한 경향, 정서적 부조화, 사고과정에서 예측할 수 없는 방해, 퇴행적인 행동이 특징이고, 일부에서는 ‘퇴행화’ 경향이 특징이다. 주요한 증상은 그러한 환자를 유형으로 분류하는 결정적인 요인이다.
한편, Table 2와 같이 1968년에 공표된 DSM-II [20]는 진단단위를 조현병으로 명명하였고 다음과 같이 정의하였다.
이 범주는 사고, 기분 및 행동의 특징적인 장애로 발현되는 일군의 장애를 포함한다. 사고장애는 실제에 대한 오인이나 망상과 환청을 초래할 수 있는 개념형성에서의 변화를 의미한다. 이러한 양상은 빈번하게 심리학적으로 자기 보호적인 양상이 나타난다. 결과적으로 기분변화는 양가적이고 제한적이며 부적절한 감정반응 및 타인에 대한 공감의 결여를 포함한다. 행동은 철퇴적이고 퇴행적이며 기이할 수 있다. 조현병은 정신상태가 기본적으로 사고장애로 귀인될 수 있으므로 주요정동장애는 기분장애가 두드러지는 것으로부터 구분할 수 있다. 편집증 상태는 실제에 대한 왜곡이 협소하고 다른 정신병 증상이 결여한 것으로 조현병과 구분할 수 있다.
하지만 DSM-II이 공표된 이후에, 당시 그에 대한 불만족이 점진적으로 증가했던 것으로 알려져 있는데, 조현병 진단이 함부로 남용되는 경향이 그 단적인 예이었다. 또한 당시 정신의학은 반정신의학 운동, 동성애에 대한 논란, 탈원화 경향, 로젠한 실험(Rosenhan experiment) 등으로부터 다양한 형태의 위기를 직면했었다[21]. 로젠한 실험은 건강한 성인 8명이 정신병 증상을 거짓으로 흉내 낸 이후 조현병 등으로 진단을 받고 미국 5개주 12개 정신병원에 입원한 것을 주요내용으로 하는 연구였다. 그리고 그 결과를 1973년 학술지 사이언스(Science)에 ‘비정상적인 장소에서 제정신인 것에 대해(On Being Sane in Insane Places)’라는 제목 하에 공표했다[22]. 이러한 여건 속에서 진단단위의 신뢰도와 타당도 향상을 위해 고정적이고 표준화된 진단단위를 확립하는 것이 무엇보다도 시급했는데, Feighner 기준은 조작주의 기준을 도입함으로써 진단을 급진적으로 간략화하여 개별환자에게 특정진단을 부여할 수 있는 접근을 도출하였다. 그리고 연구진단기준(research diagnostic criteria)을 Feighner 진단기준의 영향을 받아 개발하였다[23]. 그 결과, 1980년에 공표된 DSM-III는 에밀 크레펠린(Emil Kraepelin)의 범주 개념을 도입하였는데, 이러한 경향을 신크레펠린 학파(neoKraepelinian credo)라고 명명하기도 하였다. 하지만 현재의 조현병 진단구조는 몇 가지 문제점이 있었다.
형식적 사고장애의 점진적인 소멸
오이겐 블로일러(Eugen Bleuler)는 형식적 사고장애(formal thought disorder)를 조현병에 대한 질병 특이적인 증상으로 간주하였다. 사고장애는 논리적인 규칙의 잠재적인 붕괴에 따른 개념형성의 장애를 의미한다. 만성화된 조현병 환자는 극명한 형식적 사고장애를 상대적으로 흔히 나타내지만, 급성기 환자는 그렇지 않은 경향이 있다. 형식적 사고장애는 언어내용의 빈곤, 목표상실, 음운연상, 지리멸렬, 이해불가능 등으로 나타날 수 있다. 조현병 환자에서 사고 과정의 장애는 언어를 통해 나타나게 되는데, 역으로 의사소통의 장애를 조현병을 정의할 수 있는 특징적인 증상으로서 개념화할 수 있다[24-28]. 사고장애의 정의는 쉽지 않은데, 형식적 사고장애를 조현병에서 나타나는 다양한 언어의 이상성을 반영하는 용어로서 제안하기도 한다. 일례로, 형식적 사고장애는 다음과 같이 설명되기도 한다[29].
