






 |
 |
| J Korean Med Assoc > Volume 55(11); 2012 > Article |
Abstract
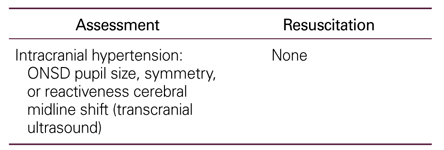
Bedside ultrasonographic examination is known to be a quick, noninvasive, cost-effective, repeatable, and harmless diagnostic modality. It can be a powerful tool for clinicians, especially in time-dependent situations including trauma. Focused assessment with sonography in trauma (FAST) has been established as a protocol especially specifically for hemodynamically unstable patients with blunt abdominal trauma. The physiologic priority of airway, breathing, circulation, and disability (ABCD) of injured patients should be assessed using a multi-systemic, multi-focused, problem-based, and point-of-care ultrasound as an extension of physical examination. This ultrasound-enhanced trauma life support, so called FAST-ABCD, can provide a great deal of important information for helping the primary physician in critical decision-making by systemically combining the airway, lung, cardiovascular, abdominopelvic, orbital, and transcranial ultrasound. Additionally, it can provide information on airway patency, guidance of endotracheal intubation and cricothyroidotomy, lung contusion, limited hemodynamics, differential diagnosis of shock, intracranial hypertension, and even more extensively on a secondary survey from head to toe. The indications for the utility of ultrasound in trauma continue to evolve beyond FAST. FAST-ABCD could be incorporated into advanced trauma life support by obtaining more evidence through more studies worldwide.
Acknowledgement
I would like to express my gratitude to all those who gave me the opportunity to complete this review. I want to thank Luca Neri, the former president of World Interactive Network of Focused Critical Ultrasound (WINFOCUS), Gordon Lee, and Hanho Doh for providing me valuable clinical data.
References
1. Neal MD, Peitzman AB, Forsythe RM, Marshall GT, Rosengart MR, Alarcon LH, Billiar TR, Sperry JL. Over reliance on computed tomography imaging in patients with severe abdominal injury: is the delay worth the risk? J Trauma 2011;70:278-284.
2. Rozycki GS, Ochsner MG, Schmidt JA, Frankel HL, Davis TP, Wang D, Champion HR. A prospective study of surgeon-performed ultrasound as the primary adjuvant modality for injured patient assessment. J Trauma 1995;39:492-498.
3. Kirkpatrick AW, Sirois M, Laupland KB, Liu D, Rowan K, Ball CG, Hameed SM, Brown R, Simons R, Dulchavsky SA, Hamiilton DR, Nicolaou S. Hand-held thoracic sonography for detecting post-traumatic pneumothoraces: the Extended Focused Assessment with Sonography for Trauma (EFAST). J Trauma 2004;57:288-295.
4. Dulchavsky SA, Henry SE, Moed BR, Diebel LN, Marshburn T, Hamilton DR, Logan J, Kirkpatrick AW, Williams DR. Advanced ultrasonic diagnosis of extremity trauma: the FASTER examination. J Trauma 2002;53:28-32.
5. Neri L, Storti E, Lichtenstein D. Toward an ultrasound curriculum for critical care medicine. Crit Care Med 2007;35:5 Suppl. S290-S304.
6. Gruen RL, Jurkovich GJ, McIntyre LK, Foy HM, Maier RV. Patterns of errors contributing to trauma mortality: lessons learned from 2,594 deaths. Ann Surg 2006;244:371-380.
7. Elliott DS, Baker PA, Scott MR, Birch CW, Thompson JM. Accuracy of surface landmark identification for cannula cricothyroidotomy. Anaesthesia 2010;65:889-894.
8. Walls RM, Murphy MF. Manual of emergency airway management 2008;3rd ed. Philadelphia: Lippincott Williams & Wilkins.
9. Gerig HJ, Schnider T, Heidegger T. Prophylactic percutaneous transtracheal catheterisation in the management of patients with anticipated difficult airways: a case series. Anaesthesia 2005;60:801-805.
10. Lichtenstein D, Meziere G, Biderman P, Gepner A, Barre O. The comet-tail artifact: an ultrasound sign of alveolar-interstitial syndrome. Am J Respir Crit Care Med 1997;156:1640-1646.
11. Wilkerson RG, Stone MB. Sensitivity of bedside ultrasound and supine anteroposterior chest radiographs for the identification of pneumothorax after blunt trauma. Acad Emerg Med 2010;17:11-17.
12. Ball CG, Kirkpatrick AW, Feliciano DV. The occult pneumothorax: what have we learned? Can J Surg 2009;52:E173-E179.
13. Ball CG, Ranson K, Dente CJ, Feliciano DV, Laupland KB, Dyer D, Inaba K, Trottier V, Datta I, Kirkpatrick AW. Clinical predictors of occult pneumothoraces in severely injured blunt polytrauma patients: a prospective observational study. Injury 2009;40:44-47.
14. Enderson BL, Abdalla R, Frame SB, Casey MT, Gould H, Maull KI. Tube thoracostomy for occult pneumothorax: a prospective randomized study of its use. J Trauma 1993;35:726-729.
