고관절 치환술과 관련된 한국의 역학적 특성과 추세
Korean epidemiology and trends in hip joint replacements
Article information

Trans Abstract
This study aimed to analyze the epidemiologic characteristics of patients who underwent hip arthroplasty using the Korean nationwide database and investigate the recent trends in implant fixation methods and bearing surface selection. We aimed to compare clinical characteristics and differences with the results from the registry of other western countries. We analyzed the data collected by the Health Insurance Review and Assessment Service database of Korea from 2007 to 2011 and the Main Surgery Statistical Yearbook from 2014 to 2018, published by the National Health Insurance Service. The number and rate of patients who underwent hip joint arthroplasty per 10,000 persons have been steadily increasing since 2007. There was a big difference in mean age and preoperative diagnosis of patients between the bipolar hemiarthroplasty and total hip arthroplasty groups. Most patients underwent surgery using a cementless biological fixation method, and the cemented fixation method was selectively used for a small portion of old aged osteoporotic patients. In relation to the use of bearing surfaces, the registry data showed that ceramic-ceramic bearings were used at an overwhelmingly high rate (81%) in Korea compared to other countries. The reason was attributable to various factors, such as patient’s age or economic status, differences in the health insurance system between countries, and recently reported complications, such as ceramic fracture or noise.
서론
고관절 치환술은 퇴행성 관절염이 진행되거나 고관절 골절이 발생한 환자에서 통증 완화 및 관절기능의 회복을 위해 사용할 수 있는 효과적인 치료법 중의 하나이다[1]. 1960년대 John Charnley에 의해 근대적인 개념의 저마찰 관절치환술이 처음 시도된 이후, 고관절 치환술은 생명공학기술 및 수술 기법 등의 발전에 힘입어 비약적인 발전을 거듭하였다[2]. 처음 인공관절이 시도된 목적은 환자의 통증 완화였으나, 최근에는 관절운동 범위 및 기능의 회복까지도 가능 해졌으며, 보건 경제학적인 측면에서도 비용효율이 높은 수술로 받아들여지고 있다. 이러한 이유로 고관절 전치환술은 2007년 Lancet에 ‘20세기 최고의 수술’로 소개된 바 있다[3].
고관절 반치환술, 고관절 전치환술, 고관절 재치환술을 포함하는 고관절 치환술 총 시행 건수는 전 세계적으로 매년 증가하는 추세이다[4,5]. 고령화 사회의 진입과 평균수명의 증가와 관련하여 고관절질환 환자 및 골다공증성 고관절 골절 환자는 앞으로도 꾸준히 증가할 것으로 예상되기 때문에 고관절 치환술 건수 역시 지속적으로 증가할 것으로 추정된다[5,6]. 이러한 증가 추세에도 불구하고, 수술 시 사용되는 삽입물의 종류 및 고정방법, 관절면의 종류 등은 환자의 진단, 연령, 동서양의 지역적인 특성 등 여러 가지 요인에 의해 차이를 보인다. 따라서 본 연구에서는 2007년부터 최근까지의 한국 건강보험심사평가원 자료를 바탕으로, 한국에서 시행된 고관절 치환술 환자들의 역학적 특성과 현재의 추세에 대해 고찰하고자 한다. 또한, 수술 적응증 및 환자군의 특성에 있어 서양과 한국의 차이점에 대해 추가적으로 분석해보고자 한다.
