서론
비타민 K 길항제와 heparin에 의한 항응고 요법이 시작된 지 50여 년이 지났으나 아직까지 항응고 요법에 사용되는 가장 중요한 약제는 비타민 K 길항제인 warfarin이다. Warfarin은 본 리뷰에서 소개하고자 하는 약제들이 나오기 전까지는 장기간 투여가 인정된 거의 유일한 경구용 항응고제였다. 하지만 여러 가지 제한점으로 인해 처방하는 의사와 warfarin을 투여 받는 환자 모두 불편함을 감수하여야 했다.
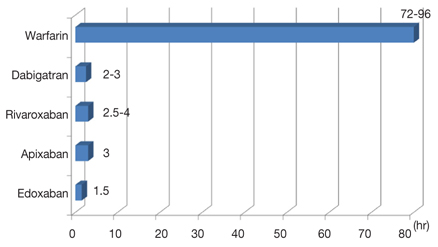
Warfarin은 작용이 나타날 때까지 걸리는 시간이 길다(Figure 1). 따라서 빠른 시간 내에 항응고 효과를 보는 것이 필요한 환자는 heparin과 같은 약제를 교가요법(bridging therapy)으로 사용해야 한다. 또한 반감기가 길어 수술 또는 시술 전에 수일간 복용을 중지하고 프로트롬빈 시간(prothrombin time)이 낮아졌는지 측정해봐야 하는 불편이 있다.
Warfarin은 cytochrome P450 (CYP) 2C9에 의해 부분적으로 대사되는데, amiodarone이 대표적인 억제자이다. 이 두 약제는 같이 처방되는 경우가 흔하므로 warfarin 용량 조절에 주의가 필요하다. 또한 약물대사와 관련된 유전자 다형성에 영향을 받는다. 약물대사와 관련된 CYP2C9과 비타민 K 대사와 관련된 VKORC1 유전자의 다형성이 존재하며 이에 따라 요구되는 개인별 warfarin 용량이 차이가 난다[1,2,3]. 게다가 치료 효과가 나타나는 영역이 좁아 잦은 모니터링이 필요하다. Warfarin은 또한 다양한 식품들이 그 대사나 작용에 영향을 미치므로 주의를 요한다[4]. 새로운 경구용 항응고제(new oral anticoagulant, NOAC)는 이와 같은 불편함을 해소하는 방향으로 개발되고 있다.
새로운 경구용 항응고제
1. 약리학적인 특성
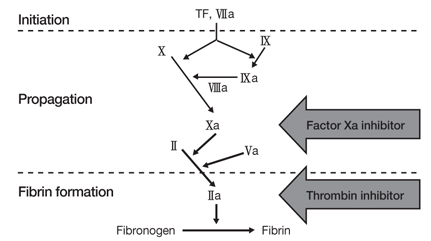
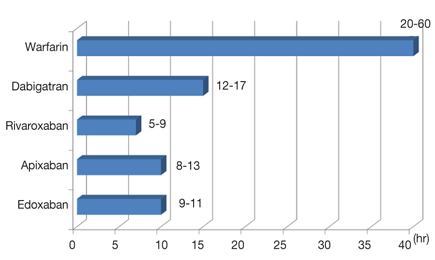
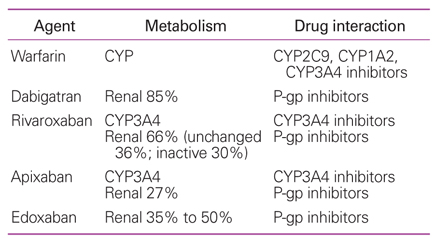
2012년 현재 대규모 임상시험을 마친 NOAC으로는 dabigatran, rivaroxaban, apixaban 등이 있다. Dabigatran은 직접적인 thrombin 억제제이며, 활성화된 인자 X(Xa)를 억제(ban)하는 약제들이 xaban으로 불리는 약제들이다(Figure 2). 이들은 Figure 1과 같이 작용이 나타날 때까지 걸리는 시간이 짧고, 또한 반감기가 짧다[5,6,7] (Figure 3). Warfarin은 모두 간에서 cytochrome P450계에 의해 대사되는 반면 NOAC은 일부가 신장으로 배설된다(Table 1). 따라서 약제의 용량을 결정하는 데에 신기능을 고려해야 한다. 또한 NOAC들도 약제간 상호작용이 있다. 투여된 약제의 일부가 CYP3A4 또는 P-당단백 등에 의해 대사되므로 이들을 억제하는 약제에 영향을 받게 된다. 특히 ketoconazole은 NOAC의 약효를 약 160% 증가시킬 수 있어 병용금기 약물이다[8].
