면역관문억제제를 이용한 항암치료의 부작용 관리
Management of adverse events in cancer treatment with immune checkpoint inhibitors
Article information

Trans Abstract
The use of immune checkpoint inhibitors is associated with a spectrum of immune-related adverse events related to the mechanism of action which is quite different from that of cytotoxic chemotherapy. Adverse effects can affect multiple organs of the body and are most common in the skin, gastrointestinal tract, lungs, and endocrine tissues, including the thyroid, adrenal gland, pituitary gland, as well as musculoskeletal, renal, nervous, hematologic, cardiovascular, and ocular systems. Any changes should be considered as being related to treatment with immune checkpoint inhibitors. Adverse events are very infrequent, but may be very serious and, even lethal, such as neurological disorders and myocarditis. When compared with standard chemotherapeutic agents, programmed death 1/programmed deathligand 1inhibitors are associated with a lower incidence of bone marrow suppression, anorexia, nausea, vomiting, and diarrhea. Immune checkpoint inhibitor therapy can usually continue in the presence of mild immune-related adverse events with close monitoring. However, moderate to severe immune-related adverse events may be associated with a severe decline in organ function and quality of life, and may result in fatal outcomes. Hence, these toxicities require early detection and proper management. The management of immune-related adverse events usually involves corticosteroid therapy or the use of immunomodulators. The use of immune checkpoint inhibitors in patients with preexisting autoimmune disease or a history of prior organ transplant should include careful consideration and a robust discussion of potential risks and benefits.
서론
현재 전신 항암치료는 기존의 세포독성항암제, 표적치료제 그리고 최근의 면역관문억제제를 통해 이루어지고 있다. 세포독성항암제는 암세포뿐 아니라 빨리 성장하는 정상세포의 분화에도 영향을 미치기 때문에 혈구감소, 탈모, 오심, 구토 등 개인 간 정도의 차이는 있겠으나 비슷하고, 예측 가능한 부작용을 보인다. 또한 표적치료제는 암세포의 성장에 주요한 열쇠인 특정 수용체에 결합하여 암세포의 성장을 억제하는 것으로 예를 들면, 피부발진 등 세포독성항암제와는 또 다른 양상의 부작용을 보인다.
최근 여러 종류의 암 치료에 있어서 주목받고 있는 면역관문억제제(면역항암제)는 우수한 암 치료성적뿐 아니라 기존의 세포독성항암제에서 보이는 혈구감소, 오심, 구토, 탈모 등의 부작용이 거의 없기 때문에 독성이 적은 약으로 알려져 있다. 하지만 기존의 세포독성항암제와는 다른 부작용을 보인다는 것이지 부작용이 없는 약은 아니다. 대부분 경한 부작용이나, 보고에 따르면 드물지만 치명적 부작용을 일으키기도 한다. 이것은 이 약제가 가진 항암기전이 재활성화된 T세포가 암세포를 공격하기 때문이다. 이 과정에서 여러 가지 사이토카인들이 분비되면서 염증반응을 일으키게 되고 여러 장기들을 침범하면서 과거의 약들과는 다른 부작용을 일으키게 된다. 구체적으로 어떻게 부작용을 일으키는지 정확한 병태생리는 알려지지 않았지만, 우리 몸의 면역시스템에 영향을 주어 일으키는 것으로 받아들여지고 있다[1]. 이는 기존의 세포독성항암제와는 다른 부작용으로 이를 두고 면역 관련 부작용으로 부르고 있다. 면역관문억제제로 암을 치료할 때 그 효과도 잘 알아야겠지만 어떠한 부작용이 나타날지에 대해서도 잘 알아 두어야 조기에 대처가 가능할 것이다. 따라서, 이 논문에서는 최근 암 치료에 새로운 패러다임을 제시한 면역항암제의 부작용에 대해 알아보고, 부작용이 발생하였을 때 어떻게 조치해야 하는지에 대해서 논의하고자 한다.
