면역억제제의 작용원리에 따른 종류와 임상의 실제
Mechanisms and clinical applications of immunosuppressive medications
Article information

Trans Abstract
Immunosuppressive medications and regimens have evolved with significant advancements in the understanding of the immunologic process after solid organ transplantation. Medications can block the communication between antigen-presenting cells and T-cells, the activation and proliferation of T-cells, antibody production by plasma cells, and the activation of the complement system by antibodies. T-cell depleting antibodies and interleukin-2 receptor blockers are commonly used during induction therapy. Calcineurin inhibitors, antimetabolites, antiproliferative agents, and corticosteroids are commonly used in maintenance therapy regimens. These medications decrease the rates of rejection episodes and markedly increase the survival rates of short-term grafts. However, in terms of the survival rate of long-term grafts, there is still room for improvement. Opportunistic infections, development of cancer, metabolic diseases, and calcineurin inhibitor toxicity are hurdles in the improvement in survival rates of long-term grafts. Therefore, many efforts are being taken to overcome these hurdles, such as the development of new drugs, individualization of immunosuppression, and induction of immune tolerance.
서론
면역억제제의 발전을 토대로 장기이식의 성적은 눈부시게 발전하였다. 현재 장기이식 분야에서 사용되는 면역억제제는 매우 다양하며, 이를 이해하기 위해서는 어떠한 원리로 작용하며, 어떤 종류가 있는지, 그리고 실제 임상에서 어떻게 사용되는지를 정리해 볼 필요가 있다. 우선, 면역억제제를 작용원리에 따라 분류하기 위해서는 이식 후 일어나는 기본적인 면역반응에 대한 이해가 필요하다. 일련의 면역반응 과정에서 한 부분 또는 여러 부분을 막는 것을 목표로 면역억제제가 작용하기 때문이다.
장기이식 후 면역반응
동종의 고형장기가 체내에 들어오는 경우, 고형장기 내의 기증자 유래 항원제시세포와 수혜자 유래 항원제시세포가 수혜자의 림프절(lymph node)로 이동하여 기증자의 항원을 수혜자의 면역세포 T세포과 B세포에게 제시하게 된다. 가장 대표적인 항원제시세포는 수지상세포이다(Figure 1).
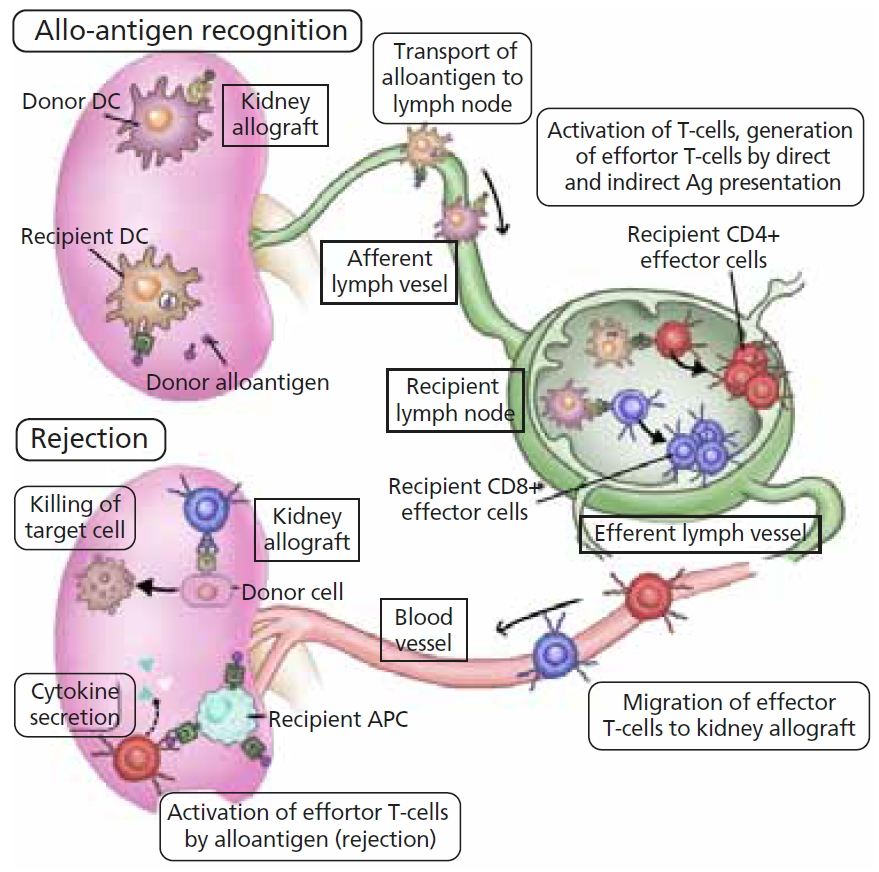
Basic scheme of immune response after solid organ transplantation. DC, dendritic cell; APC, antigen presenting cell. Illustrated by the author.