이 용어는 의심할 여지없이 본질적으로 완전히 다른 다양한 이상성을 포함하고 있다. 아마도 가장 흔하게는 잘못되어 있는 관념의 논리적인 배열일 것이다. 다른 때에는 개별적인 단어와 구의 의미가 모호해지도록, 언어 생성의 기전 그 자체가 장해가 있는 것처럼 보인다. 또 다른 때는 잘못이 담화의 수준에서 발생한 것처럼 보인다; 개별적인 단어, 문장, 사고의 배열은 의미가 통하지만, 더 이상의 언어 생성에 대한 인식할 수 있는 맥락은 없다.
고전적인 정신병리학은 형식적 사고장애를 조현병 진단을 위한 일차적인 증상으로 간주했다. 빌헬름 그리징어(Wilhelm Griesinger)는 지리멸렬(Inkohärenz)이 내용의 유사성이나 상이성이 아닌 단어에서 음소의 유사성에 의존하여 발생하는 것을 관찰하면서, 그것이 대뇌반구 간 상호작용의 결핍으로부터 유래할 것으로 추정하였다[30]. 에밀 크레펠린과 오이겐 블로일러는 조현병 환자에서 말과 언어의 이상성을 개별적으로 개념화하였다[31-33]. 크레펠린은 사고의 연쇄고리가 내부 혹은 외부에서 그 연결이 상실되거나 내부적인 통합성을 상실하는 것을 ‘Zerfahrenheit(독일어로 산만함을 의미)’라는 용어를 이용하여 정의하였다. 그리고 그것을 조발성 치매의 특징적인 양상으로 설명하였다. Zerfahrenheit가 조현병의 사고 및 언어장애의 전형적인 형태라고 상정할 때, 지리멸렬은 기질성 정신장애의 특이적인 언어현상에 대한 명백한 정의라고 할 수 있다[34]. 오이겐 블로일러는 ‘연상의 이완(loosening of associations)’을 조현병의 가장 근본적인 정신병리 기전으로 인식하였다. 오이겐 블로일러는 다른 기능을 담당하는 ‘정신(φρήν; mind)’ 사이의 ‘분리(σχίζειν; split)’를 의미하는 ‘schizophrenia’를 조발성 치매를 대신하는 용어로서 처음으로 제안하였다. 오이겐 블로일러는 연상의 이완을 다음과 같이 설명하였다[32].
연상은 그 연속성을 상실한다. 이 병에서는 생각을 안내하는 수천 가닥의 연상 중에서 때로는 한 가닥이, 때로는 큰 부분이, 때로는 전체집단이 완전히 무계획적으로 방해를 받는 것처럼 보인다.
연상의 이완은 연상 간 연결성이 그래도 유지되는 것을 지시하는 반면에, ‘Zerfahrenheit’는 연상의 합리적인 관련성이 부재하는 것을 구분하여 지시한다. Table 2와 같이 DSM-I은 조현병을 기술함에 있어 개념형성을 근본적인 장애로 상정하고 있고, DSM-II는 개념형성에서의 변화가 이차적으로 망상이나 환청을 초래할 수 있음을 반영하였다. DSM-I와 DSM-II는 개념형성에서의 변화를 망상이나 환청 등의 기저 병리이며 조현병의 일차적인 증상으로 명백하게 상정하였다. Table 1과 같이 DSM-III와 DSM-III-R은 조현병 진단기준 내에 지리멸렬 또는 연상의 이완을 형식적 사고장애에 상응하는 증상항목으로서 포함하였다. 그런데 지리멸렬이나 연상의 이완을 망상이나 환청 등 정신병 증상 및 징후와 병렬적으로 나열함으로써, 개념형성에서의 장애가 조현병의 근본적인 증상으로서 이전에 평가받았던 위상이 상대적으로 떨어지는 결과를 낳았다. 에밀 크레펠린과 오이겐 블로일러의 개념이 각각 반영된 것으로 평가받기도 하지만, 서로 이질적인 두 개념을 마치 하나의 형태로서 취급하고 단순히심각도 차이만으로 구분할 수 있다고 쉽사리 단정해버린 한계점이 있다. 결국 에밀 크레펠린의 Zerfahrenheit가 조현병 증상학에서의 중심적인 위상을 상실하게 된 것이라고 평가받았다. DSM-IV 및 DSM-IV-TR는 지리멸렬이나 연상의 이완을 ‘와해된 언어’와 등가적인 것으로 간주하면서 지리멸렬이나 연상의 이완을 대신하였다. 와해된 언어는 형식적 사고장애로서 비교적 관찰이 용이한 현상을 의미하는데, 그 예로서는 탈선(derailment)과 지리멸렬을 제시하였다. ‘와해된 언어’는 DSM-5 및 DSM-5-TR도 그대로 사용하고 있다[34].