환자의 역학적 특성
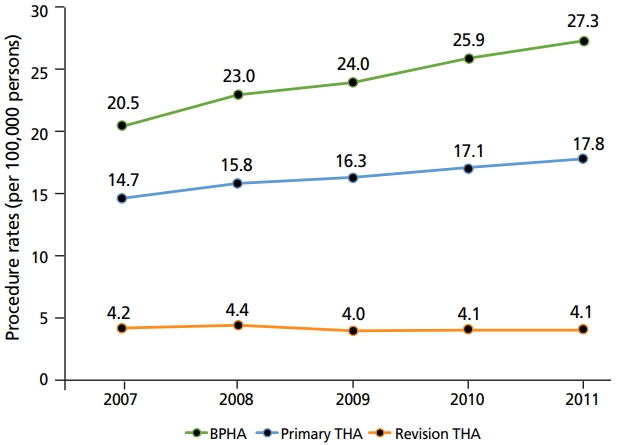
2007년부터 2011년도까지 인공고관절술을 시행 받은 환자들의 건강보험심사평가원 자료를 대상으로 한 선행연구에 따르면, 연도별 인구 10만 명당 수술 건수 증감추이를 분석하였을 때 고관절 반치환술은 매년 1.7%, 고관절 전치환술의 경우 매년 0.8% 증가하였다. 재치환술을 포함한 총 고관절 치환건수는 2007년 19,380명에서 2011년 24,682명으로 증가해 6.2%의 연평균 증가율을 보였으며, 2014년부터 2018년까지의 주요수술통계 연보에 의하면 총 고관절 치환건수는 2014년 26,036명에서 2018년 29,317명으로 약 3.0%의 연평균 증가율을 보였다(Figure 1) [7]. 하지만 경제협력개발기구 보건통계에 따르면 한국의 고관절 치환술 환자 수는 10만 명당 56건 내외로 경제협력개발기구 평균(10만 명당 182건)에는 훨씬 미치지 못하는 상태이다[8].
국내에서 고관절 반치환술을 받는 경우는 대부분 대퇴골 경부 골절 및 전자간 골절로 63% 이상의 환자가 75세 이상이다. 고관절 전치환술을 시행 받은 환자들의 주 진단은 대퇴골두 골괴사가 가장 많은 비율을 차지하였고(59%), 골관절염이 28%로 뒤를 이었다. 고관절 전치환술을 받는 환자의 약 65% 이상이 65세 이하로 고관절 반치환술 환자군에 비해 평균 연령이 상대적으로 낮았다. 성비 역시 두 군 간 의미 있는 차이를 보이는데, 고관절 반치환술을 시행 받은 환자군은 여자 환자의 비율이 74.0%로 남자 환자에 비해 약 3배 정도 높은 반면, 고관절 전치환술을 시행 받은 환자군은 남자 환자의 비율이 55.8%로 남자 환자가 여자 환자에 비해 더 많은 것으로 확인되었다[7]. 이는 대퇴골 경부 골절 및 전자간 골절의 경우 여성 환자에서 주로 발생하는 특징이 있고, 반대로 대퇴골두 골괴사는 남자가 여자에 비해 3-4대 1의 비율로 더 많이 발생하는 것으로 알려져 있기 때문이다. 한편. 미국 환자들에 대한 분석결과에 의하면 고관절 전치환술을 시행 받은 환자의 약 60%가 평균 연령 65세 이상으로 한국과 비교해 평균 연령이 높은 편이었으며, 주 진단 역시 골관절염이 약 81%로 가장 흔해서 한국의 경우(28%)와 큰 차이가 있었다[9]. 한국에서 고관절 전치환술을 시행 받는 가장 흔한 원인인 대퇴골두 골괴사는 골관절염에 비해 비교적 젊은 연령대인 30-50대에서 호발하기 때문에 두 군 간 평균 연령에 차이가 나는 것으로 해석된다[10]. 또한 고관절 골관절염의 경우, 한국을 포함한 동양인에서는 서양인에 비해 유병률이 적은 것으로 알려져 있다. 원인으로는 민족적·인종적 차이, 환자의 체질량지수, 신체활동의 차이 등 다양한 원인들이 제시된 바 있다[11,12].
고정방법
1950년대 시멘트형 고관절 치환술의 양호한 임상성적이 보고된 이후 오랜 기간 시멘트형 삽입물 고정법이 널리 행해졌으나, 1970년대 말 대두된 고관절 골용해 및 삽입물 해리의 원인으로 시멘트 고정술이 지목되면서 무시멘트형 고관절 치환술을 이용한 생물학적 고정법이 급격하게 발전하게 되었다. 국내에서도 역시 초기에는 시멘트형 고관절 치환술이 주로 시행되었으나, 현재는 대부분 무시멘트형 치환술이 시행되고 있다. 2014년부터 2018년까지 무시멘트형 대퇴스템 사용의 빈도는 80%에서 87%로 매년 증가하고 있는 추세이다(Figure 2). 미국의 경우 역시 한국과 유사한 추세를 보이고 있으며, 2001년부터 2012년까지 무시멘트형 대퇴스템 사용빈도는 꾸준히 증가하고 있다(Figure 3) [13].