항원제시세포가 항원을 T세포에게 제시하는 과정에서 B7-CD28 경로와 같은 동시 자극 신호가 동시에 작용하여야만 T세포가 항원을 인식할 수 있다. 항원을 인식한 T세포는 interleukin 2 (IL-2)라는 사이토카인(cytokine)을 분비하여 스스로 활성화되고 주변의 T세포도 활성화시키며, 분열 및 분화하여 효과 T세포 또는 기억 T세포가 된다. 효과 CD8+ T세포는 직접적으로 항원을 가지고 있는 세포를 공격하고, 효과 CD4+ T세포는 사이토카인 분비를 통하여 다른 면역세포들을 활성화시킨다(Figure 2).
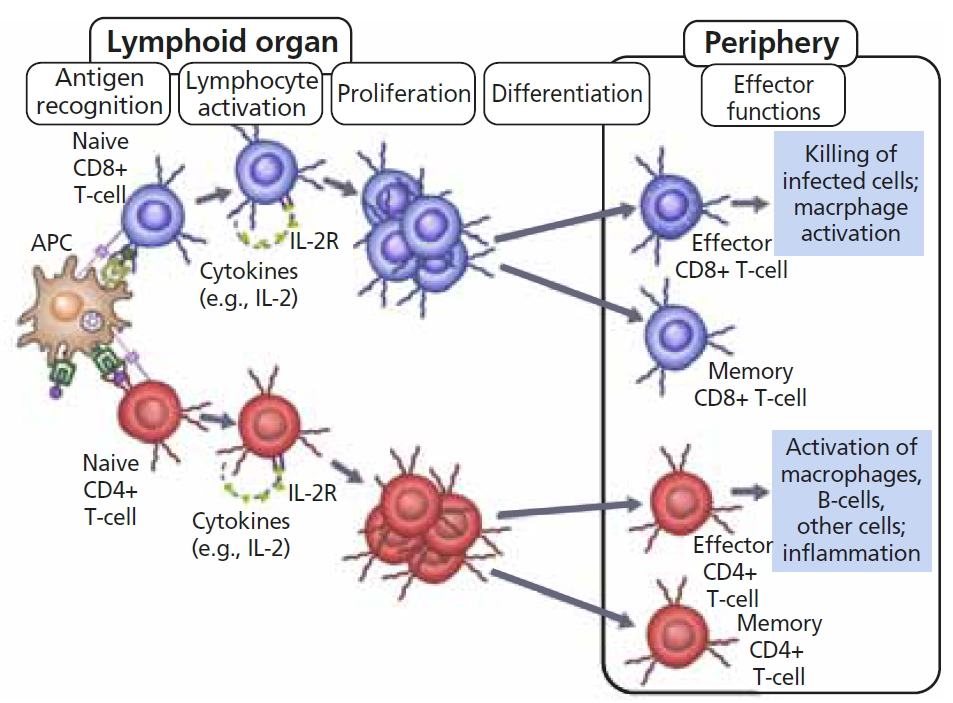
T-cell activation, proliferation, and differentiation after antigen recognition. APC, antigen presenting cell; IL-2, interleukin 2; IL-2R, interleukin 2 receptor. Illustrated by the author.
