Change of culprit agent prevents recurrent hypersensitivity reactions to iodinated contrast media
Article information
Abstract
Abstract
With technical advances in computed tomography and the introduction of non-ionic low- or iso-osmolar iodinated contrast media (ICM), the use of ICM and the occurrence of ICM-related hypersensitivity reactions (HSRs) has rapidly increased. Although ICM-related HSRs are known to be mild, they still represent life-threatening events in rare instances. It is therefore important to prevent recurrent HSRs in high-risk patients. Changing the culprit contrast agent is a powerful known tool for reducing the recurrence rate of HSRs. Based on the large body of evidence, the American College of Radiology manual on contrast media (latest version 10.3) suggests that changing the ICM within the same class may help reduce the likelihood of a subsequent contrast reaction. Furthermore, the European Society of Urogenital Radiology guidelines on contrast agents (latest version 10) also recommends using a different contrast agent with previous contrast agent reactors to reduce the risk of an acute reaction. In this article, we review the necessity and clinical efficacy of changing the culprit ICM for high-risk patients at the time of re-exposure to prevent ICM-related HSRs and minimize the risk of fatality.
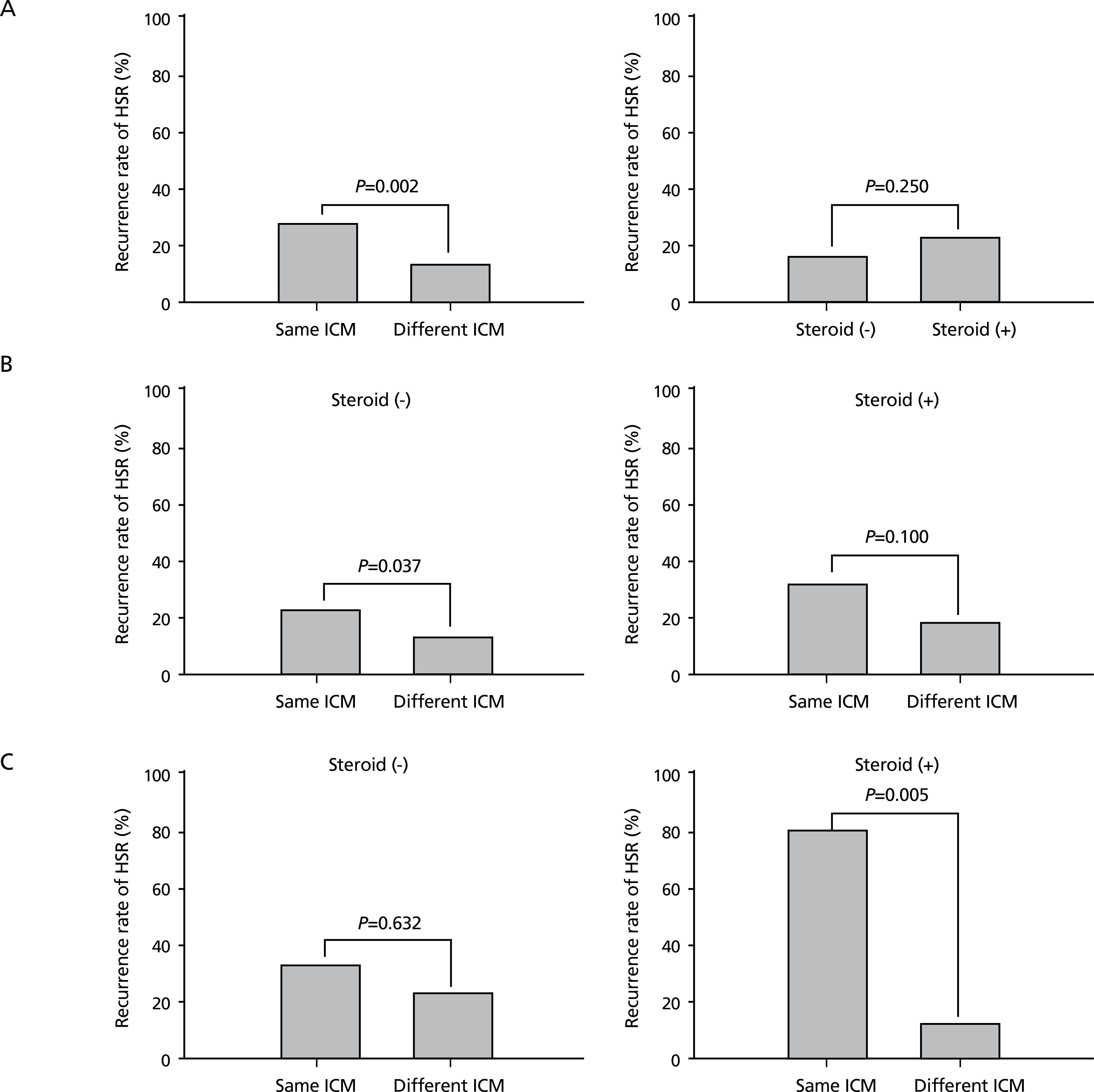
Recurrence rates of hypersensitivity reactions (HSRs) according to iodinated contrast medium (ICM) changes and steroid premedication in the total patients (A), in patients with a moderate initial HSR (B). and in patients with a severe initial HSR (C). Reproduced from Park HJ et al. Eur Radiol 2017;27:2886-2893, with permission from Springer Nature [11].

Recurrence rates of iodinated contrast media-related hypersensitivity reaction according to the combination of contrast media in absence of premedication