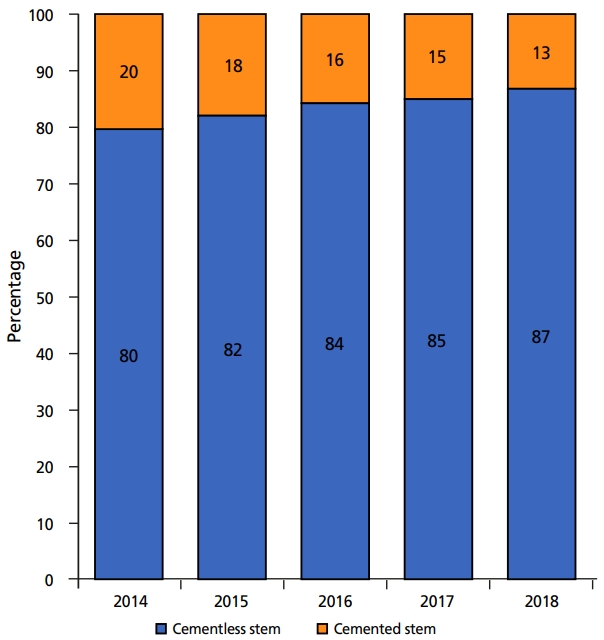
Change in the trend of using bone cement to fix the femoral stem in hip replacement in Korea from 2014 to 2018.
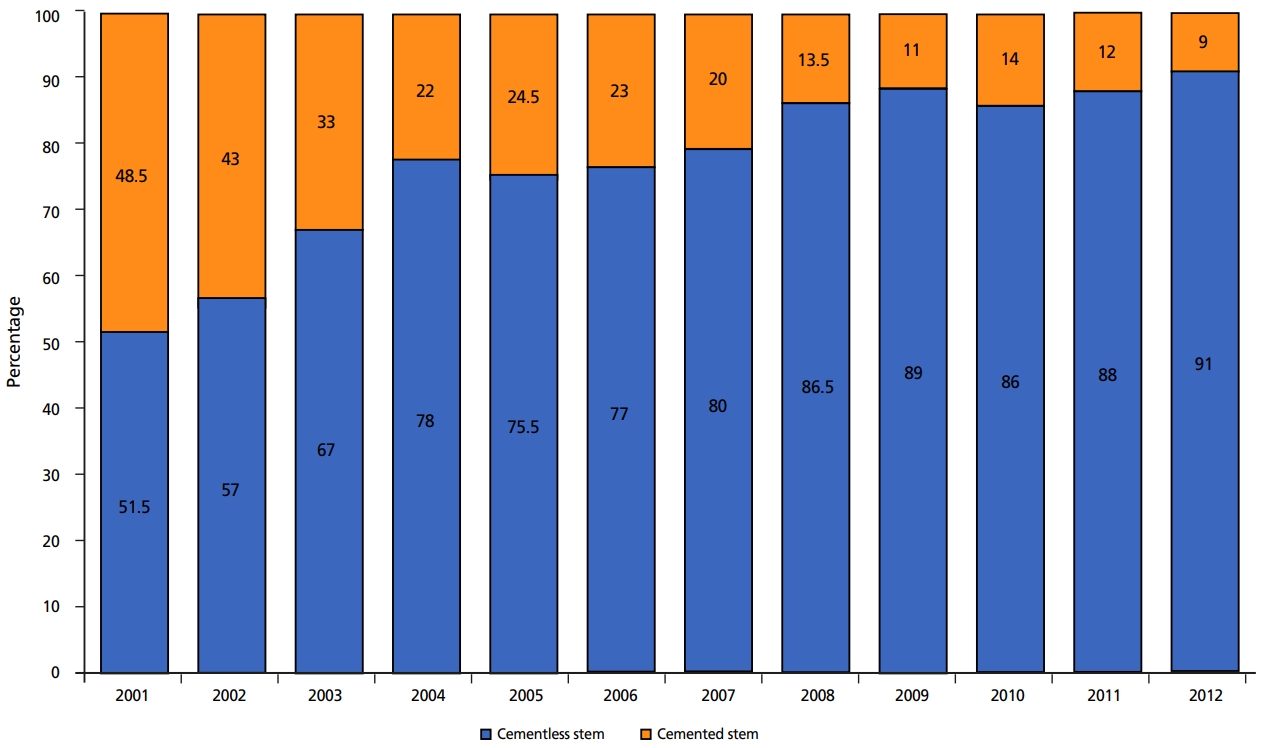
Change in the trend of using bone cement for fixation of the femoral stem in hip replacement in the United States from 2001 to 2012.