면역관문억제제로 인한 면역 관련 부작용 스펙트럼
활성화된 면역세포가 온몸의 장기를 공격할 수 있기 때문에 면역관문억제제로 인한 부작용은 어떤 장기에서도 볼 수 있다(Figure 1). 현재 널리 사용되는 면역관문억제제로는 cytotoxic T lymphocyte antigen-4 (CTLA-4) inhibitor인 ipilimumab (Yervoy; Bristol Myers Squibb, New York, NY, USA), programmed death 1 (PD-1)/programmed death-ligand 1 (PD-L1) inhibitor인 nivolumab (Opdivo; Ono Pharmaceutical, Osaka, Japan/Bristol Myers Squibb), pembrolizumab (Keytruda; Merck Sharp & Dohme, Kenilworth, NJ, USA), atezolizumab (Tecentriq; Roche, Basel, Swiss) 및 durvalumab (Imfinzi; AstraZeneca, Cambridge, UK)이 있다. 두 약제, CTLA-4 inhibitor와 PD-1/PD-L1 inhibitor는 기전의 차이로 인해서 부작용을 더 잘 일으키는 장기에는 약간의 차이를 보이고 있으나, 앞서 언급한 대로 우리 몸의 면역시스템에 문제를 일으키는 것으로 자가면역질환을 많이 닮았다. 흔히 알려진 면역 관련 부작용으로는 위장관, 내분비계, 피부, 간 등에서 보고되고 있고, 이보다 드물게 신경계, 심혈관계, 호흡기계, 근골격계, 혈액, 신장계에서 부작용이 보고되고 있다(Table 1) [2-4]. 대부분 경한 부작용(mild, grade 1; moderate, grade 2)으로 나타나지만, 드물게 신경계통이나 심장계통에 발생 시 매우 심각하고 치명적인 것(severe, grade 3; lethal, grade 4)으로 보고되고 있다[5,6].
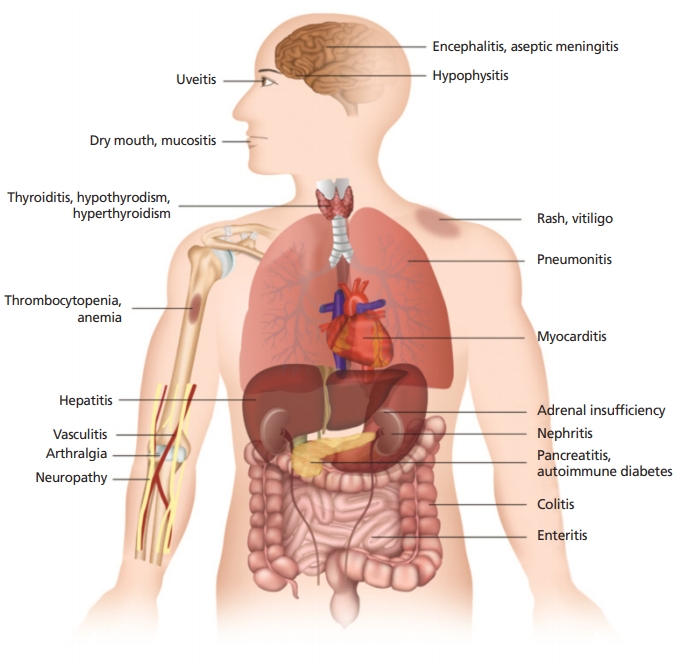
Immune checkpoint inhibitors can result in inflammation of any organ. This figure shows the most common immune-related adverse events in patients treated with immune checkpoint inhibitors. Courtesy of Inje University Haeundae Paik Hospital.

악성 흑색종을 CTLA-4 inhibitor인 ipilimumab으로 치료한 연구[7,8]에서는 전체 환자의 60-85%에서 면역 관련 부작용을 보였다. 대부분 grade 1-2 정도로 경한 부작용으로 나타났고, grade 3-4의 중한 부작용은 10-27%였다. 약제로 인한 부작용으로 사망한 경우는 2.1%로 나타났다. 이에 반해, PD-1/PD-L1 inhibitor들에서는 CTLA-4 inhibitor보다는 중한 부작용이 덜 한 것으로 알려져 있다. 비소세포폐암에 대한 nivolumab의 연구들에 따르면 전체 부작용은 58-69%에서 경험하였고, grade 3-4의 중한 부작용은 7-10% 정도로 보고되었다[9,10]. 물론 nivolumab과 ipilimumab을 함께 사용한 악성 흑색종 연구에서는 grade 3-4 부작용이 55%로 크게 증가한 양상을 보였다[8]. PD-1 inhibitor와 PD-L1 inhibitor의 부작용을 비교한 메타분석에서는 빈도 면에서 두 가지 약제에 큰 차이를 보이지 않았다[11].
