비부비동염의 분류, 진단 및 치료
The classification, diagnosis, and treatment of rhinosinusitis
Article information

Trans Abstract
Background
Rhinosinusitis, one of the most common conditions encountered by clinicians, affects quality of life and reduces work productivity. Despite its high prevalence and economic burden, there are considerable differences in practice regarding the management of rhinosinusitis. Based on many studies, including the updated guidelines, classifications have been subdivided, and new treatments have been added.
Current Concepts
Rhinosinusitis can be classified as acute rhinosinusitis (ARS) or chronic rhinosinusitis (CRS) with a cut-off duration of 12 weeks. It is diagnosed based on subjective symptoms and objective findings on computed tomography or endoscopy. Viral infections account for the majority of the causes of ARS, with watchful waiting without antibiotics as its important initial management. Meanwhile, CRS is divided into primary and secondary CRS, which is further subdivided by anatomic distribution and endotype. Particularly, the Type 2 endotype is characterized by a high recurrence rate and high resistance to current therapies. Biologics using monoclonal antibodies could therefore be used as new therapeutic options for the treatment of primary type 2 CRS. Furthermore, given the chronicity of CRS, it is important to recognize that endoscopic sinus surgery and continuous postoperative medical treatment are important for its management.
Discussion and Conclusion
Accurate diagnoses based on diagnostic criteria and subdivided classifications are necessary to determine the treatment plan and prognosis. In particular, it is important to differentiate the endotype of CRS and provide appropriate treatments to improve the patient’s symptoms and quality of life.
서론
비부비동염은 비강과 부비동의 염증 상태를 일컫는 말로 예전에는 부비동염이란 용어를 흔히 사용하였지만 부비동염이 있는 경우 비강에도 동시에 영향을 미치기 때문에 지금은 대부분 비부비동염이라고 표기한다[1]. 비부비동염은 유병기간에 따라 크게 급성과 만성으로 분류할 수 있다. 갑자기 발생하여 12주 미만의 증상기간을 나타내는 경우 급성 비부비동염(acute rhinosinusitis, ARS), 증상이 12주 이상 지속되는 경우 만성 비부비동염(chronic rhinosinusitis, CRS)으로 정의한다. ARS의 연간 유병률은 6-15%, CRS는 5-12%로 보고된다. 국내에서 실시한 2008년 국민건강영양평가에 의하면 성인에서 CRS의 유병률은 8.4%로 보고되며, 전 세계적으로 유병률이 점점 증가하고 있다[2]. 비부비동염은 삶의 질에 막대한 영향을 미치는 질환으로, 특히 ASR보다 CRS에서 더욱 심한 것으로 알려져 있다[3]. 비부비동염에 대한 보건의료 지출은 다른 질환에 비해 매우 큰 편이며, 미국에서 CRS 질병관리에 관련된 간접 비용을 포함한 전체 비용이 모든 질병을 통틀어 10위 안에 드는 것으로 추정된다[4]. 이와 같이 유병률이 증가하면서 사회적 관심이 높아지고 있고 또한 최근 몇 년간 비부비동염 중 특히 CRS의 개념과 분류, 치료에 있어 많은 변화가 있어 정리해 보고자 한다.
증상 및 진단기준
비부비동염의 임상적 진단은 두 가지 이상의 주관적 증상과 한 가지 이상의 객관적 소견을 만족하는 경우 진단할 수 있다(Table 1) [5]. 코막힘, 콧물, 안면통이나 후각 저하의 4가지 증상 중 2가지 이상의 증상을 동반해야 하는데 그 중 반드시 한 가지 증상은 코막힘이나 콧물 증상 중 하나를 포함해야 한다. 콧물 증상은 앞으로 흐르는 콧물뿐만 아니라 후비루 증상이 포함될 수도 있고, 소아의 경우 성인과 달리 후각 저하에 대한 표현이 어려울 수 있으므로 후각 저하 대신 기침 증상을 포함할 수 있다. 비용종 유무에 따라 CRS 환자군을 나누어 비교해 보았을 때 비용종이 없는 경우 코막힘을 가장 많이 호소하였고, 비용종을 동반한 경우 특히 후각 저하를 심하게 호소하는 경향을 보였다[6,7]. CRS의 경우 흡연자에서 더 흔하게 발생하고 많은 환자에서 음주로 인해 증상이 악화되는 것으로 보고된다[8]. CRS 환자의 25%에서 천식을 동반한다고 하며, 그 외 위식도역류병, 만성폐쇄폐질환 등과도 연관된 것으로 알려져 있어 동반 증상 여부도 확인하는 것이 필요하다.