한편, 유럽의 경우에는 아직까지 시멘트형 대퇴스템이 상대적으로 많이 사용되고 있고, 영국의 경우 시멘트형 고관절 치환술의 비율이 점차 증가하고 있어 2024년에는 무시멘트형 고정술을 시행 받는 환자수를 넘어설 것으로 예상하고 있다[14]. 시멘트형 대퇴 스템은 초기 고정력이 우수하기 때문에 고령의 환자나 류마티스 관절염 환자, 삽입물로의 골내성장을 기대하기 어려운 환자에서 주로 이용하고 있는데, 영국의 2017년도 National Joint Registry에 의하면, 시멘트형 고관절 치환술 시행 군에서 인공관절 재치환율이 가장 낮았다[14]. 또한 최근 발표된 논문에서는 75세 이상의 환자 중 시멘트형 고관절 전치환술을 시행한 환자군이 무시멘트형 고관절 전치환술을 시행한 환자군과 비교해 골절 및 해리 등으로 인한 술 후 30일 이내 조기 인공관절 재치환율이 유의하게 낮았다고 보고하였다[15]. 한편, 무시멘트형 고관절 치환술의 경우 시멘트형 치환술에 비해 수술시간이 유의하게 짧고, 재치환술 시 시멘트의 제거 필요성이 없어 수술이 수월해지고 골조직 손상의 적다는 장점이 있다[16]. 이처럼 고관절 치환술에서의 적절한 고정방법에 대한 논란은 아직까지 지속되고 있으며, 환자의 전신 상태와 활동 정도, 근위 대퇴골의 형태 등을 고려한 임상적인 판단이 요구된다[16-21].
인공 관절면
인공 관절면은 현재까지도 고관절 치환술에서 가장 중요한 쟁점 중 하나이다. 1950대 후반 John Charnley가 고밀도 폴리에틸렌을 사용한 저마찰 관절치환술을 처음 도입하였고, 이후 코발트 합금 골두와 초고분자량 폴리에틸렌 비구라이너(liner)가 개발되면서 고관절 치환술 시 주된 관절면으로 사용되어 왔다. 하지만, 폴리에틸렌 마모 입자의 생물학적 반응에 의해 발생하는 삽입물 주위 골용해는 고관절 치환술의 수명에 중요한 영향을 미치게 되었고, 그 대안으로 금속-금속, 세라믹-폴리에틸렌, 세라믹-세라믹 관절면이 등장하는 계기가 되었다. 세라믹 관절면의 경우 기존 3세대 세라믹 관절면보다 취성이 높고 마모율이 낮은 4세대 세라믹(Biolox Delta, CeramTec, Plochingen, Germany)이 보급되어 현재까지 우수한 임상 성적을 보고하고 있으며, 폴리에틸렌 관절면 역시 기존의 초고분자량 폴리에틸렌보다 마모율이 훨씬 낮은 고도 교차결합 폴리에틸렌이 개발되어 임상적으로 널리 사용되고 있다.