이런 면역 관련 부작용이 일어나는 시기에 대해 살펴보면, 악성흑색종 치료에 nivolumab을 사용한 연구[12]에서 피부 부작용은 약 5주째, 위장관 부작용은 7.3주째, 간염은 7.7주째, 폐 부작용은 8.9주째, 내분비 부작용은 10.4주째 일어난 것으로 보고하고 있다. 평균적으로 약제 사용 이후 5-15주에 발생하는 것으로 보고되고 있으나, 사용 직후부터 몇 개월 이후, 심지어 약제 중단 이후에도 발생할 수 있다고 알려져 있다. 따라서, 환자가 호소하는 증상과 필요한 임상검사를 면역 관련 부작용과 연관 지을 수 있어야 하고 이에 대한 이해와 인식은 암을 치료하는 임상의들에게 꼭 필요한 사항이 되겠다.
면역관문억제제 치료 전 고려사항
치료 시작 전 먼저 부작용에 취약한 환자들을 선별하는 과정이 필요하다. 환자의 과거력, 가족력, 자가면역질환에 대한 조사가 선행되어야 한다. 따라서 치료 전 혈액검사 및 영상검사를 통해 이를 확인하고, 치료를 진행하면서도 치료 전 검사 결과와 비교하면서 이러한 부작용이 발생하지 않는지 추적 관찰이 필요하다. 흉부X선검사와 complete blood count, renal function, liver function, serum electrolytes, glucose, C-reactive protein, coagulation test를 포함한 혈액검사를 매 치료 전에 2-3주마다 검사하고 thyroid stimulating hormone, free T4, hemoglobin A1c, urine analysis를 매달 검사할 것을 권고하고 있다[13]. 만약 암 치료대상 환자가 자가면역질환을 가지고 있고, 자가면역조절제를 적극적으로 사용하고 있는 경우에 면역관문억제제로 치료하였을 경우 원래 가지고 있는 자가면역질환이 악화될 수 있다. 이러한 위험성으로 인해 이전의 많은 임상연구에서는 자가면역질환이나 사이질폐질환, 자가면역조절제를 사용하고 있는 환자의 경우에는 치료 대상이 되지 못하였다. 하지만 최근에는 소규모 연구들이긴 하나 자가면역질환을 가지고 있더라도 암 치료에 면역관문억제제의 높은 효과가 예상되는 경우 주의 깊게 사용할 수도 있음을 조심스럽게 언급하고 있다[14].