한편, 클라우스 콘라트(Klaus Conrad)는 그의 저서 ‘조현병의 시작(Beginnede Schizophrenie)’에서 아래와 같은 가정을 제시하였다[35].
조현병이라는 병은 분명한 체험으로서, 인간과 동물을 구별하는 중심핵을 침입한다. 그것은 ‘나’와 ‘초월’이라는 반성능력이다. 이렇게 생각해보면, 조현병 기반의 물질적 변화를 어디에서 구하면 좋을지에 대해 하나의 힌트를 얻을 수 있다. 그것은 인간의 뇌를 유인원의 뇌와 구별한다. 인간에게 특이적인 뇌 조직의 기능 변화에 관계하고 있을 것이다. 그것은 반드시 국소적인 것은 아니고 국소적으로 존재할 수도 없다.
이러한 맥락에서, 쿠르트 슈나이더의 일급증상는 언어의 대뇌양반구 조정과정, 그 중에서도 ‘나’와 ‘너’를 구별하는 ‘지표화(indexicalization)’ 과정의 붕괴를 반영하는 의의를 지니고 있는 것으로서 형식적 사고장애의 관점에서 재정의될 수 있다[36,37]. 예를 들어, 언어와 정신병의 공통된 기원을 상정하는 문헌은 일급증상에 대해 다음과 같이 가설을 제시하기도 하였다[38].
슈나이더의 일급증상은 ‘언어적인 한계의 끝에 있는 언어’로서 기술될 수 있다; 따라서 조현병의 일급증상 증후군이 지니는 증상학 및 인구학 특징은 인간이라는 종의 기원을 밝힐 수 있는 실마리를 제공해 줄 것이다.
DSM-5와 DSM-5-TR은 조현병 진단기준에서 일급증상의 잠재적인 진단적인 가중치에 관한 항목을 삭제하였다. 조현병적 기저기분(Schizophrenie Grundstimmung), 존재의 변화된 양식(changed modality of being), 자연적인 체험의 붕괴(breakdown of natural experience), 자연적인 자기근거의 결여(lack of natural self-evidence) 등 현상학적 전체상과의 연결고리가 점진적으로 상실되는 경향이 더욱 진행된 것으로 추정할 수 있다. DSM의 반복적인 개정작업을 통해 조현병이라는 범주가 ‘만성적인 망상-환청 증후군’으로 협소화되며, 개념형성에서의 변화와 망상이나 환청 등 정신병적 증상 간 잠재적인 인과관계가 점진적으로 덜 강조되고, 빌헬름 그리징어, 에밀 크레펠린, 오이겐 블로일러 등 위대한 정신병리학자들이 제안했던 형식적 사고장애 개념들은 현저하게 간소화되고 단순화되는 변화를 거쳤다[39]. 따라서, ‘schizophrenia’는 개념형성에서의 변화를 중심적인 정신병리로서 상정하여 명명하였음에도, 그 진단기준 내에서 형식적 사고장애의 중심적 위상은 점진적으로 약해지고 망상이나 환각 등 정신병적 증상 및 징후는 점진적으로 강해지는 역설적인 상황에 놓여있다고 하겠다.