2. 임상시험 결과분석
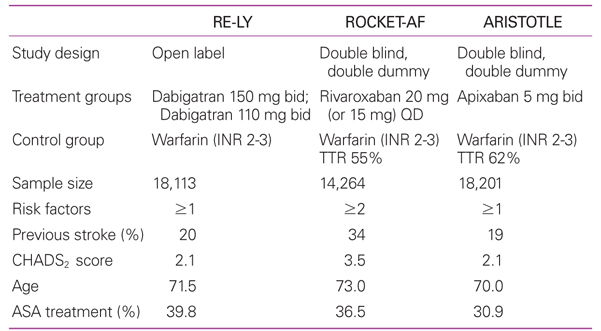
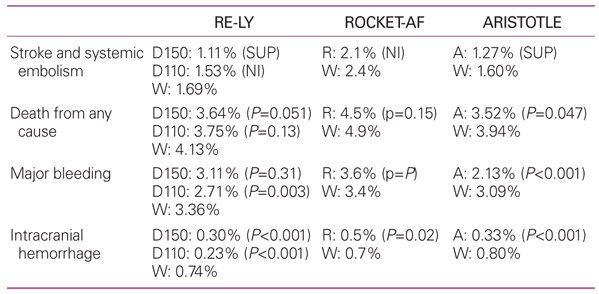
Dabigatran, rivaroxaban, apixaban의 효과와 안전성을 warfarin과 비교한 주요 대규모 임상시험은 각각 RE-LY [9], ROCKET-AF [10], ARISTOTLE [11] 연구이다. 모두 비판막성 심방세동 환자들을 대상으로 한 연구들이며, Table 2에서 보는 바와 같이 ROCKET-AF 연구에 모집된 환자들의 CHADS2 (cardiac failure, hypertension, age, diabetes, stroke)점수는 3.5점으로 다른 연구에 모집된 환자들(2.1점)보다 뇌졸중의 위험도가 높았다. Warfarin에 비해 혈전색전증의 예방효과는 열등하지 않거나 우월했으며, 주요 출혈 발생률이 낮았고 특히 두개 내 출혈 발생은 모든 NOAC군이 warfarin군에 비해 유의하게 낮았다(Table 3).
3. 심방세동 치료 가이드라인에서의 새로운 경구용 항응고제
북미와 유럽의 심장학회 가이드라인은 비판막성 심장질환자에서 심방세동이 있을 경우 항응고 요법의 대상이 되는 환자들은 warfarin과 함께 NOAC을 사용할 수 있다고 권고하고 있다[12,13]. 어떤 항응고제를 사용할 지는 환자의 선호도, 위험도, 약제의 가격, 과거 warfarin 치료 중의 안정성 등을 고려하여 결정한다. 유럽 학회에서는 NOAC을 warfarin보다 우선해서 사용하는 것에 대한 경우도 권고강도 IIa, 증거수준 B로 권하고 있다[13]. 동리듬 전환을 위한 항응고 요법으로 warfarin외에 dabigatran을 사용할 수도 있다[13].
4. 신기능에 따른 용량
전술한 바와 같이 NOAC은 신대사의 과정도 거치기 때문에 처방하기 전에 환자의 신기능을 평가해야 한다. 대한민국 식약청의 허가사항은 다음과 같다. Dabigatran의 경우 creatinine 청소율이 30 mL/min 미만인 경우 금기이다. 청소율이 30-49 mL/min일 경우 1일 2회, 110 mg/회를 권한다. Rivaroxaban의 경우 creatinine 청소율이 15 mL/min 미만인 경우 금기이고, 청소율이 15-49 mL/min일 경우 1일 1회, 15 mg/회를 권한다. 반면 유럽 학회의 가이드라인은 creatinine 청소율이 30 mL/min 미만이면 모든 NOAC 은 금기라고 권고하고 있다[13].
결론
NOAC은 대규모 임상시험들을 통해 기존 치료 약물인 warfarin에 비해 효율은 떨어지지 않으면서 출혈 부작용은 감소시키는 결과를 보였다. 적어도 비판막성 심방세동 환자들의 항응고 요법에서 상당 부분 기존 약물을 대치시킬 것으로 예상된다. 많은 장점을 가진 약물이지만 말기 신장 질환자에는 투여가 금기이며, 환자가 복용을 제대로 하고 있는지를 평가할 수 있는 모니터링 방법이 미흡하고, 급하게 약제의 효과를 반전시켜야 할 순간에 적절한 해독제가 없다는 점 등이 단점이다. 향후 이들을 보완할 수 있는 방법의 개발과 함께, 판막질환을 가진 심방세동 환자, 도자 절제술을 받는 환자 등으로의 적응증 확대도 가능한지 임상시험을 통해 확인되어야 할 것이다.
Peer Reviewers' Commentary
본 논문은 최근 개발된 항응고제에 대한 리뷰 논문이다. 기존에 수 십년간 뇌졸중 및 혈전증 예방을 위하여 사용되었던 비타민 K 길항제(와파린)는 그 탁월한 효과에도 불구하고 타 약물과의 작용, 잦은 혈액 측정을 통한 응고 수치 확인 등의 문제점으로 필요한 환자의 50% 이하에서만 처방되고 있는 실정이다. 최근에 개발된 새로운 경구용 항응고제(new oral anticoagulat, NOAC)인 dabigatran, rivaroxaban, apixaban 등은 이러한 문제점을 상당 부분 개선하였으며, 뇌졸중 예방효과도 또한 비판막성 심방세동에서 탁월하다. 본 논문은 최근 와파린의 대체약으로 출시된 여러 가지 새로운 항응고제의 장점과 사용시 주의사항, 각 약제들의 비교점을 정리하여 임상에서 유용한 정보를 제공한다. 이미 구미 선진국에서는 임상에 사용되고 있으며, 국내에서도 제한적으로 금년부터 보험이 적용되므로 많은 환자들이 혜택을 받을 것으로 생각된다. 따라서 실제 약을 처방하는 의사들의 교육 자료가 절실한 실정에서 본 리뷰 논문은 시기 적절하다고 할 수 있다.
[정리: 편집위원회]