항원제시세포는 2차 림프기관의 배중심에 존재하는 B세포에도 항원을 제시하는데, 이 과정에서 효과 CD4+ T세포의 동시적인 자극이 있어야 B세포가 활성화하고 형질세포 또는 기억 B세포로 분화하게 된다. 형질세포는 항원에 특이적인 항체를 만들게 되고, 이러한 항체는 보체의 활성화, 항체 의존성 세포 매개 세포독성, 항원제시세포 활성화, 및 내피세포 활성화 등의 작용을 통하여 이식편에 면역반응을 유발한다(Figure 3).

B-cell activation and differentiation after antigen recognition. DC, dendritic cell; B, B lymphocyte; T, T lymphocyte. Illustrated by the author.
결국 활성화된 효과 CD8 T세포의 직접적인 면역반응 또는 효과 CD4 T세포로 인한 간접적인 면역반응으로 이식편에 면역반응이 일어나는 것을 T세포 매개 거부반응이라고 하고, 형질세포에서 분비된 항체에 의하여 이식편에 면역반응이 일어나는 것을 항체 매개 거부반응이라고 한다(Figure 4).

Basic scheme of rejection after solid organ transplantation. APC, antigen presenting cell; MHC, major histocompatibility complex; IFN, interferon. Illustrated by the author.
면역억제제의 종류
1. T세포 매개 거부반응 목표 면역억제제
T세포 매개 거부반응을 막기 위한 면역억제제는 위에서 설명한 일련의 면역반응 과정을 한 단계, 또는 여러 단계 차단함으로써 효능을 나타낸다. 주로는 항원제시세포가 T세포에게 항원을 인식시키는 과정, T세포가 활성화되어 IL-2를 분비하는 과정, 그리고 IL-2의 자극을 받아 분열하는 과정을 차단하게 되고 각각의 단계를 차단하는 약물은 다음과 같다(Figure 5).
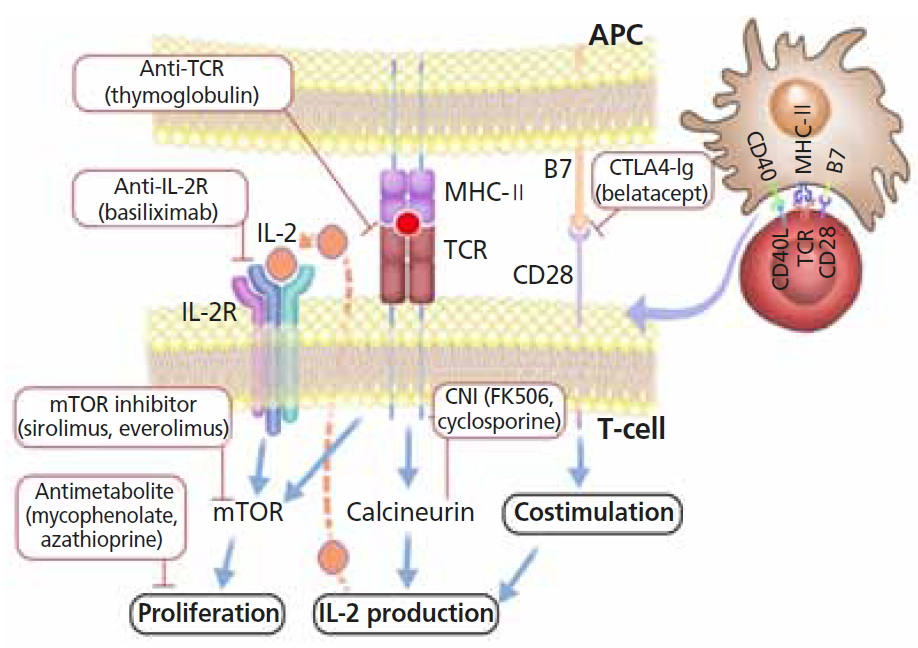
Targets of immunosuppressants in T-cell mediated rejection. TCR, T-cell receptor; IL-2, interleukin 2; IL-2R, interleukin 2 receptor; MHC, major histocompatibility complex; mTOR, mammalian target of rapamycin. Illustrated by the author.