15. Mennicke M, Gulati K, Oliva I, Goldflam K, Skali H, Ledbetter S, Platz E. Anatomical distribution of traumatic pneumothoraces on chest computed tomography: implications for ultrasound screening in the ED. Am J Emerg Med 2012;30:1025-1031.
16. Lichtenstein D, Meziere G, Biderman P, Gepner A. The comettail artifact: an ultrasound sign ruling out pneumothorax. Intensive Care Med 1999;25:383-388.
17. Lichtenstein D, Meziere G, Biderman P, Gepner A. The "lung point": an ultrasound sign specific to pneumothorax. Intensive Care Med 2000;26:1434-1440.
18. Volpicelli G, Elbarbary M, Blaivas M, Lichtenstein DA, Mathis G, Kirkpatrick AW, Melniker L, Gargani L, Noble VE, Via G, Dean A, Tsung JW, Soldati G, Copetti R, Bouhemad B, Reissig A, Agricola E, Rouby JJ, Arbelot C, Liteplo A, Sargsyan A, Silva F, Hoppmann R, Breitkreutz R, Seibel A, Neri L, Storti E, Petrovic T. International Liaison Committee on Lung Ultrasound (ILC-LUS) for International Consensus Conference on Lung Ultrasound (ICC-LUS). International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med 2012;38:577-591.
19. Sisley AC, Rozycki GS, Ballard RB, Namias N, Salomone JP, Feliciano DV. Rapid detection of traumatic effusion using surgeon-performed ultrasonography. J Trauma 1998;44:291-296.
20. Lichtenstein D, Hulot JS, Rabiller A, Tostivint I, Meziere G. Feasibility and safety of ultrasound-aided thoracentesis in mechanically ventilated patients. Intensive Care Med 1999;25:955-958.
21. Soldati G, Testa A, Silva FR, Carbone L, Portale G, Silveri NG. Chest ultrasonography in lung contusion. Chest 2006;130:533-538.
22. Rocco M, Carbone I, Morelli A, Bertoletti L, Rossi S, Vitale M, Montini L, Passariello R, Pietropaoli P. Diagnostic accuracy of bedside ultrasonography in the ICU: feasibility of detecting pulmonary effusion and lung contusion in patients on respiratory support after severe blunt thoracic trauma. Acta Anaesthesiol Scand 2008;52:776-784.
23. Gunst M, Ghaemmaghami V, Sperry J, Robinson M, O'Keeffe T, Friese R, Frankel H. Accuracy of cardiac function and volume status estimates using the bedside echocardiographic assessment in trauma/critical care. J Trauma 2008;65:509-516.
24. Ferrada P, Murthi S, Anand RJ, Bochicchio GV, Scalea T. Transthoracic focused rapid echocardiographic examination: real-time evaluation of fluid status in critically ill trauma patients. J Trauma 2011;70:56-62.
25. Carr BG, Dean AJ, Everett WW, Ku BS, Mark DG, Okusanya O, Horan AD, Gracias VH. Intensivist bedside ultrasound (INBU) for volume assessment in the intensive care unit: a pilot study. J Trauma 2007;63:495-500.
26. Ma OJ, Mateer JR, Ogata M, Kefer MP, Wittmann D, Aprahamian C. Prospective analysis of a rapid trauma ultrasound examination performed by emergency physicians. J Trauma 1995;38:879-885.
27. Natarajan B, Gupta PK, Cemaj S, Sorensen M, Hatzoudis GI, Forse RA. FAST scan: is it worth doing in hemodynamically stable blunt trauma patients? Surgery 2010;148:695-700.
28. Udobi KF, Rodriguez A, Chiu WC, Scalea TM. Role of ultrasonography in penetrating abdominal trauma: a prospective clinical study. J Trauma 2001;50:475-479.
29. Rozycki GS, Feliciano DV, Ochsner MG, Knudson MM, Hoyt DB, Davis F, Hammerman D, Figueredo V, Harviel JD, Han DC, Schmidt JA. The role of ultrasound in patients with possible penetrating cardiac wounds: a prospective multicenter study. J Trauma 1999;46:543-551.
30. Rajajee V, Vanaman M, Fletcher JJ, Jacobs TL. Optic nerve ultrasound for the detection of raised intracranial pressure. Neurocrit Care 2011;15:506-515.
Figure 1
Focused assessment with sonography in trauma including airway, breathing, circulation, and disablity (FAST-ABCD). Numbers on a figure indicate positions where probe would be applied to get images about airway, breathing, circulation, and disability. 1. Airway (neck) ultrasound (A). 2. Lung ultrasound (B). 3. Cardiovascular ultrasound (C). 4. Focused assessment with sonography in trauma (C). 5. Orbital and transcranial ultrasound (D).
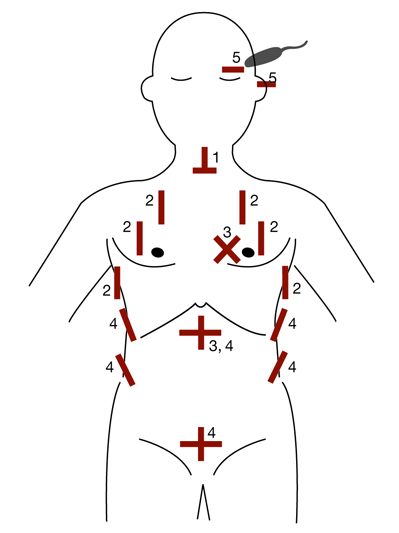
Figure 3
Cricoid cartilage, transverse scan. Cricoid cartilage (arrows). Transverse scan. The tissue-air border is shown as white line (arrow head).
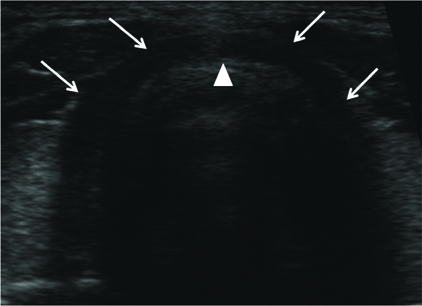
Figure 4
Cricothyroid membrane. (A) Upper airway scanned in the midsagittal plane. (B) From the right side, thyroid cartilage (T), cricoid cartilage (C), and tracheal rings (TR). Cricothyroid membrane (arrow). The tissue-air border (arrow head).