질병 본질주의 모형과의 괴리
질병 본질주의 모형(disease essentialism model)은 특정한 증상이나 징후가 생물학적 본질유형에 직접적으로 귀속할 수 있다고 상정하는데, 이것은 범주중심 정신질환 진단체계 및 구조의 토대가 된다. 질병 본질주의 모형을 정신의학에 적용할 때, 관찰가능한 증상이나 징후의 이면에서 아직 드러나지 않은 채로 존재하고 있는 등가적인 실재를 발견함으로써, 개별질환을 구분하고 식별할 수 있다고 기대하는 태도를 의미한다. 하지만, 자연적인 경계를 기준으로 정신질환을 구분하는 것은 여전히 요원한 실정이다. 질병 본질주의 모형은 조현병 등 개별질환에서 증상이나 징후가 다양하게 나타남에 따라서, 그 타당성에 대한 의문점을 제기한다[40]. 고전적인 정신병리학은 조현병을 정의하는 속성에 대한 서로 다른 세 가지 관점을 제시하였다. 에밀 크레펠린은 조현병 진단에 대한 구체적인 기준을 제시하지는 않았지만 장기간 경과와 결과의 의의를 중요하게 간주했다. 오이겐 블로일러와 쿠르트 슈나이더는 구체적으로 단면적인 증상기준을 개별적으로 제시하였다. 블로일러는 연상의 이완(associative loosening), 정동의 둔마(affective blunt), 양가감정(ambivalence), 자폐증(autism) 등을 근본적인 증상으로 간주했던 반면에, 슈나이더는 전술한 일급증상을 질병 특이적 증상으로 상정하였다. 그런데, 현재 조현병 진단기준은 크레펠린의 만성화 경과, 블로일러의 음상증상, 및 슈나이더의 양성증상을 적절히 합쳐서 만들어낸 결과물로서 평가를 받기도 한다[41]. 현재 조현병 진단구조는 구성요소의 다양한 조합과 개별요소의 다양한 해석을 고려한다면 그것은 자연적 종보다는 인지적 구성체에 해당하로 엄밀함의 정도가 제한적일 수밖에 없을 것으로 추론한다[4]. 그 결과, 조현병 진단구조는 다차원적 이질성을 필연적으로 내포한다.
철학자 루트비히 비트겐슈타인(Ludwig Wittgenstein)의 견해는 질병 본질주의 모형의 기본전제와 대립했던 것으로 평가받는다. 그는 언어철학 관점에서 ‘단어의 의미와 사용(word meanings given by usages)’, ‘가족유사성과 본질(family resemblance and essence)’, 및 ‘정신과정의 오인(misidentification of mental process)’을 다루었다. 이러한 논의를 통해 특정 정신의학 진단이 특정 정신과정을 지시할 것이라고 단정하는 관점에 대해 비판적인 논의를 제시할 수 있다[42]. 그의 견해에 따르면, 특정한 정신적인 증상과 징후의 집합으로 구성된 ‘정신질환’의 개념 아래에 물질적인 혹은 비물질적인 심오한 실재가 존재한다고 가정하는 것보다는 가족유사성을 적용하여 간주하는 것이 보다 더 효과적일 수 있다. 저서 ‘철학탐구’에서 다음과 같이 기술하였다[43].
예를 들어 우리가 ‘게임’이라고 부르는 것을 한 번 고찰해 보자. 판 게임, 카드 게임, 공놀이, 격투 경기 등에 대해서 말이다. 무엇이 이것들에 공통되는가? 무엇이든 이것들에 공통되지 않으면 안 된다. 그렇지 않으면 그것들을 ‘게임’이라고 말하지 않는다라고 해서는 안 된다. - 이들 모두에게 무엇인가 공통적인 것이 있는가의 여부를 보자. 왜냐하면 그것들을 주시하면 모든 것에 공통된 것이 보이지는 않겠지만 그것들의 유사성이나 연관성을 보고 이들 전체 계열을 보게 될 것이다. 이미 말한 바와 같이 생각하지 말고 보라!
‘게임’이라는 개념은, 윤곽이 흐릿한 개념이라고 말할 수 있다. ‘그러나 흐릿한 개념이 도대체 개념인가.’ 핀트가 어긋난 사진이 도대체 인간의 영상인가? 게다가 핀트가 어긋난 영상을 분명한 영상으로 바꾸어 놓는 것이 항상 좋은 일인가? 초점이 안 맞은 것이야말로 바로 우리가 자주 필요로 하는 것이 아닌가?