면역 관련 부작용 발생 시 임상에서의 적절한 대처방법
부작용이 발생하였을 경우 어떻게 대처하고 치료해야 하는지에 대한 전향적 연구가 없기 때문에 적절한 조치에 대해서는 아직은 임상적 경험에 바탕을 두고 있다. 하지만 조기에 적절한 조치를 할 경우에 부작용의 강도 및 기간을 줄일 수 있다고 보고되고[7] 있기 때문에 부작용 인지에 대한 환자 교육 및 의료진 교육이 필요하겠다. 또한 적절한 면역억제제(예: prednisolone)를 사용하거나 일시적 면역관문억제제 사용을 중지함으로써 대부분 경한 부작용을 조절할 수 있다. 다양한 장기 및 다양한 정도로 나타나는 부작용에 대해서 다양한 전문가들로 구성된 다학제팀의 접근이 필요하다. 매우 치명적이고 심각한 면역 관련 부작용 발생 시에는 종양내과뿐 아니라 면역 관련 부작용에 대해 인식하고 있는 호흡기내과, 소화기내과, 간내과, 심장내과, 내분비내과, 알레르기내과, 신경과, 피부과 등의 organ specialist들이 필요할 수 있겠다. 부작용 발생의 정도에 따라서 경중을 grade 1-4로 나누었을 때 grade 1인 경우에는 면역관문억제제를 유지하면서 경과관찰을 하고, grade 2인 경우 소량의 스테로이드를 사용하면서 경우에 따라서는 면역관문억제제 치료를 일시 중단하고 grade 1 정도로 호전되는지 경과를 볼 것을 권고하고 있다. 하지만 grade 3의 부작용을 보이면 약제 치료를 중단하고 입원 치료를 하면서 고용량의 전신 스테로이드를 사용하고, 3-5일 경과관찰 후 호전을 보이지 않을 경우 다양한 전문가들과 협업을 권고하고 있다. grade 3의 부작용을 보인 경우에, 호전되었다고 하더라도 면역관문억제제의 재사용은 득과 실을 잘 평가해서 판단할 것을 권고한다. grade 4의 중환자실에 갈 정도의 심각한 부작용이 발생하면 다학제팀과 함께 고용량 스테로이드뿐 아니라 다양한 면역억제제 및 면역조절제 치료, 예를 들면 tumor necrosis factor-α antagonist, azathioprine, mycophenolate mofetil, tacrolimus, cyclosporine 등을 시도해보고 면역관문억제제의 영구 중단을 권고하고 있다[3].
각 장기에서 나타나는 구체적 면역 관련 부작용 및 이에 대한 처치
1. 피부 부작용
피부 이상반응(rash, pruritus, vitiligo 등)은 가장 흔하게 나타나는 면역 관련 부작용으로 ipilimumab을 사용하였을 경우 약 45%, pembrolizumab을 사용하였을 경우 약 30%에서 나타났다. 하지만 중한 부작용 grade 3-4의 경우는 2-4%의 빈도를 보였다[7,15] (Figure 2). 경한 부작용은 국소 스테로이드제제 혹은 항히스타민제로도 조절이 가능하나 면밀한 경과관찰이 필요할 수 있다. Papulopustular rash가 발생하였을 경우에는 toxic epidermal necrolysis나 Stevens-Johnson 증후군으로 이행될 수 있으므로 피부과 협진이 반드시 필요하다.

Maculopapular rash on both lower extremities after pembrolizumab treatment. The skin rash covers >30% of the body surface area: development of grade 3 dermatologic adverse events.. The patient was admitted and treated with intravenous high dose (methyl)prednisolone (1 mg/kg/day IV) for 3 days with dermatologic consultation. Informed consent for publication of the clinical images was obtained from the patient.
2. 내분비계 부작용(갑상선기능이상, 뇌하수체염)
갑상선기능저하가 가장 흔히 볼 수 있는 내분비계 부작용으로 PD-1/PD-L1 inhibitor 사용 시 4-10%에서 발생하는 것으로 알려져 있고[16], ipilimumab 사용 시에는 좀 더 적게 발생하는 것으로 알려져 있다. 다른 부작용은 조기에 치료를 하면 호전을 보이나 내분비계 부작용은 장기적 치료가 필요한 경우가 많다. 갑상선기능저하를 보인 경우에도 지속적인 thyroxin 투여가 필요하게 된다. 이런 경우 thyroxin을 지속 투여하고 갑상선기능을 모니터링하면서 면역관문억제제를 사용을 유지해 볼 수 있다. 갑상선기능항진 또한 발생할 수 있으나, 1-7% 정도로 드물게 보고되고 있다. 1형 당뇨병도 발생할 수 있으나 PD-1 inhibitor에서 1% 미만에서 나타난다. 드물게 2형 당뇨에서도 케톤산증이 발생할 수 있다는 보고가 있어서 당뇨를 가진 환자들에게는 주기적 혈당 확인이 필요하다[17]. 또한 뇌하수체의 염증반응으로 인해 발생하는 뇌하수체염은 드물게 발생하지만 발생하면 매우 치명적일 수 있다. CTLA-4 inhibitor와 PD-1 inhibitor의 병합치료에서 6.4%, CTLA-4 inhibitor 단독 치료에서 3.2%, PD-1 inhibitor에서는 0.4%로 보고되고 있다[18]. 피로감 등의 비특이적인 증상에서부터 두통, 오심, 어지럼증, 시력감소, 무월경 등의 증상을 보일 수 있다. 이러한 증상을 보일 때는 혈액검사에서 부신피질자극호르몬, 갑상선자극호르몬, 황체형성호르몬, 난포자극호르몬, 프로락틴, 테스토스테론, 에스트라다이올과 같은 뇌하수체 관련 호르몬 검사를 시행하고 뇌전이와 감별하기 위해서라도 뇌 자기공명영상 검사를 시행해야 한다. 갑상선기능저하와 마찬가지로 뇌하수체기능저하가 발생했다면 이 또한 장기적 호르몬 치료가 필요하게 된다.