Figure 5
Esophageal intubation. Transverse scan just cranial to the suprasternal notch. Enlarged esophagus by tube is shown on the deep left side of trachea (arrow head) in real time (arrow).

Figure 6
Lung pulse. (A) Left lung sliding is abolished in this selectively intubated patient and vertical movement of pleural line is identified along to the cardiac pulsation on a real-time 2D image, but it cannot be objectified on this static image. (B) M-mode can record vibrations in rhythm with the cardiac activity (arrows).
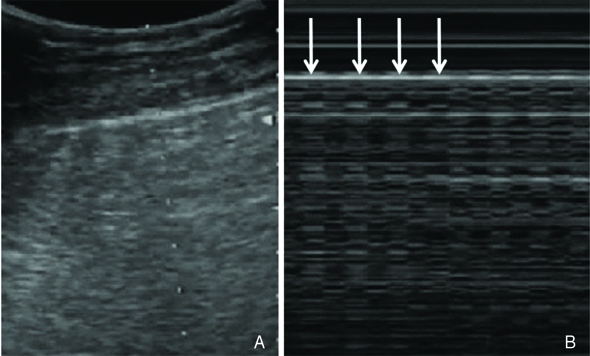
Figure 7
Longitudinal scan on thorax of a normal subject. (A) Upper and lower ribs and their acoustic shadows (vertical arrows). Pleural line and it's reverberation artifacts, Alines (horizontal arrows). (B) The upper rib-pleural line-lower rib profile shapes a sort of bat flying toward you, bat sign which is the basic landmark in lung ultrasound.