2007년부터 2011년까지 한국에서 시행된 인공고관절 전치환술 전체 건에 대한 인공관절면의 사용빈도는 세라믹-세라믹 관절면(76.7%)이 가장 높았으며, 금속-폴리에틸렌 (11.9%), 세라믹-폴리에틸렌(7.3%), 금속-금속(4.1%) 관절면이 그 뒤를 이었다[22]. 조사 기간 동안 세라믹-세라믹 관절면 사용빈도는 71.6%에서 81.4%로 지속적인 증가세를 보인 반면, 다른 관절면의 사용빈도는 모두 유의하게 감소하였다(P<0.001) (Figure 4). 또한 이러한 인공 관절면의 사용빈도의 순서는 환자의 나이, 성별, 병원의 종류 등과는 관련이 없는 것으로 확인되었다[22].
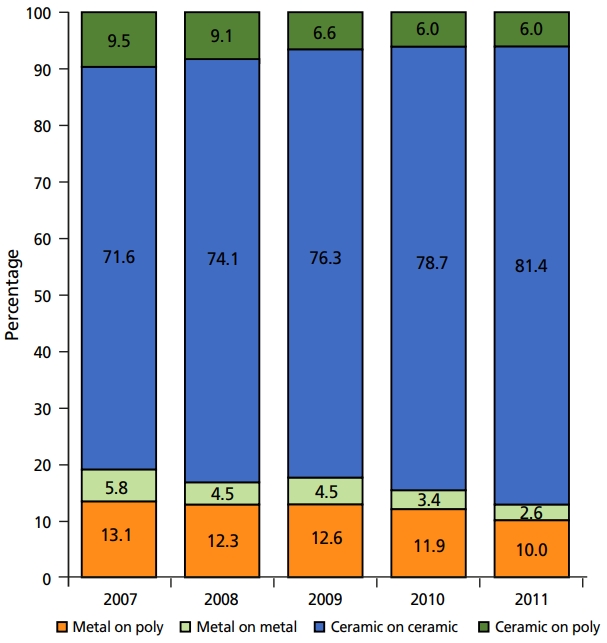
Bearing surface utilization by year as a proportion of all total hip arthroplasties performed in Korea from 2007 to 2011.
미국과 한국에서 사용하는 인공 관절면의 종류와 그 빈도는 뚜렷한 차이를 보이는데, 미국의 입원환자 샘플(Nationwide Inpatient Sample) 등록자료에 의하면 2007년도 가장 많이 사용된 관절면은 금속-폴리에틸렌(44.3%)이었으며, 금속-금속(37.6%), 세라믹-폴리에틸렌(11.1%), 세라믹-세라믹(7.0%) 관절면이 그 뒤를 이었다. 이후 2014년까지 금속-금속 관절면은 사용빈도가 37.6%에서 4.0%로 급격히 감소하였으며, 반대로 세라믹-폴리에틸렌 관절면은 사용빈도가 11.1%에서 50.8%로 급격히 증가하였다(Figure 5) [3,23].