3. 호흡기계 부작용
면역항암제로 인해 발생하는 폐렴은 CTLA-4보다는 PD-1/PD-L1 inhibitor에서 더 많다. grade 3 부작용은 1-2%이지만 심각한 폐렴 발생으로 약제를 영구 중단한 경우는 0.2-4.0%, 이로 인해 사망에 이르게 된 경우가 0.5%로 보고되고 있다. 발생 시기와 부작용의 정도 또한 다양하게 나타나기 때문에 주의를 요한다[19]. grade 1은 증상은 없고 영상검사의 변화만 있는 것으로 면역항암제 투여를 연기하고 2-3일 경과를 지켜볼 것을 권고한다. grade 2는 호흡곤란, 기침, 흉통 등이 새로이 발생하고 증상의 강도가 경미한 정도를 말한다(Figure 3). 면역항암제 투여를 중지하고 48시간 뒤에도 증상의 호전이 없으면 prednisolone을 경구약(1 mg/kg/day)으로 복용할 것을 권고하고 있다. 물론 이 경우에 감염은 배제되어야 할 것이다. 스테로이드는 4-6주에 걸쳐서 천천히 감량하고 하루에 10 mg 정도로 조절이 되면, 면역관문억제제 투여 재사용을 신중하게 고려하라고 권고하고 있다. grade 3-4는 심한 호흡곤란, 저산소혈증을 보이는 경우로 입원이 필요하고 high resolution computed tomography(HRCT)와 필요 시 기관지 내시경 및 기관지폐포세척(Bronchoalveolar lavage) 검사를 권고한다. HRCT의 면역 관련 부작용 폐렴의 특이적인 양상은 없고 ground glass opacities, cryptogenic organizing pneumonia-like appearance, interstitial pneumonia pattern 등을 보일 수 있다. 기관지 내시경을 통한 기관지폐포세척 검사에서 lymphocytic cellular pattern을 보이고 조직검사에서 diffuse lymphocytic infiltrates를 볼 수 있겠다. 치료는 예방적 항생제를 사용하면서 (methyl)prednisolone (2-4 mg/kg/day intravenous [IV])을 사용하고 필요 시 인공호흡기 치료를 하라고 되어 있다. 고용량 스테로이드 치료에도 반응이 없을 경우 다른 면역억제제인 infliximab, mycophenolate, cyclophosphamide를 사용해 볼 것을 추천한다[3].

The patient with non-small cell lung cancer was treated with nivolumab. After two cycles, dyspnea and dry cough developed. The final diagnosis was grade 2 immune related pneumonitis secondary to nivolumab use. (A) Before nivolumab, (B) after two cycle of nivolumab, (C) before nivolumab, and (D) after two cycle of nivolumab. Informed consent for publication of the clinical images was obtained from the patient.