1) 항원제시세포와 T세포의 상호작용
(1) 항흉선세포 글로불린
항흉선세포 글로불린(antithymocyte
globulin, ATG)은 사람의 흉선세포를 말이나 토끼에 접종하여 생긴 항체이다. 초기에는 말의 항체가 사용되었으나 최근에는 토끼의 항체가 사용된다. 다양한 항원에 대한 다양한 항체가 생성되기 때문에 여러가지 작용을 할 수 있지만, 주로는 ATG는 T세포의 표면에 붙어 T세포로 들어오는 자극을 차단하고, 항체 의존성 세포 매개 세포독성을 유발하여 T세포를 고갈시킨다[1].
(2) CTLA4-Ig
앞서 언급한 바와 같이 항원제시세포가 T세포에 항원을 제시할 때 B7-CD28경로를 통한 동시자극신호가 같이 전달되어야 T세포가 온전히 활성화될 수 있다. CTLA4는 T세포에서 발현하여 항원제시세포의 B7과 결합하여 T세포의 과도한 활성화를 억제하는 역할을 하는 표면항원이다. 이러한 CTLA4의 역할을 이용하기 위하여 인간의 IgG heavy chain과 CTLA4 단백질을 결합시켜 만든 약물이 CTLA4-Ig이며[2], 대표적인 약물이 belatacept이다.
2) T세포 활성화 및 IL-2 생성
3) IL-2 신호 및 T세포 분열
(1) IL-2 수용체 길항제
활성화된 T세포는 IL-2를 만드는 동시에 IL-2의 수용체를 표현하게 된다. IL-2의 자극은 세포 내로 전달되어 T세포의 분열 및 분화를 유도한다. 이러한 IL-2 수용체의 alpha chain에 결합하여 IL-2의 자극이 세포 내로 전달되는 것을 막는 약물이 IL-2 수용체 길항제이며[5], basiliximab이 대표적인 약물이다.
(2) Mammalian target of rapamycin 억제제
IL-2 수용체를 통한 자극이 세포 내로 전달되면 mammalian target of rapamycin (mTOR) 경로를 통하여 세포주기가 G1기에서 S기로 전진하게 된다. 이러한 mTOR 경로를 억제하는 약물이 mTOR 억제제이며[6], 대표적인 약물로는 sirolimus, everolimus가 있다. 이러한 mTOR 경로는 림프구뿐만 아니라 단핵구, 수지상세포, 자연살해세포, 및 내피세포 등에서도 세포주기의 전진을 억제하는 역할을 한다. 때문에 항 종양세포 효과도 가지고 있다.
(3) 항대사제
세포가 분열하기 위해서는 DNA의 합성 과정이 필수적이며, DNA의 합성을 위해서는 purine이 재료로 사용된다. Azathioprine은 이러한 purine을 대체하여 DNA의 합성을 억제하고, mycophenolate는 purine 합성에 필수적인 효소인 inosine-5′-monophosphate dehydrogenase를 억제하여 DNA 합성을 억제한다. 이렇게 DNA 합성을 억제함으로써 림프구의 분열을 억제하는 약물이 항대사제이다.
4) 여러가지 과정의 복합적인 작용
(1) 스테로이드
스테로이드는 세포 내의 glucocorticoid 수용체에 결합하여 세포핵으로의 작용이 나타나고 다양한 효과를 나타낸다. 사이토카인의 합성에 필요한 NF-κB와 activator protein-1효소를 억제하여 T세포의 분열 및 분화를 억제하게 되고, 단핵구 또는 대식세포의 세포독성작용을 억제한다[7].
2. 항체 매개 거부반응 목표 면역억제제
항체 매개 거부반응을 막기 위한 면역억제제는 B세포가 활성화되고 형질세포로 분화하여 항원 특이적인 항체를 만들고 결국 항체가 이식편에 면역반응을 일으키는 과정의 한 단계 또는 여러 단계를 차단함으로써 그 효능을 나타낸다(Figure 6).