Definitions of rhinosinusitis
증상과 함께 내시경 또는 컴퓨터단층촬영(computed tomography, CT)에서 이상소견이 있는 경우 최종적으로 비부비동염이라 진단할 수 있다. 내시경 소견에서 비용종 혹은 중비도의 부종이나 점액 화농성 분비물이 확인되는 경우 또는 CT에서 부비동이나 개구비도 복합체(ostiomeatal complex)의 점막변화가 있는 경우 진단할 수 있다(Figure 1). Water’s view, paranasal sinus view 등을 촬영하여 부비동을 확인하는 방법도 있으나, 현재 사용되는 진단기준에서 simple x-ray 소견은 포함되지 않는다. 내시경 소견이나 CT 소견 없이 증상만으로 진단할 경우 알레르기 비염이나 비알레르기 비염과 증상이 중복되어 유병률이 과도하게 증가할 수 있으므로 주의해야 한다[9,10]. 실제 증상만으로 진단한 경우 유병률은 5.5-28%로 다양하고 높게 나타났지만, 내시경이나 CT 소견을 포함하여 진단한 경우 CRS의 유병률은 3-6%로 보고되었다[11,12].

Representative endoscopic signs of rhinosinusitis. (A) Multiple nasal polyps are shown in right nasal cavity. (B) Purulent discharge drains from the right middle meatus into the nasopharynx. (C) Mucosal edema is shown in the right middle meatus.
급성 비부비동염
1. 분류
ARS는 크게 3가지로 나눌 수 있다, 흔히 감기(common cold)라고 이야기하는 viral ARS, 감기가 2주 이내에 완전히 낫지 않고 지속되거나 악화되는 경우를 post-viral ARS, 2차적 세균 감염이 발생한 경우는 acute bacterial rhinosinusitis (ABRS)라고 한다(Figure 2) [13]. Postviral ARS의 유병률은 약 18%이며, 증상발현 5일 경과 후에도 증상의 악화가 명확히 나타나는 경우가 아니라면, 증상발현 10일 이전에 post-viral ARS를 진단하는 것은 피해야 한다. ABRS의 유병률은 0.5-2%로 알려져 있으며 Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis, Staphylococcus aureus가 대표적인 원인균이다[14]. 38도 이상의 열을 동반하거나 콧물의 색이 변하는 경우, 심한 국소적 안면통이나 두통을 동반하는 경우, erythrocyte sedimentation rate (ESR)/C-reactive protein (CRP)가 증가된 경우, 증상이 호전되다가 다시 악화되는 양상을 보이는 경우, 이 5가지 중 3가지 이상의 소견을 보일 때 경우 ABRS를 의심할 수 있다[15].
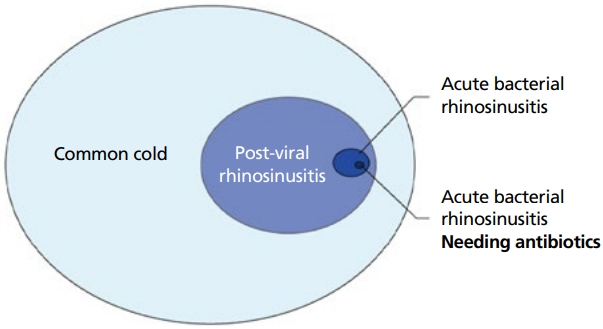
The incidence of different forms of acute rhinosinusitis (ARS). Common cold, post-viral rhinosinusitis and acute bacterial rhinosinusitis (ABRS). Antibiotics are only indicated in a small part of the patients with ABRS. Adapted from Fokkens WJ, et al. Rhinology 2020;58(Suppl S29):1-464, according to the Creative Commons license [13].