Figure 8
Seashore sign on M-mode. (A) This static image can not show lung sliding, which can be identified in real time. A-lines (horizontal arrows) (B) This M-mode image shows a double component pattern separated by the pleural line (vertical arrows). The top looks waves, and the bottom looks sand. It recalls the beach, hence the seashore sign.

Figure 9
Multiple B-lines (lung rockets). Vertical lines arising from pleural line are shown. They are comet tails with well-defined, laser-like lines spreading up to the edge of the screen without fading. These artifacts are caused by thickened interlobular septum.

Figure 10
Pneumothorax: A-line sign and stratosphere sign. (A) The absence of lung sliding cannot be visualized in this static image, but horizontal artifacts arising from the pleural line can be seen, and no B line is visible. This pattern called the A-line sign. (B) M-mode can show a pattern of completely horizontal lines, which means no motion of the structures above and below the pleural line (vertical arrow). This M-mode pattern called the stratosphere sign.
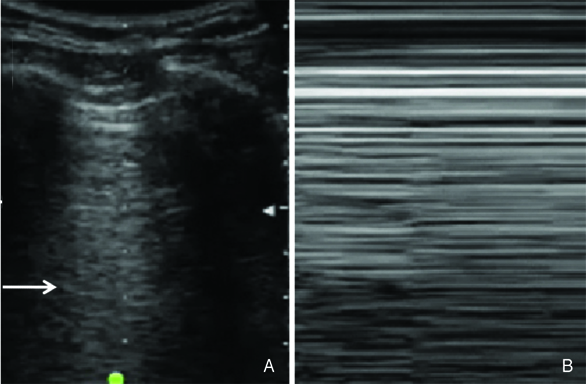
Figure 11
Pneumothorax: lung point. In real time, a transient inspiratory movement is visible at the pleural line. Arrows indicate the border between lung and air (pneumothorax), which is moving. This is the lung point sign. + LS, presence of lung sliding; - LS, absence of lung sliding.

Figure 12
Hemothorax. Hemothorax (H) can have internal echo. Consolidated lung (C) caused by compressive atelectasis is visualized. Bright echogenic spots in the consolidated lung are the airbrochogram (arrows).

Figure 13
Pleural effusion: sinusoid sign. (A) Small pleural effusion is visible at a middle axillary line (arrow). (B) The thickness of effusion varies in rhythm with the respiratory cycle. Deep border, a visceral pleura (arrow) moves toward the chest wall, thus shaping sinusoid.

Figure 14
Lung contusion (LC): consolidation. Image scanned sagittally on the left side (probe was positioned on a little bit higher than usual region of focused assessment with sonography in trauma in left upper quadrant). Hypoechoic lesion for alveolar consolidation (socalled hepatization) whose dimensions remained unchanged during the inspiration phase (LC). Blood within the thorax (horizontal arrows). Diaphragm (vertical arrow). H, hematoma; S, spleen; St, stomach gas. Courtesy of Dr. Gordon Lee.
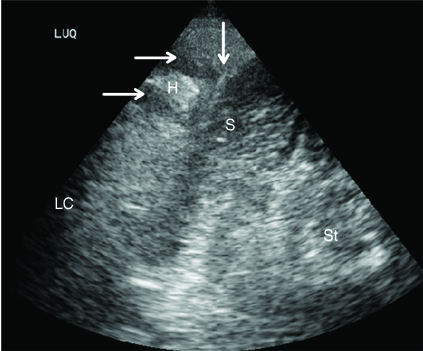
Figure 15
Lung contusion: B-lines. Lung contusion can be visualized as B-lines. Within 1 to 2 hours after primary injury, A progressive infiltrate into interstitial space cause thickened interlobular septum. Focal B-lines are shown in the upper intercostal space (arrows), but no B-line is visible in the lower intercostal space.
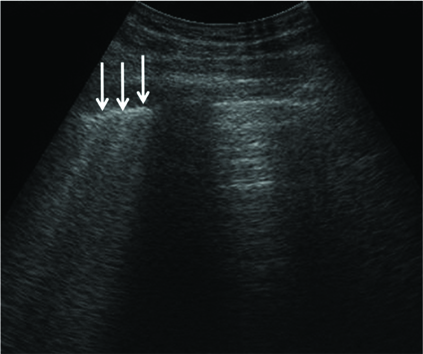
Figure 16
Flattened inferior vena cava (IVC). Subcostal longitudinal view in hemorrhagic shock. Flattened IVC is demonstrated (arrows). Additionally small and hyperkinetic ventricles can be identified on cardiac ultrasound.