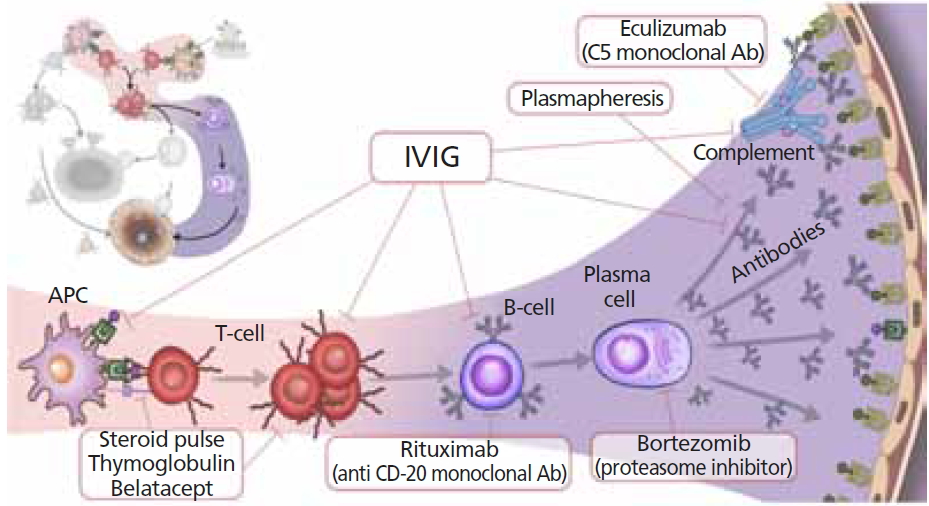
Targets of immunosuppressants in antibody mediated rejection. IVIG, intravenous immunoglobulin; APC, antigen presenting cell. Illustrated by the author.
1) T세포와 B세포 상호작용
(1) ATG
2차 림프기관의 배중심에 있는 B세포가 활성화되기 위해서는 활성화된 CD4 T세포의 도움이 필요하다. ATG는 T세포를 고갈시킴으로 해서 B세포의 활성화를 미연에 방지할 수 있다.
2) B세포 활성화
(1) 항CD20 단일 항체(Rituximab)
CD20은 성숙된 B세포의 표면에 발현되는 단백질이다. 하지만 줄기세포 단계 또는 형질세포 단계에서는 발현되지 않는다. Rituximab은 이러한 CD20에 대한 항체로 보체 의존 세포독성, 세포 성장 저해, 및 세포 자연사 유발을 포함한 여러가지 경로를 통하여 B세포를 고갈시킨다[8]. 대표적인 약물로는 rituximab이 있으며, 원래는 CD20양성 B세포 비호지킨 림프종의 치료를 위하여 개발되었고, 장기이식 분야에서는 B세포가 형질세포로 분화되는 것을 미연에 방지하기 위하여 사용된다[9].
3) 형질세포의 항체 생성
(1) Proteasome 억제제(Bortezomib)
세포로 들어오는 여러가지 종류의 신호가 DNA로 전달되어야 물질의 합성이나 세포의 분열이 일어나게 된다. 이러한 과정에서 NF-κB를 통한 유전자 조절이 필요하며 proteasome은 NF-κB를 억제하는 IκB를 분해하여 NF-κB를 활성화시키는 역할을 한다. Proteasome 억제제는 이러한 NF-κB를 통한 세포 내 신호전달을 방해하여 결국 세포 자연사를 유발하게 된다[10]. 대표적인 약물로는 bortezomib이 있으며, 원래는 형질세포가 비정상적으로 증식하는 다발성 골수종의 치료를 위하여 사용되었고, 장기이식 분야에는 형질세포의 기증자 특이 항체 생산을 억제하고 세포 자연사를 유도하기 위하여 사용된다[11].