조현병은 망상, 환각, 와해된 언어, 와해된 행동, 음성증상 등 DSM 진단기준을 구성하는 증상뿐만 아니라 인지기능저하, 사회적 위축, 불량한 병식, 기분증상, 불안, 운동증상, 경미한 신체적 이상, 연성 신경학적 징후 등 다양한 임상양상을 그 특징으로 한다. 따라서 임상가는 이중에서 몇 가지 특징을 토대로 조현병이라는 진단단위로 정의한다. 예를 들어, 현실검증력을 보존하여 환청을 지속적으로 체험하지만 그것이 환청임을 인식하는 증례, 망상이나 환청은 없지만 추상적 사고의 장애가 있는 증례, 망상이나 환청은 없지만 정신사회적 기능을 적절하게 수행하는 증례 등은 DSM 진단기준에 엄밀하게 부합한다고 할 수는 없음에도 불구하고 흔히 임상가는 조현병이라고 진단을[4]. 조현병으로 진단받은 증례들은 기저의 공통된 신경생물학적 속성이나 기전을 공유하기 보다는 가족유사성으로 연결되어 있다고 간주하는 것이 더 타당하다고 볼 있다. 결국 근본적인 정신과정을 상정할 수 없다는 것은 조현병이라는 진단단위에 일반적으로 실증적이거나 과학적인 설명에 대한 부착점이 주어지지 않았다는 것을 반영한다고 볼 수 있다[44,45].
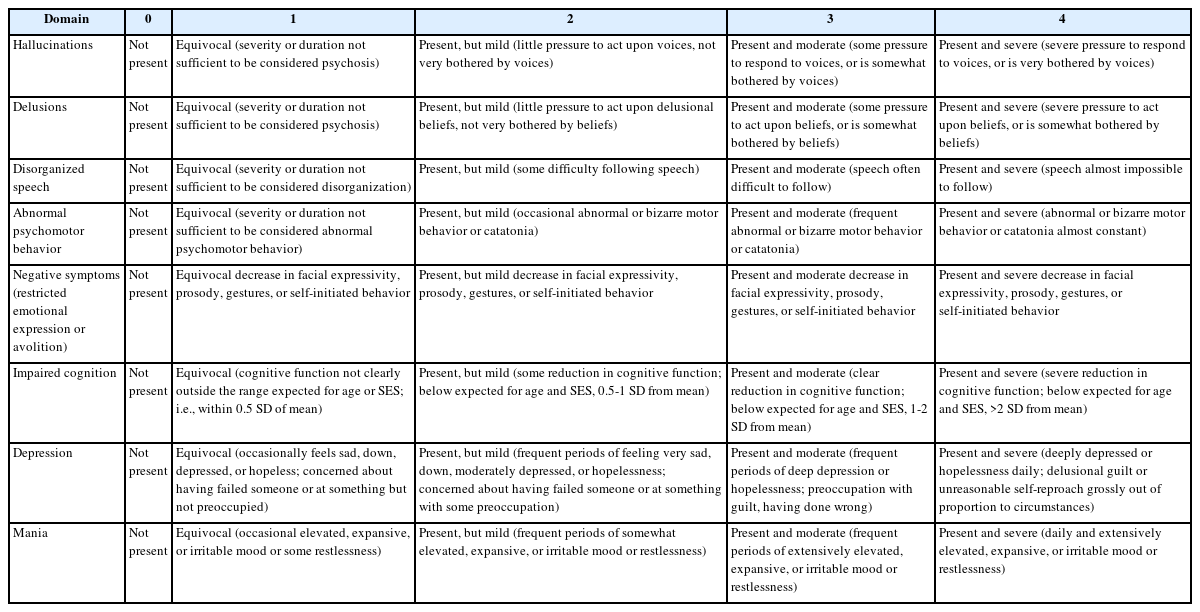
DSM-5 개정을 위한 전문위원회는 조현병 진단기준을 논의하기 위해 ‘정신병 탈구성화(Deconstructing Psychosis)’라는 백서를 편찬하였다. 서론에서는 정신병의 범주적이고 차원적인 표상에 관련한 근거를 평가하고 정신병의 현재 임상적 진단 실제와 자연적 표현형 간 간극을 연결함에 있어 유망한 시도를 제안하는 것이라고 그 목표라고 기술하였다[46]. 특히, 조현병과 양극성장애의 차이는 변연계 회로나 감마아미노뷰티르산(gamma aminobutyric acid, GABA) 세포 통합성 등 내적표현형(endophenotype)에서 두드러지게 나타난다고 서술하였다. 동시에 조현병과 양극성장애의 임상양상 간 유사성은 분자, 세포, 및 신경회로 수준에서 개별적인 내적표현형 간 중복을 시사하는 것이라고도 했다[47]. 이러한 맥락에서, 정신병적 양성증상을 체험하는 사람들이 임상실제에서 조증, 혼란, 정보처리능력 결핍 등 다른 차원에서의 변화도 동반하는 것을 보다 효과적으로 기술하기 위해 ‘일반 정신병 증후군(general psychotic syndrome)’이라는 개념도 제안했다. 