Figure 17
Cardiac tamponade. Subcostal 4 chamber view in the hypotensive patient. Echogenic pericardial effusion (E) compressing the right ventricle is visible (arrow).

Figure 18
Focused assessment with sonography for trauma: hemoperitoneum. (A) Peritoneal effusion in Morison's pouch. (B) Peritoneal effusion in Douglas pouch. (C) Peritoneal effusion in subdiaphragmatic and splenorenal recess.

Figure 19
Measurement of optic nerve sheath diameter (ONSD). The optic nerve sheath is a linear hypoechoic structure posterior to the globe. Caliper 1 identifies the site of ONSD measurement 0.3 cm behind the retina. Caliper 2 measures the ONSD (0.3 cm in this case).
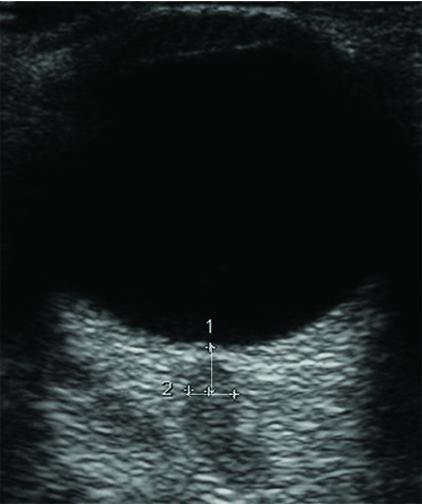
Table 1
Ultrasound-enhanced airway assessment and resuscitation of the trauma patient: airway ultrasound
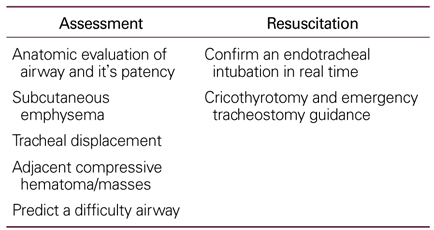
Table 2
Ultrasound-enhanced breathing assessment and resuscitation of the trauma patient: lung ultrasound

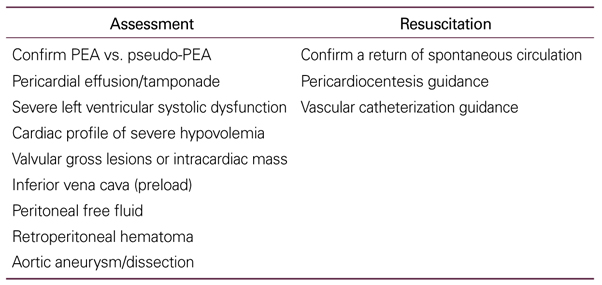
Table 3
Ultrasound-enhanced circulation assessment and resuscitation of the trauma patient: cardiovascular ultrasound
- TOOLS
-
- Share :
-





-
METRICS

-
Related articles in
J Korean Med Assoc -
Fertility preservation for patients with cancer2022 June;65(6)
Clinical Guidelines of Treatment of Obesity in Adults2003 April;46(4)
Clinical application of oral rehydration solution2012 June;55(6)
Proposal for stabilization of regional trauma centers in Korea2016 December;59(12)
Medical rehabilitation system for patients in acute rehabilitation units2017 November;60(11)
- Editorial Office
-
37 Ichon-ro 46-gil, Yongsan-gu, Seoul
Tel: +82-2-6350-6562 Fax: +82-2-792-5208 E-mail: jkmamaster@gmail.com
Copyright © 2024 by Korean Medical Association.