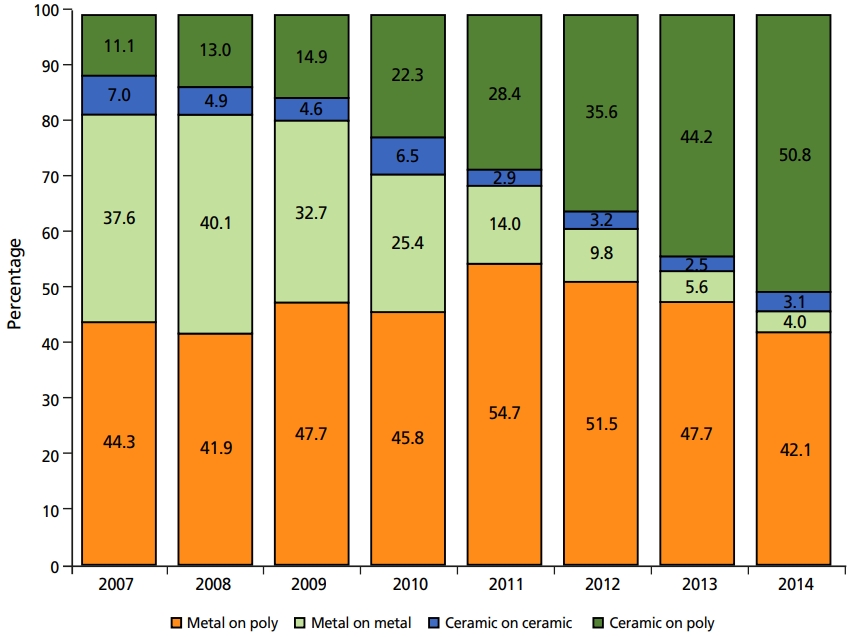
금속-금속 관절면 사용의 급격한 감소와 관련하여, 2011년 2월 미국 식품의약국에서 금속 파편으로 인한 연부조직 이상반응을 보고한 바 있다. 연구진들은 유리된 금속 이온 및 마모 입자들이 체내에서 지연성 세포 매개 과민반응을 일으킬 수 있으며, 일부 환자에서는 ALVAL (aseptic lymphocytic vasculitis associated lesions) 반응을 유발할 수 있다고 보고하였다. 그 외에도 금속 마모 입자로 인한 발암 가능성, 태아 독성 및 기형 발생의 위험 등 여러가지 생물학적 이상반응의 발생 가능성이 있다고 발표하였고, 위 보고가 발표된 후 금속-금속 관절면의 사용은 급감하게 되었다[24,25]. 2007년부터 2012년까지의 미국 내 174개 병원의 고관절 전치환술 데이터를 조사한 Lehil과 Bozic [13]의 연구에 의하면, 해당 기관들의 금속-금속 관절면의 사용 빈도는 5년 사이 31%에서 불과 1%로 급격히 감소하였다.
세라믹-세라믹 관절면의 사용빈도에 있어 미국(2011년도 기준, 2.9%)과 한국(2011년 기준, 81.4%)은 매우 큰 차이를 보이는데, 환자의 평균연령 차이가 중요한 인자 중 하나에 해당한다. 한국의 경우 고관절 전치환술을 받는 환자들의 평균나이가 58.1세인 반면, 미국 환자들의 평균나이는 65.1세로 한국 환자들은 미국 환자들에 비해 상대적으로 젊다. 이는 수술을 받는 환자 중에서 대퇴골두 골괴사의 비율이 높고, 고관절의 골관절염이 드문 한국과, 고령의 골관절염 환자가 주를 이루는 미국과의 인종적, 사회 환경적 차이에 기인한다. 한국에서는 환자의 나이와 인공 관절면의 수명을 고려해 상대적으로 마모율이 적고 수명이 긴 세라믹-세라믹 관절면을 선호하는 경향이 있다[22,23].
한편 세라믹-세라믹 관절면 이용률은 미국 내에서도 기관별, 지역별로 큰 차이가 있는데, 연구에 의하면 도심지 병원의 경우 세라믹-세라믹 관절면 이용률이 시골 병원보다 3-5배 높았으며, 사립병원의 경우 공공병원보다 이용률이 3-5배 높았다. 반대로 사립병원의 세라믹-폴리에틸렌 관절면 사용빈도는 공공병원의 절반밖에 되지 않는 것으로 보고되었다[26]. Bozic 등[27]은 미국에서는 세라믹-세라믹 관절면의 가격이 높고 수명이 긴 프리미엄 제품으로 취급되기 때문에, 공공 의료보험 환자들에 비해 경제적 여유가 있는 사보험 환자들이 세라믹-세라믹 관절면을 더 많은 빈도로 사용하고 있다고 밝혔다. 하지만 한국의 경우 의료보험 정책으로 인해 인공 관절면의 종류에 따른 가격의 차이가 거의 없으므로, 환자의 경제적 능력이 아닌 술 자의 선호도 및 임상적 판단에 따라 관절면의 종류를 선택하게 된다.