2. 진단
앞서 기술한 바와 같이 증상과 더불어 비내시경이나 CT에서 이상소견 확인 시 ARS를 진단할 수 있는데, CT는 대개 치료에 반응이 없거나 합병증이 의심되는 경우 촬영한다[16]. ABRS가 의심되는 경우 혈액검사로 ESR/CRP 증가를 확인해 보는 것이 도움이 될 수 있으며, 경험적 항생제 사용에도 호전이 없는 경우에 ABRS의 정확한 원인균을 확인하기 위해서 부비동 천자를 통한 균 배양검사가 필요하다. 그러나 이는 침습적이고 통증을 동반하는 검사이므로 부비동 천자 대신 중비도에서 농을 채취하여 배양할 수 있다.
3. 치료
Viral ARS의 치료는 성인과 소아 모두 대부분 증상치료로 충분하다. 생리식염수 비강세척, 항히스타민제, 비충혈 제거제(nasal decongestants), 진통제 등을 사용할 수 있다. Post-viral ARS 치료는 비강세척과 함께 필요하다면 증상 완화를 위해 성인에서 비강스테로이드를 사용할 수 있고, ABRS 환자에서 항생제가 필요한 경우가 있지만 Figure 1과 같이 항생제를 필요로 하는 ABRS 환자의 비율은 매우 적다. 따라서 증상치료를 하며 질병의 경과를 주의 깊게 관찰하되, 항생제는 제한적으로 사용해야 한다는 것이 중요하다. 항생제를 처방해야 하는 경우 경험적 항생제로 amoxicillin보다는 amoxicillin-clavulanate가 1차 약제로 권고되며 대개 복용 3일째 증상 호전 효과가 나타난다[17]. S. pneumoniae에 내성이 있는 지역이나, 심한 염증, 한달 이내 항생제 사용 병력이나 입원력이 있는 경우, 면역저하 환자의 경우에서는 amoxicillin-clavulanate 2배 용량을 사용하는 것이 권고된다. Penicillin 알레르기가 있는 환자에서는 doxycycline이나 fluoroquinolone를 대신 처방할 수 있고, 또는 3세대 세팔로스포린과 클린다마이신 복합용법을 처방할 수 있다. 항생제 처방 기간은 성인에서는 5-7일, 소아에서는 10-14일 처방한다. ABRS가 잘 치료되지 않고 진행하는 경우 심각한 합병증을 유발할 수 있고, 합병증 발생 시 빠른 진단을 위해 항상 면밀한 주의가 필요하다. 그럼에도 불구하고 많은 연구에서 항생제 사용으로 합병증이 예방되지는 않았기 때문에 ABRS 환자에서 항생제는 제한적으로 사용해야 한다[18]. 합병증으로는 안와주위염, 안와봉와직염, 골막하농양, 안와농양, 해면정맥동혈전 등과 같은 안와내 합병증 및 경막하농양, 경막외농양, 뇌막염, 뇌농양과 같은 두개내 합병증이 발생할 수 있다. 그 외에 골수염이나 상안와염 증후군 및 안와첨 증후군을 일으키기도 한다. 합병증 발생 시에는 뇌혈관장벽을 통과하는 광범위 항생제를 사용하며, 항생제 치료에 호전이 없으면 수술적 배농이 필요한 경우 수술을 시행해야 하는데 한 연구에서 안와합병증의 약 55%에서 수술적 치료가 필요하다고 보고하였다[19].