일반 정신병 증후군은 정신병리의 범주적 표상을 양극성(bipolar), 발달성(developmental), 및 기타(other)로 구분하였으며, 그 차원적 축은 양성증상, 음성증상, 와해화, 정보처리능력 결핍, 조증증상, 및 우울증상으로 구성되었다[48]. Table 3과 같이 DSM-5 및 DSM-5-TR의 제3부 새로 개발된 평가척도와 모델에는 정신병적 장애의 이질성을 평가하기 위한 도구로서, ‘임상가-평정 정신병 증상 심각도 차원(Clinician-Rated Dimensions of Psychosis Symptom Severity)’을 새로운 임상적 평가도구로 제시하였다. 임상가-평정 정신병 증상 심각도 차원은 환각, 망상, 와해된 언어, 비정상적 정신운동 행동, 음성증상, 우울증, 조증 등 8개 항목으로 구성되어 있으므로, 조현병과 기분장애 간 불분명한 경계와 이로 인한 조현병의 이질성을 간접적으로 반영한 것으로서 볼 수 있다[49].
현상학적 정신병리학의 필요성
낸시 안드레아슨(Nancy Andreasen)은 ‘미국에서 DSM과 현상학의 죽음: 의도하지 않은 결과의 예시(DSM and the Death of Phenomenology in America: An Example of Unintended Consequences)’라는 논문을 통해, DSM-III 이후의 진단구조 내에 실증주의 및 조작주의 태도가 강화됨에 따라서 나타나는 문제점을 다음과 같이 지적하였다. 첫째, 진단기준은 특정한 질환의 오직 특징적인 증상의 일부만을 포함하고 있을 뿐이며, 질환 전반에 대한 포괄적인 기술을 담보할 수는 없다. 둘째, DSM을 활용한 진단과정에서 인지적인 상호과정을 간과하고 DSM을 체크리스트 수준으로 부주의하게 사용하는 것이 빈번하다. 실제로, 앨런 프랜시스(Allen Frances)는 조작주의 진단체계를 부주의하게 오용하여 개인의 악행을 함부로 정신질환 진단으로 명명하는 것을 통렬하게 비판한 바 있다. 셋째, 신뢰도(reliability)를 담보하기 위해 타당도(validity)를 희생한 결과, 정신의학 연구에서 DSM의 유용성이 제한적인 수준에 머물고 있다. 그리고 조현병 등 정신질환을 이해하기 위해서 DSM 진단기준을 암기하기보다는 무엇보다도 과거 위대한 정신병리학자의 이론적 토대를 학습하는 것이 필수적이라고 주장하였다. 그 중에서도 현상학적 정신병리학이 동시대 정신의학 임상실제에서도 여전히 유효한 것이라고 설명하였다[50].