세라믹 관절면과 관련된 합병증은 상대적으로 드물게 발생하지만 세라믹 파손과 소음 문제가 보고되고 있다[28-30]. 한편 최근 출시된 고도 교차결합 폴리에틸렌 라이너가 기존 폴리에텔렌 라이너에 비해 낮은 마모율과 우수한 임상성적을 보이고 있으며, 금속 골두와 대퇴 스템의 경부 사이의 틈에서 발생하는 틈부식이 인공관절 전치환술 실패의 또 다른 원인 중 하나로 알려지게 되었다[31-38]. 이러한 여러가지 이슈들은 미국 내에서 세라믹-폴리에틸렌 관절면을 선호하는 근거가 되고 있으며, 최근 한국 역시 미국과 같이 세라믹-폴리에틸렌 관절면 사용의 빈도가 점차적으로 증가하는 추세이다(Figure 6).

Proportion of acetabular liner type by year (Korea) Recent trend for polyethylene and ceramic liner usage in total hip arthroplasty in Korea from 2014 to 2018.
새로운 디자인의 인공관절 삽입물(비구컵)
현재 사용되는 금속 삽입물 디자인은 John Charnley가 고안한 저마찰 관절치환술을 기반으로 발전해왔다. 하지만 초기에 소개된 인공관절 삽입물은 비교적 양호한 임상 성적에도 불구하고 폴리에틸렌 비구 라이너의 마모, 관절 탈구 등의 합병증이 문제가 되어 왔다. 이러한 합병증에 대한 관심이 높아지면서, 과거 1974년 Gilles Bousquet와 André Rambert가 최초 디자인한 이중 운동 비구컵이 새롭게 관심을 받게 되었다[39]. 이중 운동 비구컵은 큰 관절면을 가지는 외측, 그리고 작은 관절면을 가지는 내측으로 구분되는 두 개의 관절면으로 이루어져 있으며, 통상적인 인공고관절전치환술보다 기능적으로 큰 골두를 이용할 수 있게 되었다(Figure 7). 큰 골두 사용 시 관절 운동범위가 증가하고, 기구 충돌이 감소하며, 탈구 유발 거리를 증가하게 되므로, 결과적으로 인공 관절 탈구를 줄일 수 있는 장점이 있다. 최근까지 여러 연구에서 이중 운동 비구컵의 우수한 임상 성적 및 낮은 탈구 합병률을 보고하였으며, 그 대상은 재치환술 환자[40-42] 외에, 대퇴골두 무혈성 괴사 환자[43], 고관절 골절 환자[44,45], 젊은 연령 환자[46,47]에 걸쳐 다양하다.

Components of dual mobility cup (Modular Dual Mobility acetabular system; Stryker, Mahwah, NJ, USA). The system consists of cobalt-chrome liner, polyethylene liner, and femoral head. (Courtesy of Stryker).
이중 운동 비구컵 연도별 사용빈도의 변화에 관한 Registry 분석은 한국을 포함해 아직까지 보고된 바 없으나, 기구의 사용과 관련한 연구발표는 최근 10여년에 걸쳐 급격하게 증가하는 추세이다. 이중 운동 비구컵과 관련한 전 세계 논문 보고수의 변화는 Figure 8과 같다. 한국의 경우 역시 아직까지 공식적인 국가등록자료 등의 분석 결과가 보고된 바 없으나, 인공관절 재치환술 환자, 재발성 탈구 환자에서부터 노인성척추후만증으로 인한 골반 후방 경사가 심한 환자, 고관절 골절 환자 등으로 그 적용범위가 넓어지고 있으며 사용빈도 역시 꾸준히 증가하고 있다.