만성 비부비동염
1. 분류
CRS는 비부비동염 증상이 12주 이상 지속되는 경우를 말하며, 전통적으로 표현형에 따라 비용종이 없는 만성 비부비동염(chronic rhinosinusitis without nasal polyps, CRSsNP), 혹은 비용종을 포함한 만성 비부비동염(chronic rhinosinusitis with nasal polyps, CRSwNP)으로 나뉘고, 이 두 가지 표현형을 기준으로 원인과 진단, 그리고 치료를 구분하였다. 일반적으로 CRSsNP의 경우 ABRS가 완전히 치료되지 않은 결과 만성화되어 CRS가 된다고 가정하여 주 치료로 다양한 항생제가 연구되었고, 이와 달리 CRSwNP은 발병기전이 allergy와 관련 있는 것으로 생각되어 corticosteroid가 주 치료제로 소개되었으며, 이러한 약물치료가 실패할 경우 수술적 치료를 시행하였다. 그러나 지난 20여 년간의 연구결과를 통해 이러한 가정은 지나치게 단순한 것임을 알게 되었고, 최근 CRS는 다양한 환경 요인과 숙주의 면역체계 사이에서 상호작용의 기능장애로 인해 발생하는 다인성 병인을 가진 증후군으로 이해된다. CRS의 치료를 위해 환경적 요인에 기반하여 곰팡이, S. aureus, 세균총과 같은 원인 미생물의 직접적인 치료는 실제 임상에서 효과가 미미하였고, 숙주 요인에 기반한 유전연구는 비실용적이었다. 따라서 최근에는 부비동 점막에서 나타나는 염증반응에 집중하게 되었고, 이는 내재형(endotype)을 밝히는 것에 초점을 두고 있다[20]. 내재형에 따른 연구들이 축적되면서 CRS는 서로 다른 병태생리를 가지는 복잡한 질환으로 이해되고 있다. 표현형에 따른 기존의 분류는 이러한 분자 생물학적인 병태생리 기전을 반영하기에 충분하지 않아 새로운 분류의 필요성이 대두되었고, 2020년 European position paper에서는 CRS의 분류 및 치료에서 큰 변화가 있었다[13]. CRS를 원발성과 이차성으로 나누고, 각각을 질병의 해부학적 분포 정도와 내재형에 따라 나누는 새로운 분류법을 제시하였다(Table 2).

Classification of CRS
원발성 CRS는 우선 일측성인지 양측성인지에 따라 분류하고 내재형에 따라 제2형 염증인지 아닌지(type 2 or non-type 2 inflammation) 구분한다. 일측성 type 2 CRS의 대표적인 예는 알레르기성 진균성 비부비동염(allergic fungal rhinosinusitis, AFRS)이 있다. 일측성의 non-type 2 CRS는 isolated sinusitis로 일반적인 CRS가 포함된다. 양측성 CRS 중 type 2 염증의 특징을 가지고 있는 대표적인 질환은 CRSwNP, eosinophilic CRS (eCRS), AFRS, 중심구획 알레르기질환(central compartment allergic disease)이 있고, 그 외의 다른 나머지 양측성 CRS는 non-eCRS를 포함하여 대부분 non-type 2 inflammation에 포함된다. Type 2 염증은 특징적으로 innate lymphoid cell 2와 helper T cell 2 (Th2 cell)가 활성화되고, 인터루킨(interleukin, IL)-4, IL-5, IL-13 사이토카인이 매개하는 반응으로서 호산구와 비만세포가 출현하고 활성화된다. 치료에 저항성이 있는 경우가 많아 치료가 어렵고 높은 재발률을 보이는 특징을 가진다. 각 표현형에 따라 내재형을 확인한 연구에 따르면 CRSwNP에서 type 2 염증이 87%로 높게 나타났지만, CRSsNP에서도 55%의 비율로 절반이 넘는 환자가 type 2 염증을 나타내었다[21]. 천식과 아스피린 과민성을 동반한 환자에서도 type 2 염증이 특징적으로 나타난다.
이차성 CRS는 일측성인 경우 치성 비부비동염(odontogenic sinusitis), 진균성 비부비동염(fungal sinusitis), 종양에 의한 비부비동염 등이 있고, 양측성인 경우 일차성 섬모장애(primary ciliary dyskinesia), 낭종성 섬유증(cystic fibrosis), 육아종성 혈관염(granulomatosis with polyangitis, GPA), eosinophilic GPA 등이 원인이 되어 비부비동염이 발생할 수 있다.
2. 진단
CRS의 진단은 앞서 기술한 바와 같이 특징적인 2가지 이상의 증상과 함께 내시경이나 CT에서 비부비동염 의심소견이 있으면 진단할 수 있는데, 전반적으로 CT가 gold standard 검사로 여겨지며 최근 low dose multi-detector CT나 conebeam CT가 방사선량이 적고 시간이 절약되면서 해부학적 정확성은 유지되어 점점 선호되고 있다[22]. 또한 eCRS는 상악동보다 사골동의 염증이 더 심한 경향을 보이는 특징이 있으므로 CT 소견이 내재형을 파악하는 데 도움이 된다[23].