현상학적 정신병리학(phenomenological psychopathology)은 비정상에 대한 상식적, 사회정치적, 및 과학적 견해를 괄호 안에 넣고 체험적 변화 및 차이의 다양성을 기술하는 것을 목적으로 하는 방법론이다. 현상학적 정신병리학은 외견적으로 비합리적이거나 부조리한 현상 속에서 인간이란 무엇인가를 파악하려고 한다. 따라서, 현상학적 정신병리학은 환자중심의 태도를 견지하고 있기에 조작주의 진단구조의 제한점이 상존하는 임상실제에서 여전히 유효한 것이라고 할 수 있다. 현상학적 정신병리학은 정신병리학과 현상학적 철학 간 교류의 첫 번째 이정표에 해당한다. 정신병리학에 영향을 끼친 현상학적 개념은 간주관성(intersubjectivity)과 지향성(intentionality)이다. 간주관성은 객관적인 세계상의 성립을 위한 개념으로서, 세계의 존재에 대한 감각이 자신에게 존재하듯이 타인에게도 동시에 존재한다는 것을 이해한다는 것을 의미한다. 지향성은 심리적인 현상은 그 자체에 대상을 지향하고 있음을 의미하며 환청의 체험은 타자에 대한 지향성으로 정립할 수 있다. 현상이라 함은 어떤 객관적인 사물을 가리키지 않으며 어떤 의식에 의해 체험되는 대상이 나타나는 구체적인 모습을 지시한다[51-56].
정신병리학자이자 실존철학자인 카를 야스퍼스(Karl Jaspers)는 그의 저서 ‘정신병리학 총론(Allegemeine Psychopathologie)’에서 에드문트 훗설(Edmund Husserl)의 현상학과 빌헬름 딜타이(Wilhelm Dilthey)의 이해심리학을 정신병리학의 방법론으로 수용함으로써 환자의 전체상과 주관적인 체험에 대한 이해를 정신병리학 내에 도입하였다. 이를 통해 현상학적 정신병리학을 정립하였다. 야스퍼스는 정신질환을 발달(development)과 과정(process)으로 구분하였는데, (성격장애의) 발달은 감정이입을 통해 의미, 동기 및 목적의 이해의 연장선에서 추적할 수 있는 것을 의미하는 반면에 (정신병의) 과정은 정신적인 행동에 대한 이해의 일관성을 상실한 것을 의미한다. 야스퍼스는 감정이입을 통한 소통의 손상을 조현병의 근본적인 결핍으로 간주하였으며, 개인적인 체험의 ‘궁극적으로 이해될 수 없음(ultimately un-understandability)’을 조현병의 특징적인 속성으로 보았다[57-60]. 그리고 야스퍼스의 조현병에 대한 현상학적 관점은 전술한 슈나이더의 일급증상으로 계승되었다. 2010년 대한조현병학회는 schizophrenia의 한글용어를 ‘정신분열병’에서 ‘조현병’으로 개정할 때, 휴정의 ‘선가귀감’ 중 다음 문구로부터 착안하였다. “공부는 거문고 줄 고르는 법(調絃之法)과 같아서 팽팽함과 느슨함이 알맞아야 한다. 너무 애쓰면 집착하기 쉽고, 잊어버리면 무명에 떨어질 것이니.” 즉, 조현지법(調絃之法)을 통해, 신경영상학 연구결과를 토대로 조현병에서 신경회로가 부적합하게 조율되어 있는 질병상태를 은유적으로 표현한 것이었다[61,62]. 그리고 조현병의 영문표기인 ‘attunement disorder’는 상식의 소실 상태에서 간주관성 세계에 편입하기 곤란한 상태를 반영한 것이었다[63]. 따라서 DSM 진단구조 속에서 주관적이고 개인적인 체험으로서의 조현병에 대한 인식의 중요성이 점진적으로 잊혀 가는 상황 속에서[64], 그래도 조현병의 영문명칭인 attunement disorder가 그 현상학적 전체상을 반영하고 있는 것은 그 의의가 적지 않다.