4. 위장관계 부작용
위장관계 부작용은 CTLA-4 inhibitor에서 흔히 보고되고 있고(27-54%), 설사가 가장 많다. 하루 7회 이상의 설사를 하는 경우 grade 3/4의 부작용 정도로 보고 복부 CT, sigmoidoscopy로 검사를 하고 (methyl)prednisolone (1-2 mg/kg/day IV)을 3-5일간 사용하면서 치료할 수 있다. 치료에도 불구하고 호전이 없을 경우에는 infliximab 5 mg/kg/day 1회 또는 2주 뒤 반복 투여로 치료해 볼 수도 있다. Ipilimumab을 사용한 악성흑색종 연구에서 대장 천공이 1-1.5%로 발생하였다. 복통, 설사, 혈변 등을 보일 때 주의를 요하고 위장관 부작용은 다른 부작용과 병합되어 발생할 수도 있기 때문에 피부발진, 관절염, 간염, 췌장염이 같이 동반될 수 있음도 살펴보아야 한다[20].
5. 간독성
PD-1/PD-L1 inhibitor로 인한 간염 또한 그 빈도는 매우 적다(5-10%) [21]. 간기능 검사에서 aspartate aminotransferase 혹은 alanine aminotransferase 수치가 정상의 3-5배 상승(혹은 >120-200 U/L)일 경우 grade 2의 독성으로 면역항암제 투여를 중지하고 스테로이드 치료를 고려하라고 권고한다. Aspartate aminotransferase/alanine aminotransferase가 정상 수치의 5-20배의 grade 3(혹은 >200-800 U/L), 정상 수치의 20배(혹은 >800 U/L)인 grade 4의 경우에는 약제의 영구 중지와 (methyl) prednisolone (1-2 mg/kg/day IV)으로 2-3일 경과관찰 후 호전이 없을 경우 mycophenolate mofetil로 치료할 것을 권고하고 있다[3]. grade 2 이상의 부작용 발생 시 영상검사와 간 조직검사를 시행해 볼 수 있다[21].
6. 근골격계 부작용
경한 근육통과 관절통은 2-12%에서 흔히 볼 수 있고, PD-1 inhibitor를 사용한 경우 더 잘 볼 수 있다[22]. 경한 관절통에는 비스테로이드성소염제로 치료를 시작해 볼 수 있고, 증상 호전이 없을 경우에는 저용량의 prednisone (10-20 mg)으로 치료해 볼 수 있다. 관절염, 혈관염은 매우 드물게 보고되고 있는데 심한 관절염으로 통증이 심할 경우에는 류마티스내과에 협진을 구해야 하고 1 mg/kg/day의 스테로이드 치료를 시작해야 하는 것으로 권고하고 있다[3].
7. 신경계 부작용
신경계 부작용은 드물게 발생하지만 치명적인 결과를 초래할 수 있기 때문에 주의를 요한다. 보고에 따르면 CTLA-4 inhibitor에서 3.8%, PD-1 inhibitor에서 6.1%로 병합 치료에서는 12% 독성이 증가함을 보였다[5]. 신경학적 부작용이 나타나면 약제를 중지하고 자기공명영상, lumbar puncture 등을 통해 진단을 하고 고용량 스테로이드 치료를 시작해야 한다. 심각한 정도의 기엥-바레증후군(GuillainBarré syndrome)이나 myasthenia-like symptoms 경우에는 plasmapheresis 또는 정맥용 면역글로불린 치료를 고려해야 한다[3].
결론
과거의 세포독성항암제와는 다른 면역관문억제제는 우리 몸의 면역세포를 통해 암을 치료하는 새로운 개념으로 현재 활발히 사용되고 있다. 부작용 측면에서도 과거 독성이 심한 항암제보다 더 우수하기 때문에 많은 암 환자들의 삶의 질 측면에서도 도움이 된다. 하지만 임상에서 실제 사용 역사가 짧고 경험치의 축적이 적기 때문에, 대부분 경한 부작용으로 조절이 가능하다고는 하나, 과거 경험하지 못한 전혀 새로운 부작용의 종류와 강도를 맞이할 수 있다. 또한, 면역 부작용의 위험인자, 악화요인, 예후에 대한 연구가 거의 없어서 현재로서는 명확히 알 수 없기에, 약제를 사용함으로써 발생할 수 있는 부작용을 미리 잘 이해하고 숙지하여 조기에 환자들의 변화를 인지하는 것이 무엇보다 중요하리라 여겨진다.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.