CRS 환자에서 조직학적 검사는 최근 내재형 분류가 강조되면서 중요성이 높아지고 있다. 부비동 점막에서 호산구의 분포비율이나 type 2 염증반응에서 우세한 사이토카인의 분포를 확인할 수 있다. 대개 고배율 시야에서 호산구가 10개 이상이면 eCRS로 진단할 수 있다. 호산구 침윤의 정도나 전반적인 염증 상태는 질병의 경과와 중증도와 밀접한 관련이 있는 것으로 생각된다[24].
혈액검사에서 CRS와 직접적으로 관련된 특정 marker는 아직 알려진 것이 없으나 GPA, eosinophilic GPA 또는 면역저하가 의심되는 환자에서 감별진단을 위해 c-ANCA, proteinase 3의 검사를 시행할 수 있다. 또한 최근 각광받고 있는 생물학적 제제(biologics) 치료의 적응증 확인을 위해 호산구, IgE 등의 검사가 이용될 수 있다.
3. 치료
European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS) 2020에서는 분류 체계가 바뀌었듯, 이전과 달리 CRSsNP와 CRSwNP를 구분하여 치료하지 않는다. 2021년 미국에서 발표된 International Consensus Statement on Allergy and Rhinology에서는 여전히 CRSsNP와 CRSwNP를 구분하여 치료방침을 안내하고 있지만, EPOS 2020의 분류에 맞추어 치료를 소개하고자 한다.
예전에는 CRS 증상 호전을 위해 약물치료에 실패하면 수술적 치료를 하는 것으로 생각했지만, 최근 CRS의 치료 개념은 꾸준한 관리가 필요한 만성질환이며, 부비동 내시경 수술은 이러한 관리의 한 단계로서 국소 약물 전달을 용이하게 하기 위한 하나의 방법으로 생각한다. 즉, 수술이 치료의 끝이 아니라 치료의 한 과정이며, CRS는 수술 후에도 지속적인 관리가 필요한 질병임을 인지하고 있어야 한다.
CRS의 기본치료는 비강세척과 스테로이드 비강 스프레이다. 급성 악화 소견을 보이는 경우일지라도 ARS와 마찬가지로 CRS에서 항생제 사용은 효과가 미미하기 때문에 자제해야 한다. 비강세척은 CRS의 증상 개선과 점액 감소에 도움을 주고, 대개 실온의 등장성 생리식염수로 시행하며 200 mL 이상의 용량을 사용할 것을 권유한다[25]. 비강스테로이드 스프레이는 많은 연구를 통해 삶의 질 개선과 증상 호전에 효과적인 것이 증명되었으며, 장기간 사용에도 안전하고 소아에서도 성장에 영향을 미치지 않는다고 보고되어 필요 시 권유할 수 있다[26]. 비강세척과 스테로이드 비강 스프레이 사용 6-12주 후에도 호전이 없다면 일측성인지, 양측성 인지에 따라 치료방향이 달라진다.
일측성인 경우 CT를 촬영하여 원인이 되는 질환이 있는지 확인하고 원인치료를 병행한다. 진균성 비부비동염의 경우 수술적 치료가 필요하고 치성 비부비동염도 대다수에서 부비동 내시경 수술이 필요하며 동시에 원인 치아의 치료가 반드시 동반되어야 재발을 예방할 수 있다[27]. 종양에 의한 비부비동염은 종양에 대한 검사를 진행한다. 특정 원인이 없는 경우에도 약물치료로 호전이 없으면 수술적 치료를 시행할 수 있다.