환자의 외부세계에 대한 전체적인 관계는 가장 포괄적인 방식에서 영향을 받는다. 모든 이러한 장애에 대한 지식은 개인과 인류 모두에서 정신적 삶에서 보편적인 법칙의 많은 부분을 드러낼 뿐만 아니라 인간 마음에 대한 심도 있는 통찰을 제공할 수 있으므로 정신적 삶에 대한 연구에서 가장 효과적인 분야이다. 그것은 사회적 삶의 수많은 지적, 도덕적, 종교적, 및 예술적 경향과 현상을 이해할 수 있는 적절한 척도를 제공한다. 그러나 그것은 임상가에게 필수적인 정신적 장애를 이해할 수 있게 하는 인간존재에 대한 가장 중요한 질문에 대해 다양한 과학적 관계를 제시하며, 그 임상적 실용성이 뛰어나다. 정신질환은 그것이 심지어 가장 경미한 형태일지라도 임상가가 직면해야하는 가장 큰 고통을 수반한다.
이 글은 남긴 연구자는 현상학적 정신병리학자가 아니라, 바로 범주적 진단단위를 지향했던 에밀 크레펠린이었다[31]. 그는 정신의학이 의학의 한 분과임에 대한 신념을 토대로, 그 분과가 지닌 특수성을 생생하게 포착하여 전달하고자 하였다[65]. 즉, 임상실제에서 현상학적 정신병리학의 의의가 어느 정도인지를 반영하는 글이라고 하겠다.
결론
1980년대 실증주의 및 의과학 태도의 영향 아래에서 DSM-III가 공표된 이후로, DSM 진단구조는 줄곧 개념을 이에 대응하는 조작들의 집합과 동의어로 상정하는 조작주의를 통해 정의되었다. DSM 내의 조현병이라는 진단단위는 자연적 표현형이라기보다는 인지적 구성체에 해당한다. 현재의 조현병 진단구성은 에밀 크레펠린의 만성화, 쿠르트 슈나이더의 양성증상, 오이겐 블로일러의 음성증상을 적절하게 합쳐낸 결과물로서 평가되기도 한다. DSM-5과 DSM-5-TR의 조현병 진단기준에서의 개정사항은 슈나이더의 일급증상에 대한 진단적 가중치 조항과 편집형, 와해형, 긴장형, 미분화형, 잔류형 등 유형에 대한 조항을 모두 삭제하는 것이었다. 그 결과, 그간 조현병의 질병 특이적 증상으로 간주되었던 형식적 사고장애의 개념이 진단구조 내에서 점진적으로 잊히게 되었고, 조현병이라는 범주는 만성적인 망상-환각 증후군으로 상대적으로 협소화되었다고 비판을 받았다. 증상중심 조현병 진단단위는 질병 본질주의 모형과 부합하지 않으므로, 동일 진단 내에서도 이질성을 내포하여, 연구도구로서 제한점을 있다고 볼 수 있다. 카를 야스퍼스는 감정이입을 통한 소통의 손상이나 궁극적으로 이해될 수 없음 등을 조현병의 근본적인 결핍으로 간주하였는데, 현상학적 전체상의 의의도 잊혀 가는 경향이 있다. 따라서, 현상학적 정신병리학은 개인의 주관적이고 개인적인 체험의 변화를 파악하는 방법론으로서 여전히 유효하다고 하겠다.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
References
Peer Reviewers’ Commentary
이 논문은 조현병의 진단 기준과 체계가 정신병리학적 측면에서 변화되어 온 과정과 현재의 DSM 진단 체계가 가지고 있는 특징과 한계를 정리한 논문이다. DSM-III 진단 체계에서 조현병의 진단 기준으로 환청, 망상, 사고장애 등 관찰이 가능한 개념들을 진단에 필요한 증상으로 삼았다. 이러한 조작주의적 진단 기준은 진단의 신뢰도와 특이도를 높이기 위하여 도입되었지만, 사고, 언어, 개념형성의 이상을 조현병의 근본 증상으로 보는 형식적 사고장애의 개념이 간소화되고 환청과 망상의 진단적 의미가 지나치게 부각된 측면이 있음을 잘 설명하고 있다. 이 논문에서는 조현병의 본질에 대한 이해 노력과 질병의 현상학적 의미 파악도 중요함을 잘 지적하고 있다. 이 논문은 조현병 환자를 진료하는 임상 현장에서 조현병 환자를 진단하는 데 많은 도움이 될 것으로 판단된다.
[정리: 편집위원회]