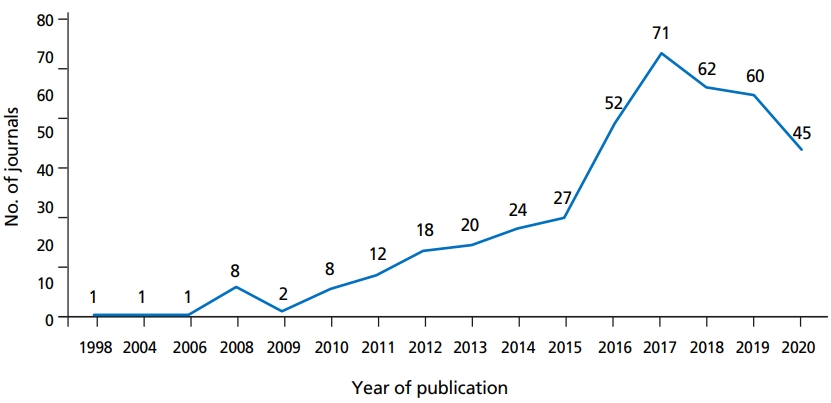
Increase in number of journals published worldwide for more than 20 years, regarding “Dual Mobility Cup”.
하지만, 초기 모델에 삽입된 고밀도 폴리에틸렌 관절면의 마모로 인한 삽입물의 무균성 해리(1.1-1.4%)와 인공삽입물 내 탈구(0.3-4%) 등의 중장기적 합병증이 보고된 바 있으며, 금속 비구 라이너의 마모로 인한 혈중 금속이온농도 상승 역시 보고된 바 있다[48-50]. 따라서 이중 운동 비구컵의 장기추시 결과 및 합병증에 대해서는 추가적인 분석이 필요할 것으로 판단된다. 또한 관절면 마모는 아직까지 충분히 검증된 바는 없으나, 기존 고밀도 폴리에틸렌 관절면을 초고분자량 폴리에틸렌 관절면으로 대체함으로써 라이너 마모를 감소시킬 수 있을 것으로 기대하고 있다.
결론
고령화 사회로의 진입 및 신체활동의 증가로 인해 고관절 치환술 환자는 앞으로도 꾸준히 증가할 것으로 예상된다. 하지만 환자의 수술 전 진단이나 연령과 같은 역학적인 특성에 따라 시행되는 고관절 치환술의 종류에는 차이가 있으며, 환자 분포 역시 다른 나라의 자료와 분명한 차이를 보인다. 고관절 반치환술 및 전치환술 환자는 전세계적으로 계속 증가하고 있으며, 골관절염이 고관절 전치환술의 주를 이루는 서양과 달리 한국은 골관절염의 유병률이 낮고 대퇴골두 골괴사 환자의 비율이 상대적으로 높으며, 평균연령 역시 낮다.
이러한 차이는 삽입물 고정법 및 인공 관절면 종류의 선택에도 큰 영향을 미치게 된다, 한국의 경우 환자들이 상대적으로 젊고, 활동적이기 때문에 관절면 마모율이 상대적으로 낮고, 장기 임상 결과가 양호한 무시멘트형 인공관절 삽입물 및 세라믹-세라믹 관절면을 선호하는 경향이 강하다. 하지만, 세라믹 라이너의 부적절한 삽입, 세라믹의 파손, 세라믹 관절면의 소음 발생 등 합병증이 지속적으로 보고되면서 최근 수 년 사이 세라믹-폴리에틸렌 관절면 사용을 선호하는 새로운 경향이 관찰되고 있다.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
References
Peer Reviewers’ Commentary
이 논문은 2007년부터 2011년까지의 건강보험공단 자료와 2014년부터 2018년까지의 주요 수술통계연보를 이용하여 우리나라의 고관절치환술의 현황 및 추세를 환자의 역학적 특성, 삽입물의 고정방법 및 관절면의 종류에 따라 분석하고 이를 미국 및 영국 등 서구의 나라들과 비교해 주고 있다. 고관절 치환술은 국내에서 점점 증가하고 있고, 부분치환술은 고관절 골절, 전치환술은 골괴사가 주요 원인이며, 무시멘트형 치환술이 대부분을 차지하고, 관절면으로는 세라믹-세라믹 관절면의 빈도가 높음을 설명하고 있다. 이 논문은 일차의료를 담당하는 의사들이 국내 고관절치환술의 현황과 인공고관절수술을 이해하는데 많은 도움을 줄 것으로 판단된다.
[정리: 편집위원회]