양측성 비부비동염 증상을 호소하는 경우 type 2 CRS와 non-type 2 CRS를 구분하여 치료한다. Type 2 CRS의 경우 기본치료에 추가적으로 경구 스테로이드제를 단기간 사용하면 효과적인 경우가 많다. 그러나 경구 스테로이드제를 자주 반복적으로 사용하게 되는 경우 수술을 고려하거나 다른 추가치료를 고려할 수 있는데, 아스피린 과민성 환자에서는 아스피린 탈감작 요법이 도움이 될 수 있고, 또 다른 치료 중 하나는 최근 각광받고 있는 생물학적 제제이다. Type 2 CRS 환자는 치료에 잘 반응하지 않고 수술 후에도 반복적으로 재발하는 특징을 나타내어 기존 치료 외에 새로운 치료가 요구되었다. Type 2 CRS에서 우세하게 분포되어 있는 사이토카인 IL-4, IL-5, IL-13 또는 IgE을 억제하는 monoclonal antibody를 이용한 치료가 시도되었고, 여러 연구를 통해 증상 호전에 효과적인 것이 입증되었다. 2019년 IL-4 수용체 억제제인 dupilumab을 CRSwNP 환자에서 사용할 수 있도록 미국 식품의약국 승인을 받았고 국내에서도 2021년 3월부터 CRS 환자 치료를 위해 식품의약품안전처에서 dupilumab 사용을 승인하였다. 반복적인 경구 스테로이드의 사용을 감소시키고 다른 치료와 비교하여 특히 후각 호전에 효과적인 것으로 나타났다[28]. 그러나 비용이 비싸고 사용기간에 대한 합의가 이루어지지 않아 표준 처방지침이 아직은 부족한 실정이며, 장기간 연구가 되어있지 않아 치료 종료 후 얼마나 효과가 지속되는지 불분명하다는 단점이 있다. 또한 치료 반응을 예측하거나 type 2 CRS와 직접적으로 연관된 biomarker는 아직까지 발견되지 않았다. 그럼에도 불구하고 반복적인 치료, 수술에도 증상 호전이 없는 환자에서 적용해 볼 수 있는 효과적인 새로운 치료라는 점에서 충분히 주목할 만하다. Non-type 2 CRS의 경우는 기본치료에 호전이 없는 경우 장기간 저용량 마크롤라이드(macrolide)를 항염증 효과를 위해 사용할 수 있다. IgE 수치가 낮은 환자에서 사용할 경우 더 효과적인 것으로 보고되며 대개 12주 정도 사용한다. 이러한 약물치료에도 효과가 없으면 수술을 고려할 수 있다.
결론
비부비동염 환자의 치료를 위해 진단기준과 세분화된 분류에 따라 정확한 진단을 내리는 것이 치료방향을 결정하고 예후를 예측하는 데 중요하다. 과거 ARS에서 쉽게 항생제를 처방하고, CRS에서 약물치료에 효과가 없으면 쉽게 부비동 수술을 시행했지만, 많은 연구를 바탕으로 여러 차례 진료지침이 업데이트되면서 분류가 세분화되고 치료방향이 바뀌거나 새로운 치료가 추가되었다. ARS는 대부분이 바이러스 감염에 의해 발생하기 때문에 증상치료로 충분하지만, ABRS 합병증 발생 시에는 빠르게 항생제를 투여하는 것과 동시에 질병의 진행 상황을 주의 깊게 관찰해야 한다. 최근 CRS는 내재형에 따른 분류가 치료에 있어서 중요한 요인으로 생각되고 특히 치료에 잘 반응하지 않고 재발이 잦은 내재형인 type 2 CRS는 꾸준히 관리해야 하는 만성 질병, 또는 하나의 증후군으로 생각된다. 이러한 환자에서 부비동 수술에 대한 인식은 최종 치료가 아닌 국소 약물 전달을 용이하게 하는 관리의 한 단계로 전환되었다. 따라서 환자의 내재형을 감별하여 적절한 치료를 선택하고 꾸준한 관리를 통해 환자의 증상 개선과 함께 삶의 질을 향상시킬 수 있도록 해야 한다.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
References
Peer Reviewers’ Commentary
이 논문은 알레르기 비염과 함께 국내에서 유병률이 증가하고 있는 급성 및 만성 비부비동염의 분류, 진단 및 치료에 대해 최신 문헌을 토대로 자세히 기술하고 있으며, 바뀐 분류 체계와 최신 진료지침에 대해서 일목요연하게 정리하여 설명해 주고 있다. 비부비동염의 치료에 있어서는 항생제의 제한적 사용 필요성과 부비동 내시경수술의 축소된 역할, 그리고 생물학적 제재의 효용성에 대해 잘 설명하고 있다. 또한 type 2 만성 비부비동염이 단기적인 치료로 해결되기를 기대하기보다는 고혈압이나 당뇨병과 같은 다른 만성 질환처럼 꾸준히 관리해야 하는 대상인 것임을 잘 강조하고 있다. 이 논문은 재발이 잦고 완치가 어려운 만성 비부비동염을 진료하는 임상 현장에 많은 도움을 줄 것으로 판단된다.
[정리: 편집위원회]