4) 항체 제거
(1) Intravenous immunoglobulin
Intravenous immunoglobulin은 기존에 체내에 존재하는 기증자 특이 항HLA 항체 또는 항ABO 항체에 결합하여 침전시킴으로써 항체를 고갈시킨다. 결국 항체로 인하여 발생하는 보체계 활성화, 항체 매개성 세포 의존성 세포독성, 항원제시세포 및 내피세포의 활성화 등이 진행되는 것을 예방하게 된다[12]. 혈장교환술도 같은 목적으로 intravenous immunoglobulin과 함께 사용될 수 있다.
5) 보체 활성 억제
(1) C5 inhibitor (eculizumab)
항체가 면역반응을 유발하고 세포독성을 유발하는 방식 중에 하나는 보체계를 활성화시키는 것이다. 보체계가 활성화되는 과정 중 C5는 중요한 역할을 한다. C5a는 중성구에 대하여 화학주성을 유도하고, C5b는 염증반응이 발생한 세포의 세포막에 구멍을 만드는 membrane attack complex를 형성한다. C5에 대한 인간화 항체인 eculizumab은 C5에 결합하여 C5a와 C5b로 나뉘어 지는 것을 막음으로써 보체계 활성화로 인한 세포손상을 억제한다[13]. 비정형 용혈성 요독증후군으로 인한 신손상의 치료에 효과적이라는 보고들을 바탕으로, 항체 매개성 거부반응의 치료에 적용하고자 하는 시도가 진행 중이다[14].
면역억제제의 임상적용
1. 유도면역억제제
1) 유도면역억제제의 면역학적 필요성
이식편이 수혜자의 신체 내로 들어오게 되면 즉각적인 면역반응이 일어나게 된다. 기증자에 특이적인 T세포와 선천성 면역계가 이식 초기에 활성화되며 이식편에 대한 강력한 면역반응이 발생하게 된다[15]. 유도면역억제제는 강력한 면역억제제로 이러한 이식 초기의 면역반응 및 거부반응을 예방하기 위한 목적으로 사용된다. 국내에서는 고용량 스테로이드, IL-2 수용체 길항제(basiliximab) 및 ATG가 주로 사용되고 있다.
2) 유도면역억제제의 임상적용
2010년 Cai 등[16]은 UNOS (United Network for Organ Sharing)에 등록된 데이터를 분석하여 유도면역억제제의 종류에 상관없이, 유도면역억제제를 사용하는 것이 신장, 간, 폐 이식 후 이식편 생존율을 향상시킨다고 보고하였다. 이러한 연구결과를 바탕으로 유도면역억제제의 사용은 점차 증가하고 있으며, Scientific Registry of Tra-nsplant Recipients의 보고서에 따르면, 2018년 미국에서 신장이식 및 췌장이식의 90%에서 유도면역억제제가 사용 되었고 ATG와 같은 T세포 고갈 약제가 가장 많이 사용되었다. 하지만, 유도면역억제제의 이용은 장기별로 차이를 보이고 있는데, 간이식의 경우 2018년 미국에서 30%의 수혜자에게만 유도면역억제제가 사용되었고, basiliximab과 같은 IL-2 수용체 길항제가 가장 많이 사용되었다. 신장이식의 경우, T세포 고갈 약제와 IL-2 수용체 길항제 중 어느 유도면역억제제를 사용할 것인가 에 대한 연구가 많이 진행되고 있으나, 아직까지 이식편의 생존율에 유의미한 장점을 가지는 약물이 확실하게 밝혀지지는 않았다[16]. 간이식의 경우, 유도면역억제제의 사용이 이식편의 생존율을 향상시키는가에 대한 논의가 아직 진행중이다[17,18]. 심장 및 폐이식의 경우에도 유도면역억제제의 효용성에 대한 연구가 진행 중이며, 폐이식 분야에서는 이식편 생존율에 긍정적인 영향을 미친다는 연구가 보고되고 있으나[19-21], 심장이식 분야에서는 아직 생존율 향상에 대한 논의가 아직 진행중이다[22,23].
2. 유지면역억제제
1) 유지면역억제제의 필요성
유도면역억제제는 면역억제 능력이 매우 뛰어나지만, 그에 동반되는 합병증 또는 감염의 위험성이 너무 크기 때문에 오랫동안 사용이 불가능하다. 그러므로 면역억제 능력이 떨어지더라도 비교적 감염의 위험성이 적어, 장기이식환자들이 지속적으로 복용을 하면서 거부반응을 예방할 수 있는 유지면역억제제가 필요하다.
2) 유지면역억제제의 임상적용
최근에는 칼시뉴린 억제제의 한 종류인 tacrolimus를 기반으로, 항대사제인 mycophenolate, 그리고 스테로이드 세 가지 약물을 같이 사용하는 3제 요법이 가장 흔하게 이용된다. Scientific Registry of Transplant Recipients의 보고에 따르면 2018년 미국에서 시행된 신장이식, 간이식, 및 췌장이식의 60%에서 이러한 3제 요법이 사용되었다. 나머지 40%의 대부분 역시 tacrolimus와 mycophenolate 또는 스테로이드를 조합한 2제 요법이 사용되었다. 이러한 유지면역억제제의 이용으로 이식 초기의 거부반응을 억제하고
1년 이식편 생존율은 향상시킴으로써, 이식편의 장기생존률을 크게 향상시킬 것으로 기대하였으나, 기대만큼 큰 향상이 없다는 점이 여러 연구를 통하여 보고되었다[24-26]. 이러한 결과는 면역억제로 인한 기회감염의 증가, 암발생의 증가, 대사성 질환의 발생 그리고 칼시뉴린 억제제로 인한 신독성 등이 원인인 것으로 나타났다[27].
이러한 면역억제제의 부작용을 최소화하면서도 거부반응을 효과적으로 억제하는 유지면역억제요법을 찾기 위한 연구가 최근 장기이식 분야의 가장 큰 화두이며, 스테로이드 중단[28], 칼시뉴린 억제제 용량 최소화[29], 면역억제제 개별화[30], 면역관용 유도[31-34] 및 신약의 적용[35-37] 등이 시도되고 있다. 또 다른 방향으로, 가장 효과적인 약물의 혈중 농도 최저치를 찾기 위한 연구들[38,39], 그리고 개별 환자내 약물 농도 차이를 줄이고 환자의 약물 순응도를 증진시키기 위한 여러가지 시도 역시 진행되고 있다[40,41].
결론
이식 후 면역반응에 대한 이해가 높아짐에 따라 효과적인 면역억제제가 많이 개발되어, 장기이식 후 이식편의 생존율은 괄목할만한 성장을 이루었다. 하지만 안정성 측면과 장기 생존율 측면에서 아직까지 개선의 여지가 있으며, 보다 안전하게, 오랫동안 이식편을 유지하기위한 노력이 지속되고 있다. 이러한 시도들로부터 도출되는 결과들을 토대로 이식편의 장기 생존율과 더불어 이식 수혜자의 생존율 및 삶의 질이 점차 향상될 것으로 기대된다.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
References
Peer Reviewers’ Commentary
이 논문은 장기이식 후 발생하는 면역 반응과 함께 장기이식 후 사용하는 다양한 면역억제제의 기전을 기술하고, 실제 장기이식 후 임상에서 사용되는 면역억제요법에 관한 최신 지식을 정리한 논문이다. 장기이식은 장기 부전의 가장 효과적인 치료로, 면역억제제가 발달함에 따라 그 성적이 향상되어왔다. 장기이식 후 거부반응은 크게 T세포 매개 거부반응과 항체 매개 거부반응으로 나뉜다. 이 논문에서는 이들 거부반응의 기본적 면역 반응을 소개하고, 각 면역억제제가 이들 면역 반응 중 어느 부분을 목표로 작용하고 있는지 알기 쉽게 기술하였다. 현재 사용되는 다양한 면역억제제들에 대한 소개와 함께 앞으로 면역억제치료가 나아가야 할 방향까지 제시하여, 장기이식 분야에서 면역억제제를 이해하는데 좋은 정보를 줄 것으로 판단된다.
[정리: 편집위원회]